
Abstract
Nasal myiasis is a nasal infestation caused by myiasis, a parasitic disease affecting the nasal cavity. It is a rare condition. The nasal cavity is in close proximity to the sinuses, eyes, and cranial cavity. If the fly larvae migrate into this location, it may result in significant complications. The prompt and appropriate removal of maggots and the administration of an efficacious treatment can effectively prevent further deterioration of the disease. In this case study, we present the case of a 55-year-old woman who was admitted to the intensive care unit with severe respiratory failure. On the fourth day following admission, the patient remained unconscious, and several white larvae emerged from the nasal cavity. Through identification, the larvae were determined to be Musca domestica larvae. Subsequently, saline irrigation was performed under nasal endoscopy, and anti-inflammatory therapy was administered to the patient to prevent intracranial infection. Following treatment, the patient’s symptoms were effectively managed, and the prognosis remained favorable until the 1-month follow-up. This case report presents a literature review of the reported cases of nasal myiasis caused by M. domestica and discusses the susceptibility factors and treatment modalities for nasal myiasis.
Introduction
Nasal myiasis is defined as an infestation caused by the invasion of dipterous fly larvae into the living tissues of humans or other mammals.1,2 The flies deposit their eggs in open wounds or natural cavities, which then hatch into larvae. This disease, initially documented by Lelean in 1904, can affect individuals of all age groups.3,4 In China, myiasis is most commonly observed in agricultural and animal husbandry regions, particularly in warmer areas of South China, with fewer cases reported in North China. 5 The clinical manifestations of human myiasis vary depending on the location of the parasites. These can include the ocular, oral, nasopharyngeal, auricular, gastrointestinal, urogenital, cutaneous, traumatic, and other visceral areas.6,7 Cutaneous myiasis is the most prevalent form, while nasal myiasis is less common. 5
This study presents a case of respiratory failure in a patient admitted to the Department of Intensive Care Unit (ICU) at the First Central Hospital of Tianjin, which was complicated by the presence of nasal myiasis. This case was approved by the Ethics Committee of the First Central Hospital of Tianjin (Approval No. BL202403), and the patient signed an informed consent form authorizing the reporting of this case. The treatment approach, infection prevention strategies, and control measures are discussed, with the aim of enhancing medical professionals’ understanding of myiasis and emphasizing the importance of vigilance toward this condition.
Case presentation
A 55-year-old woman was admitted to the ICU of Tianjin First Central Hospital with intermittent dizziness and nausea of 7 days’ duration and impaired consciousness of 3 days’ duration. The patient was admitted to the hospital 7 days ago for unexplained dizziness and nausea. They subsequently sought medical advice from a local physician and were prescribed medication. However, details regarding the specific medication and dosage are unknown. The medication had no beneficial effect. The patient’s level of consciousness declined over a period of 3 days before she was admitted to an external medical facility for in-patient treatment. Unfortunately, the treatment administered at the facility was unsuccessful in improving the patient’s condition. The patient presented with severe respiratory failure 24 h earlier, requiring intubation and mechanical ventilation for respiratory support. The family decided to transfer the patient to the ICU of our hospital for further evaluation and management. The patient was born in Tianjin, China, where she has lived for a considerable period of time. She denied any history of travel, surgery, or trauma, and also reported no family history of infectious or genetic diseases.
The patient presents with a temperature of 39.2°C, a heart rate of 135 beats per minute, a respiration rate of 32 breaths per minute, and a blood pressure of 146/85 mmHg. The patient displays acute illness symptoms, confusion, and a lack of cooperation during the examination. The nasal shape is observed to be normal, and there is no purulent discharge present within the nasal cavity. The tracheal tube was correctly positioned within the oral cavity, and there was no evidence of tonsillar enlargement. No thoracic deformity was observed, and coarse respiratory sounds were audible in both lungs, accompanied by the presence of wet rales. Upon admission to the hospital, the patient was diagnosed with respiratory failure and pneumonia based on their medical history, clinical symptoms, and pre-admission laboratory tests and examinations. Upon admission, the patient was in critical condition, necessitating close monitoring of vital signs. Laboratory tests and examinations indicated improvement, leading to the decision to perform endotracheal intubation with ventilator support. Treatment strategies included rehydration, expansion, anti-infection measures, sputum control, gastric acid suppression, gastric protection, and consultation with relevant departments for additional assistance.
