
Abstract
Objective:
This study aims to evaluate the change in attitudes and knowledge about basic cardiopulmonary resuscitation in football professionals following a training intervention and to examine its correlation with sociodemographic variables.
Method:
The study consists of two phases. The first phase involves an observational cross-sectional study to assess the level of attitude and knowledge in cardiopulmonary resuscitation. The second phase includes an educational intervention consisting of a training and practical session on basic cardiopulmonary resuscitation, with a pre-post single-group study. The questionnaire was completed by football professionals from the Spanish first division and their coaches, with N = 206 in the first phase and N = 70, 30 days after the training intervention in the second phase. A possible limitation is that the final sample size is smaller than the initial one; however, it still exceeds the estimated minimum. A two-phase statistical analysis was conducted: a cross-sectional analysis using nonparametric tests (Wilcoxon, Kruskal–Wallis and Spearman) assessed baseline attitude and knowledge in relation to sociodemographic variables, followed by a pre-post intervention analysis using parametric (t-tests, ANOVA, and Pearson) or nonparametric tests depending on data distribution to evaluate intra- and inter-group changes. Normality was tested with the Shapiro–Wilk test and appropriate tests were applied accordingly.
Results:
There is a significant increase (p < 0.001) in the average attitude of participants between before (4.25 ± 0.39) and after (4.40 ± 0.41) the intervention. Knowledge also shows a significant increase (p < 0.001) between before (5.66 ± 1.92) and after (7.60 ± 1.84) the intervention. There is no significant correlation with age, gender, professional category, or levels of knowledge and attitudes.
Conclusions:
The basic cardiopulmonary resuscitation training intervention has proven beneficial, regardless of gender, educational level, or category studied (players/coaches).
Introduction
The high incidence of circulatory system pathologies worldwide necessitates the implementation of protocols and actions to reduce the number of affected individuals and the mortality rate. According to the National Institute of Statistics, 23% of deaths in the first 5 months of 2020 in Spain were due to acute myocardial infarction, with a prevalence in 2021 of 28 cases per 100,000 inhabitants. 1
The incidence of sudden cardiac arrest (SCA) in football players is unknown, but some authors estimate it to be 2.5 times higher than in non-athletes,2,3 making it the leading cause of death in young athletes.4,5 The cases of Spanish first-division professional footballers Dani Jarque and Antonio Puerta marked a turning point in societal perception of such events.6,7 More recent examples include Christian Eriksen in 2020, who was resuscitated by event emergency teams, 8 and Sheffield United Football Club player Maddy Cusack, who died suddenly at age 27 on September 20, 2023. 9
Healthcare systems focus their efforts on reducing these figures mainly through early assistance for these patients and research to optimize the efforts of attending doctors and nurses and find the optimal algorithm that increases the success rate. This involves implementing rapid response protocols, enhancing pre-hospital emergency services, and ensuring the widespread availability of Automated External Defibrillators (AEDs). In addition, continuous medical training and simulation-based education play a crucial role in preparing healthcare professionals to act swiftly and efficiently in cardiac emergencies. Advanced technologies, such as artificial intelligence and machine learning, are also being integrated to analyze large datasets and identify patterns that can refine resuscitation strategies. Public awareness campaigns and bystander cardiopulmonary resuscitation (CPR) training initiatives further complement these efforts, as immediate intervention by nonmedical personnel significantly improves survival rates. By combining these approaches, healthcare systems aim to create a more efficient and effective response framework that maximizes patient outcomes and minimizes mortality related to SCA. Basic cardiopulmonary resuscitation (CPR-B) is unanimously consolidated as the optimal response to cardiopulmonary arrests. It is updated every 5 years with recommendations that have been tested and shown to be more efficient.10–14
Many studies suggest that people who do not receive CPR-B assistance during cardiac arrest have a lower chance of survival. 15 Cardiopulmonary arrest is a time-dependent pathology, meaning that the longer a patient goes without healthcare attention (CPR-B), the greater the injuries. The drinker curve shows that after 4 min without CPR-B, the chances of success decrease to 50%.16,17 Various studies state that it is crucial to recognize cardiac arrest early, perform early CPR-B, and defibrillate with a semi-automatic defibrillator (AED) as soon as possible to reduce morbidity and mortality in patients who suffer a cardiopulmonary arrest. 18
Despite strong scientific evidence supporting the importance of BLS-CPR training (Basic Life Support cardiopulmonary resuscitation) in resuscitation maneuvers among athletes remains insufficient. A study that followed the recommendations of the European Resuscitation Council (ERC) found that most professional athletes lack basic CPR knowledge and adopt a passive attitude toward cardiovascular emergencies on the field. 19
Existing gaps in CPR knowledge among professional athletes
Despite the critical nature of CPR in sports settings, significant knowledge and skill gaps exist among professional athletes. Research reveals that while cardiac events in sports can be potentially fatal, proper training and immediate response can dramatically improve survival rates. However, multiple studies indicate that professional athletes across various sports remain underprepared for these emergencies, creating dangerous gaps in the sports emergency response chain. 20
Knowledge and awareness deficiencies
Basic understanding of cardiac emergencies
A profound gap exists in professional athletes’ basic understanding of SCA and its implications. In a survey presented at the Care of the Athletic Heart conference, only 50% of collegiate athletes reported knowing what SCA actually is, demonstrating a fundamental knowledge deficit. This lack of understanding directly impacts how athletes perceive cardiac risks in sports settings. The same study revealed that a mere 7.7% of athletes expressed concern about SCA occurring during play, indicating a significant disconnect between the actual risk and athletes’ perception of it.
Recognition of emergency situations
Professional athletes often struggle to recognize the signs of cardiac emergencies, which delays critical intervention. Without proper training, many athletes may misinterpret serious cardiac events as less urgent conditions such as fatigue, dehydration, or minor injuries. Effective CPR requires prompt recognition of SCA, and this recognition gap represents a serious barrier to immediate action. The ability to quickly identify when a teammate or competitor is experiencing SCA rather than another form of collapse is essential but often lacking among professional athletes. 21
Therefore, BLS-CPR training for players and coaches is not only a crucial preventive measure but also a strategy that can save lives.
Research demonstrates alarmingly low rates of CPR certification among professional athletes. A survey of professional football players in Turkey revealed that only 7.7% had received formal CPR training with certification, and merely 5.9% had undergone this training within the previous 5 years. This indicates that even among those with some training, knowledge may be outdated or forgotten. The survey of collegiate athletes showed slightly better but still concerning results, with 51% reporting having received some form of CPR training. 22
Despite its vital importance, there is no conclusive evidence in the analyzed results confirming the existence of systematic training programs specifically aimed at elite athletes. 23
This study aims to describe CPR-B knowledge among football professionals. In addition, based on the hypothesis that attitude influences a better response to a cardiac arrest situation, a study was conducted to describe attitude and knowledge among different groups based on sociodemographic parameters to determine the effectiveness of an intervention regarding the cognitive-attitudinal increase in CPR-B.
The aim of the study is to evaluate the change in attitudes and knowledge about CPR-B in football professionals following a training intervention and to examine its correlation with sociodemographic variables.
Methods
Study design
This study followed a single-group, pre-post intra-subject design, aimed at evaluating changes in knowledge and attitude regarding CPR-B before and after an educational intervention. Although no external control or comparison group was included, each participant served as their own control by comparing their pre- and post-intervention responses. This design allows for the assessment of within-subject changes over time, minimizing the influence of individual differences and confounding variables.
The study was conducted in two phases:
Pre-intervention phase: An observational cross-sectional study was carried out with 206 professional football players and coaches. Participants completed a baseline questionnaire assessing CPR-B knowledge and attitudes. Immediately after completing the questionnaire, they participated in a standardized CPR-B training session.
Post-intervention phase: One month after the training, a follow-up online questionnaire was administered to assess changes in the same domains (knowledge and attitude). A total of 70 participants responded to this post-test. The reduced number of responses in the post-phase is attributed to the change in administration method: while the pre-test was conducted in-person with the surveyor present, the post-test was distributed online through the clubs, and participants were required to complete it independently.
This within-subject comparison design, where each participant’s post-intervention data is compared to their own baseline data, is what constitutes the “intra-subject control.” The approach is appropriate for assessing educational interventions where randomization or the inclusion of a separate control group may not be feasible due to ethical or logistical constraints.
Sample definition and data collection
The intervention was implemented with professional football players and coaches in the Valencian Community (Spain) in 2022. The participants’ data were pseudonymized.
The sample size was determined using G*Power software (Version 3.1.9.6). A power analysis was conducted for the comparison of paired means in the variables attitude and knowledge. The parameters used for the calculation were a significance level (α) of 0.05, a statistical power (1 − β) of 0.95, and an effect size of 0.5, which is commonly considered medium.