On the fourth day following admission, the patient remained unresponsive. In the early morning, several white larvae, measuring between approximately 0.5 and 1 cm in length, were observed emerging from the patient’s nasal cavity (Figure 1(a)). Nasoscopy revealed the presence of white larvae within the nasal cavity (Figure 1(b)). The nasal cavity was flushed with saline, resulting in the expulsion of several white larvae (Figure 2). The larvae were subsequently forwarded to the Parasite Teaching and Research Laboratory of Tianjin Medical University for species identification. After thorough examination, the larvae were identified as belonging to the Musca domestica species, commonly known as the housefly. This conclusion was reached based on the presence of degenerated head structures with claw-like mouth hooks (Figure 3(b)). Additionally, the larvae exhibited the presence of anterior and posterior valves at both ends (Fig. 3(b) and (c)). A computed tomography (CT) examination of the sinuses revealed mild inflammation in the left sphenoid sinus and pterygoid sinus. The diagnosis of nasal myiasis was established based on the patient’s clinical presentation, findings from a nasal examination, and the identification of maggots. Once the diagnosis was confirmed, the patient underwent a 3-day course of debridement and saline rinsing of the nasal cavity, performed three times a day using a nasal endoscope. This procedure was undertaken to clear the larvae and purulent secretions. Furthermore, the patient was administered intravenous meropenem at 8-h intervals for the purpose of preventing intracranial infection.
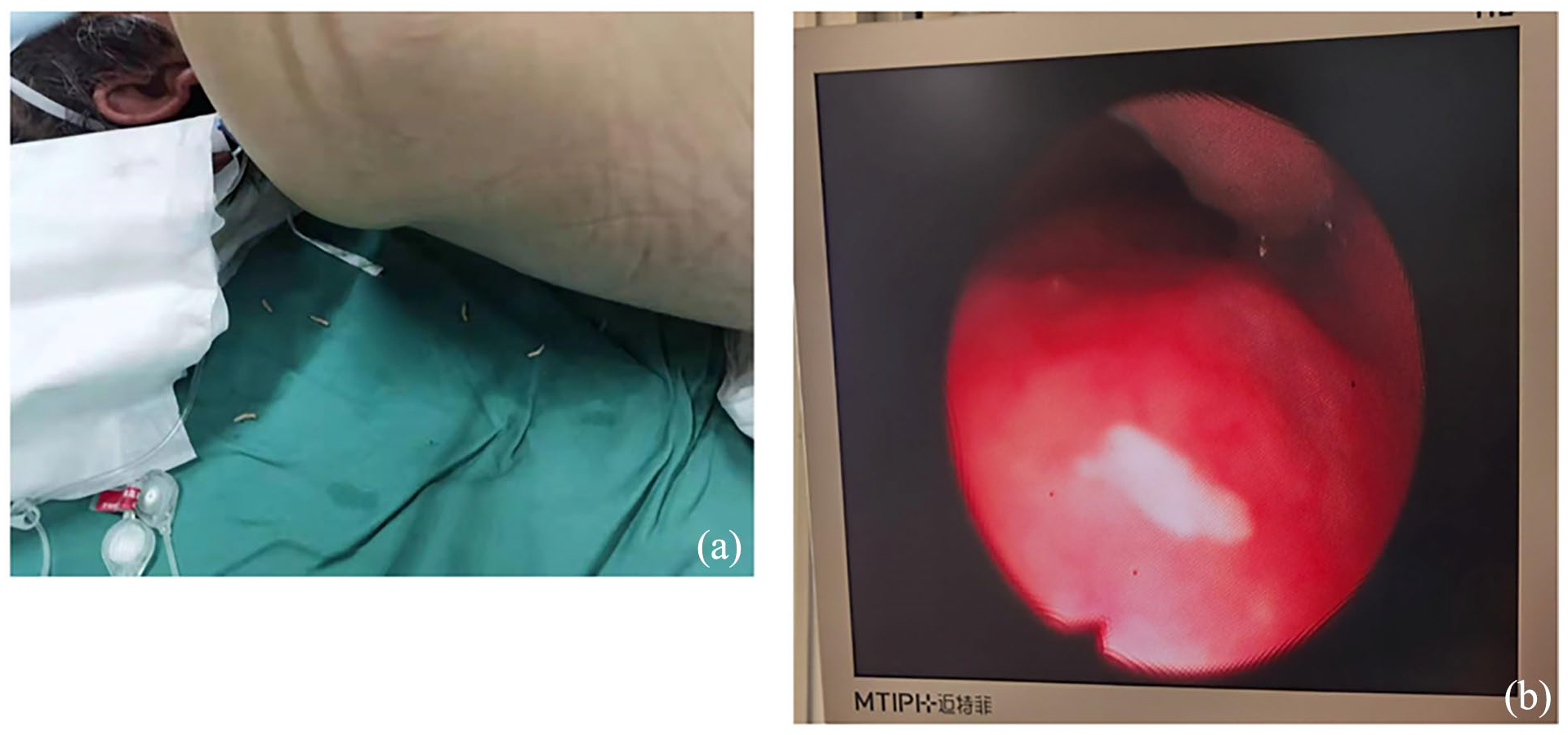
Larvae moved out of the nasal cavity and nasoscopy reveals white worms in nasal cavity. (a) the larvae moved out of the patient’s nasal cavity. (b) Nasoscopy revealed the presence of white larvae within the nasal cavity.

Larvae were flushed out by saline.

Microscopic view of the larvae. (a) General view of the larva. (b) Head features of larvae containing mouth hooks and anterior valves. (c) Caudal features of the larva containing the posterior valve.
Following a 4-day course of treatment, the patient’s symptoms were successfully managed. Subsequent endoscopy examinations conducted during the patient’s hospitalization confirmed the complete removal of maggots from the patient’s nasal cavity (see Supplemental Video). A 1-month follow-up post-discharge indicated a favorable prognosis with the absence of any further adverse symptoms.
Discussion