The analysis resulted in a required sample size of 54 participants. However, considering potential sample attrition between the pre- and post-measurements, a larger initial sample of 206 participants was selected. Ultimately, 70 participants completed the study.
Ethical aspects
The study was approved by the Biomedical Research Ethics Committee of CEU Cardenal Herrera University (CEEI22/286), with prior approval from the medical teams of the first-division football clubs in the Liga Santander in the Valencian Community (Spain). The study is also registered in Clinical Trials (NCT06812312).
All participants provided written informed consent to take part in the present study.
Study design and selection criteria
The sampling carried out was non-probabilistic and incidental. Inclusion criteria included being professional football players or coaches in the Valencian Community and voluntarily participating in the study. All participants gave their written consent after being informed. The following data were recorded for each participant: gender, education level, category (player or coach), and age. Exclusion criteria included having suffered from a serious health problem and not understanding English or Spanish.
Validated questionnaires were used to assess the attitude toward helping others in CPR-B for both lay first responders and healthcare professionals 24 and those by Chen et al. 25 and Oteir et al. 26 to assess CPR-B knowledge.
The first questionnaire, 24 consisted of three sections with a total of 19 questions, including individual information, current status and effects of CPR training, attitude toward CPR training, and willingness to providing help in an emergency situation, and the second one was a structured questionnaire consisting of 4 sections with 27 nominal-level binary questions.25,26
The resulting questionnaire consisted of 39 questions assessing both attitudes and knowledge. It was divided into 19 Likert-type items using a 5-point scale (1 = strongly disagree; 2 = disagree; 3 = neither agree nor disagree; 4 = agree; 5 = strongly agree) and 20 multiple-choice questions. A total score was calculated, and an improvement was expected after the intervention, with post-intervention scores surpassing the initial scores.
The internal consistency of both questionnaires was analyzed using Cronbach’s Alpha, obtaining a value of 0.84 for attitude and 0.58 for knowledge.
In addition, some questions about CPR knowledge, based on the CPR knowledge questionnaire by Pivač et al. 24 were added and validated by an expert committee to check their relevance. The resulting questionnaire, comprising 39 items, was analyzed before and after the intervention, and statistical analysis was conducted on the sociodemographic variables (gender, education level, and role of participants).
To gather the various aspects mentioned, from the perception of the importance of training, the necessity or utility of knowing the CPR-B technique, and the change in knowledge and attitude of participants after training, the questionnaires were structured and administered following the procedure described in Figure 1.

Flowchart of the different phases of the study.
This way, a preliminary version of a data collection tool that combines attitude assessment with knowledge assessment was obtained, as a correlation between both competence dimensions was verified.
The final questionnaire consists of 39 questions and was administered online in the second phase (FORMS/Office 365 platform). The total population registered in the Football Federation of the Valencian Community is 454, with a response rate of 45%. 27 The questionnaire responses are in the possession of the researchers and can be consulted upon request.
After completing the questionnaire, a 2-h training intervention was conducted by a CPR-B instructor. The first 30 min were dedicated to explaining how to recognize a cardiopulmonary arrest, the correct technique for chest compressions, ventilations, and AED use. The remaining 90 min were for the practical application of the intervention. This was conducted with five CPR-B training torsos (Little Anne QCPR training mannequin, Laerdal) and a simulated AED for CPR training (AED Practi-Trainer – Bilingual, WNL). Both theoretical and practical training were provided by a basic life support instructor from the Spanish Society of Intensive Care Medicine and Coronary Units, instructing participants under the 2021 ERC recommendations. 12 One month after the training intervention, the questionnaire was administered again via the FORMS platform of Office 365 (CEU Cardenal Herrera University) to measure changes in knowledge and attitudes post-training. One month is a time period that balances the need to observe significant and sustained changes with the practicality and efficiency of the study. It is a common choice that allows for effective evaluation of medium-term results. Studies such as those by Hamdan et al. 28 or Chang et al. 29 highlight the importance of evaluating the impact of CPR educational interventions in the short term, such as at 30 days, to measure knowledge retention and changes in attitudes. Out of the 206 professionals who participated in the initial training, a total of 70 individuals responded to the post-intervention questionnaire (post-educational intervention response rate = 34%). With this sample size, a power greater than 0.99 is obtained, considering a significance level of 0.05 and an effect size of 0.5, calculated for a difference of 0.2 and a standard deviation of 0.5. The analysis of correct responses was conducted using the unified questionnaire, and the results were compared with those obtained in the first phase. The database is available in a repository and will be provided upon reasoned request.
Data analysis
In the first phase of the study, a cross-sectional analysis was performed using pre-intervention data from 206 participants. Baseline attitude and knowledge, expressed as mean ± standard deviation (SD), were analyzed in relation to sociodemographic variables. Normality was assessed using the Shapiro–Wilk test. Both attitude (W = 0.9722, p = 0.0004) and knowledge (W = 0.9651, p < 0.0001) were found to be non-normally distributed, so nonparametric tests were employed. Specifically, the Wilcoxon rank-sum test was used to compare groups based on sex and role in the team, the Kruskal–Wallis test was used for level of education, and Spearman’s rank correlation coefficient was calculated to assess correlations with age and between attitude and knowledge.
In the second phase, a pre-post intervention analysis was conducted. The variables of interest were the change in attitude and the change in knowledge, both calculated as the difference between pre- and post-intervention scores and expressed as mean ± SD. These changes were analyzed to assess two types of variation: intra-group variation, which refers to whether the change in attitude or knowledge within the same group (e.g., men, women, players, or coaches) was significant; and between-group variation, which examines whether these changes differed significantly between groups (e.g., whether the increase in attitude was greater in men than in women). The Shapiro–Wilk test was again used to assess normality. The change in attitude was normally distributed (W = 0.9754, p = 0.1826), whereas the change in knowledge was not (W = 0.9554, p = 0.0141). Therefore, a one-sample t-test was used to determine if the increase in attitude was significant for the entire group and each subgroup. Independent samples t-tests were used to compare increases in attitude with respect to sex and role in the team. ANOVA was used to compare attitude changes across different levels of education, and Pearson’s correlation coefficient was used to determine the correlation between age and attitude change. Analogously, for the nonparametric analysis of knowledge change, the Wilcoxon signed-rank test was used to assess overall significance, the Wilcoxon rank-sum test was used for comparisons involving sex and professional role, the Kruskal–Wallis test was used for education level, and Spearman’s rank correlation was used for age and between attitude and knowledge.
Variables with a normal distribution are expressed as mean ± SD, while non-normally distributed variables are expressed as median and interquartile range.
Results
The results obtained in the first phase of the study, both in terms of knowledge and attitude, do not follow a normal distribution, so they were statistically analyzed using nonparametric methods. For correlations, a linear regression model was used, and it was checked whether the Pearson coefficient was significantly different from zero. It was checked whether the participants’ attitudes and knowledge were related to their age using regression analysis. Table 1 shows the pre-post intervention participant profile.
Relationship between professional category, gender, and educational level of the participants, pre-post intervention. Valencia Community, Spain, 2022.

ESO: compulsory secondary education; VET: vocational education and training.
N = 206: sample pre-intervention.
N = 70: sample post-intervention.
In the cross-sectional phase, 206 individuals participated (response rate = 63%), including professional coaches and players, with an average age of 25.01 ± 8.4, ranging from 17 to 38 years old. The average age of coaches was 35.2 ± 8.0, and that of players was 21.9 ± 3.6.
Figure 1 shows the flow diagram of the intervention’s evolution over time.
Table 2 shows the attitude and knowledge results of the participants before the intervention. It was observed that attitude was independent of the participant’s age (rho = 0.0743, p = 0.2883), while knowledge showed a significant correlation with age (rho = 0.3907, p < 0.0001). The positive Pearson coefficient indicates an increase in knowledge with age (Table 3).
Relationship between the attitude and knowledge of the participants before the educational intervention and comparison between groups. Valencia Community, Spain, 2022.