Myiasis is a disease caused by the infestation of the skin, cavities and wounds by larvae of a wide variety of dipteran flies. 8 Myiasis has a global distribution, though it is more frequently reported in tropical and subtropical regions, as well as in nomadic populations.2,9 Myiasis is a common occurrence in domestic and wild animals, but it is a rare phenomenon in humans. 10 The relationship between the host and the fly maggot larval parasite determines whether myiasis is classified as exclusive parasitism or parthenogenetic parasitism. Specialized parasites feed on live host tissues, whereas parthenogenic parasites tend to feed on cadavers or necrotic tissues, decompose tissues, and occasionally infect humans.2,8 The myiasis induced by specialized parasitism can cause complications due to larvae feeding on healthy tissues, which can be life-threatening in severe cases. 8 Therefore, patients with suspected myiasis should be diagnosed in a timely manner and treated effectively as early as possible.
Myiasis can be classified into various categories based on the location of infection. Among these, cutaneous and ocular myiasis are the most prevalent, while nasal myiasis is less commonly reported. 11 However, due to the proximity of the nasal cavity to the sinuses, eyeballs, and cranial cavity, migration of fly maggots into this location may result in significant complications. Therefore, nasal myiasis should not be overlooked.
Nasal myiasis is most prevalent in patients with chronic rhinopathy, who present with purulent nasal secretions that attract flies to the nasal cavity and induce nasal myiasis.5,12 Nasal myiasis occurs when the female fly deposits her eggs in or near the mucous membrane of the nasal cavity, which is followed by the emergence of the first maggots, which burrow through the tissue. 13 A review of the literature reveals a considerable number of case reports documenting the discovery of maggots, specifically fly maggots, in patients with impaired consciousness following their admission to a hospital.5,7,14 It is notable that the patients in these cases had a history of diabetes mellitus, which is similar to that of the patient in the present case. A review of the literature also reveals that case reports of fly maggot infection in diabetic patients are not uncommon.15–17 This suggests that diabetic patients may be more susceptible to myiasis. In light of these findings, it has been suggested that susceptibility to myiasis in humans may be influenced by a number of factors, including poor hygiene, advanced age, psychiatric illness, rural background, low socioeconomic status, homelessness and diabetes mellitus.2,9 Consequently, the prevention of fly maggots is of particular importance for diabetic patients and individuals with psychiatric illnesses or other factors that may impair consciousness.