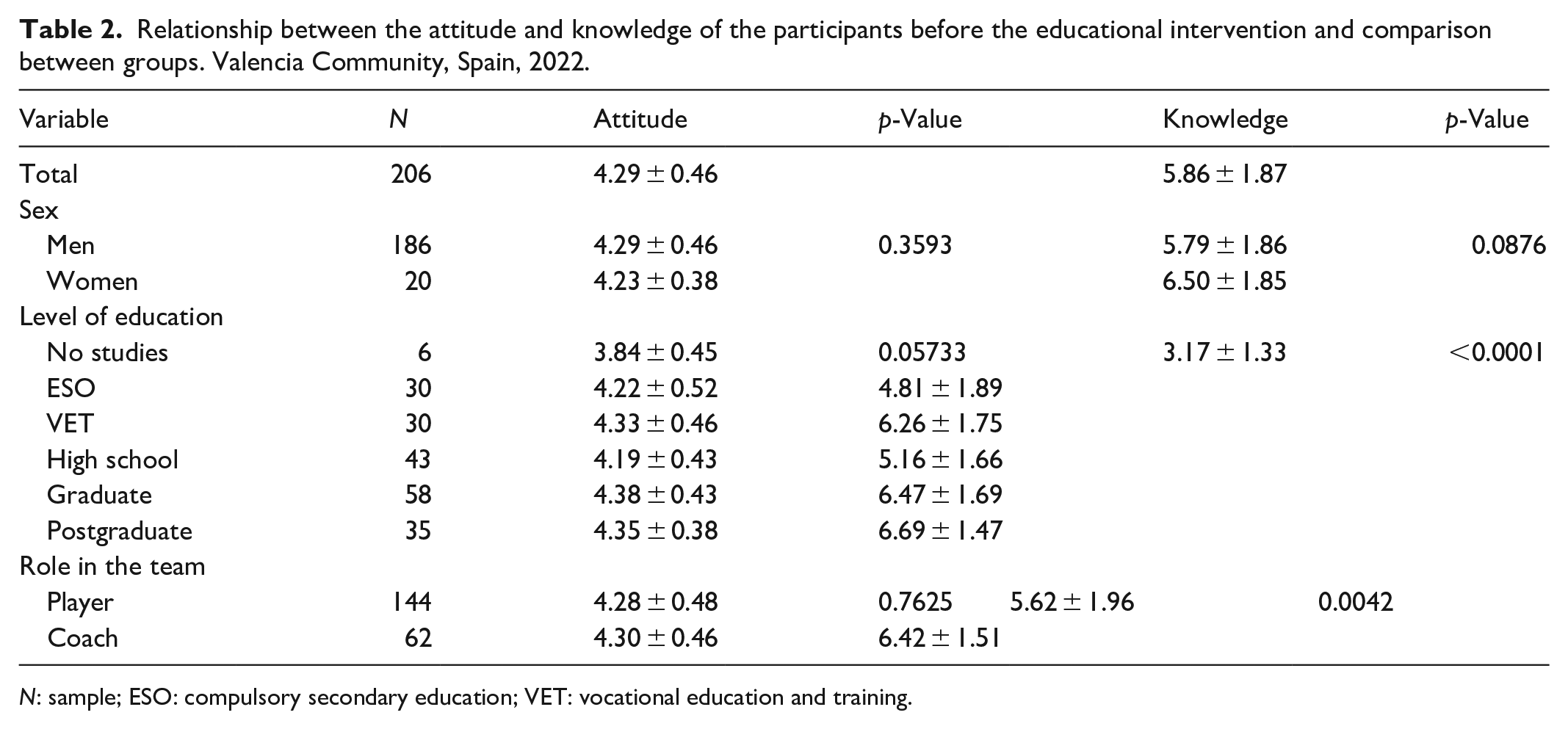
N: sample; ESO: compulsory secondary education; VET: vocational education and training.
Correlation analysis between the main variables and age.

Pearson test.
Spearman test.
Furthermore, a possible correlation between attitude and knowledge was studied, yielding significant results (rho = 0.1500, p = 0.0314).
Regarding the correlation between knowledge and education level, it was observed that the higher the academic degree, the greater the CPR knowledge (p < 0.0001).
In knowledge, although women have a higher average score (6.50 vs 5.79), the p-value of 0.0876 suggests that the difference is not statistically significant but indicates a trend where women may have better CPR knowledge than men.
In attitude, there is a trend toward significance (p = 0.0573), suggesting that individuals with less education may have a less favorable attitude toward CPR. In knowledge, differences are statistically highly significant (p < 0.0001). Participants without education have the lowest knowledge, while university graduates and postgraduates have the highest scores.
This suggests that formal education plays a crucial role in CPR knowledge, likely due to exposure to medical and scientific training.
In the second phase of the study, 70 responses were obtained for the post-intervention questionnaire.
It was verified that there was a significant increase (p = 0.0004) in participants’ attitudes before the intervention (4.25 ± 0.39) and after (4.40 ± 0.41). Knowledge also shows a significant increase (p < 0.0001) between before (5.66 ± 1.92) and after (7.60 ± 1.84) the intervention.
No significant relationship was found when analyzing a possible correlation between age and variations in attitude (p = 0.6782) and variations in knowledge (p = 0.6115). Table 3 shows a significant increase in attitude and knowledge post-intervention within the categories of gender, education level, and team role, with the intervention being equally effective for all categories (Table 4).