Additionally, myiasis may result from poor sanitation in an area with a high fly population. Despite the patient’s long-term residence in Tianjin, but her neighbors were engaged in animal husbandry, and the sanitary environment at home was poor, which could have facilitated the entry of mosquitoes and flies into her nasal cavity. Additionally, the patient was admitted to the hospital with a sinus CT suggestive of sinusitis. At the time of admission, the patient was in an impaired state of consciousness, and her family members were unable to provide a detailed account of her medical history, including whether she had suffered from chronic rhinitis induced by flies parasitized in the nasal cavity or sinusitis due to the flies parasitized in the nasal cavity. On the fourth day following admission to the hospital, approximately 0.5 to 1 cm in length, larvae emerged from the patient’s nasal cavity. Given that the incubation period for fly eggs is 12–24 h and the development of maggots requires approximately two and a half days, it can be inferred that this patient’s infection was acquired outside the hospital.
In the event of a diagnosis of nasal myiasis, prompt intervention is imperative to forestall tissue damage and associated complications. The primary approach to managing myiasis is to remove the larvae. The current treatment options for nasal myiasis include local anesthetic debridement, endoscopic forceps removal, the creation of a toxic and anaerobic environment through the use of turpentine solution to kill and clear the fly larvae, and saline rinses for clearance.18,19 Furthermore, an appropriate anti-infective therapy should be administered based on the patient’s clinical condition. The patient presented with a combination of unconsciousness, respiratory failure, and pneumonia. To prevent the aspiration of foreign matter and the exacerbation of pneumonia, the patient underwent nasoscopic saline rinsing of the nasal cavity three times a day for four consecutive days. Additionally, anti-inflammatory therapy was initiated to avert the potential for intracranial infection. Following a 4-day course of treatment, nasal microscopy demonstrated the complete clearance of maggots from the patient’s nasal cavity. Upon discharge from the hospital, the patient was observed for 1 month, during which time no further adverse symptoms were noted and the prognosis was favorable.
Conclusion
In comparison to the southern and northern pastoral regions of China where fly maggot disease is more commonly reported, Tianjin is situated in the North China Plain where the incidence of this disease is relatively rare. However, this case serves to illustrate that fly maggots can still be contracted in Tianjin due to the high prevalence of flies and poor hygiene practices. It is imperative that healthcare professionals remain cognizant of the potential for myiasis in their daily diagnostic and therapeutic endeavors. In the case of ICU patients, who often present with critical conditions and impaired consciousness, it is of the utmost importance to integrate the clinical manifestations with the individual patient’s circumstances. This integration facilitates the prompt differentiation of myiasis and the implementation of early intervention measures to prevent the deterioration of the patient’s condition.
Footnotes
Acknowledgements
We thank the patient for her agreement to the publication of the report. We are also very grateful to Mr. Hu and other faculty members of the Parasite Teaching and Research Department of Tianjin Medical University for their help in identifying the larvae
Author contributions
H.X. and W.F. contributed to design, write, and final approval of the manuscript. W.L. collected the larvae and revised the manuscript, H.W. performed nasal endoscopy. L.D. was responsible for developing clinical diagnosis and treatment plans for patients. All authors reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tianjin Medical Construction of Key Discipline (Specialty) Funded Project (TJYXZDXK-013A) and Tianjin Science and Tchnology Program (No.21JCYBJC00090 and 22JCQNJC00420) and the National Clinical Key Specially Project Foundation of Ministry of Health in China (grant No. 2011-873).
Ethical approval
We have conducted an ethical approval based on the Declaration of Helsinki at Ethics Committee in Tianjin First Center Hospital (Approval No: BL202403). The Tianjin First Center Hospital Ethics Committee and all of the authors of this report consent to publish this case report.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.