Variation in the attitude and knowledge of the participants after the intervention. Valencia Community, Spain, 2022.

N: sample; ESO: compulsory secondary education; VET: vocational education and training.
t-Student test for a mean.
Wilcoxon test for a mean.
t-Student test for two means.
Wilcoxon test for two means.
ANOVA test.
Kruskal–Wallis test.
Discussion
This study evaluates the knowledge and attitude toward CPR maneuvers in football professionals, demonstrating that the practical intervention following theoretical training significantly improves CPR knowledge levels. The effectiveness of practical training in CPR has been widely documented in the literature, emphasizing its role in skill retention and confidence building. 16 Studies show that hands-on training leads to better long-term recall and performance compared to theoretical instruction alone.
When comparing both genders in the knowledge questionnaire, although no statistical significance was found, indications were observed as the Women group showed a higher knowledge level compared to the Men group, consistent with other studies concluding that the Women group is better prepared in this area than the Men group. 30 Conversely, in other similar studies, the Men group showed better scores in compression and ventilation practice. 31 This discrepancy may be due to differences in physical strength or confidence levels during hands-on CPR execution. Despite the continuous growth of women’s football, the number of teams is still lower than that of men’s football. Future studies may reinforce or refute our findings with more solid statistical significance.
Furthermore, coaches demonstrated greater CPR knowledge than players, likely influenced by education level and age, as both variables correlate with improved knowledge acquisition. In our study, 61.3% of the coaches had a university degree, and their average age was 1.6 times higher than that of players. Older individuals typically accumulate more life experience and training opportunities, which can positively impact their CPR competence. In addition, the players’ group included individuals with no formal education (4%), which may contribute to lower overall knowledge scores. This aligns with research highlighting education as a key determinant of CPR proficiency, where individuals with higher academic training display better retention and execution of CPR techniques. 32
The study also found that participants with a higher attitude toward CPR achieved better knowledge scores. This suggests that motivation and willingness to learn play crucial roles in effective CPR education. 33 A positive attitude has been linked to increased engagement during training sessions, leading to higher skill retention. However, age did not influence attitude, indicating that motivation for learning CPR may be independent of life stage, reinforcing the importance of universal training initiatives across all age groups.
This study confirms that the practical intervention was effective, as it improved both attitude and knowledge levels in participants. Importantly, these benefits were universal, occurring independently of gender, role (player or coach), education level, or age, as in the study carried out in the West Bank by Amro and his team. 34 Previous studies support the idea that well-structured CPR training programs can produce significant learning gains across diverse populations, regardless of demographic differences. 35 Given these findings, football professionals should be systematically trained in CPR to ensure readiness for on-field emergencies, potentially reducing SCA fatalities in sports. 36
The standard certification renewal period for CPR skills is currently set at every 2 years according to guidelines established by major resuscitation authorities. This biennial recertification standard has been widely adopted across various sectors, including healthcare, education, and athletics.
However, emerging evidence suggests that this 2-year interval may be insufficient for maintaining effective CPR skills. Research indicates significant skill degradation occurs much sooner than the standard recertification timeline, potentially compromising the effectiveness of emergency response when it matters most. This finding has serious implications for professional athletes who may need to respond to cardiac emergencies among teammates, coaching staff, or even spectators. 37
This research reinforces the importance of CPR education in sports environments. Future studies should aim to expand sample sizes to confirm trends in gender-based knowledge differences; evaluate long-term knowledge retention to determine whether periodic refresher courses are necessary; investigate the impact of real-life CPR experiences on confidence and performance and assess the influence of CPR simulations under stress conditions, as real-life cardiac arrest scenarios often involve high-pressure decision-making. 38
By integrating CPR training into standard sports curricula, football professionals can enhance their preparedness, potentially saving lives in critical moments. Considering that the number of participants ensures the power of the intervention and that the studied group of elite football players have a similar profile of habits oriented toward high performance, as well as the fact that the intervention is based on the ERC standards, the intervention could be extrapolated to any country that uses these recommendation guidelines.
Study limitations
The response rate after the intervention may have been affected because the pre-intervention questionnaire was conducted alongside the CPR-B instructor, and after the intervention, the questionnaire was sent online 1 month later, with participants responding alone. This suggests that follow-up methods need to be robust to ensure continuous participation, although, in our study, the study power remains higher than the threshold we had set.
Additionally, there was difficulty accessing first-division team players due to their sporting commitments, as well as possible self-reporting biases that could arise from using an online-administered questionnaire and conducting non-probabilistic sampling.
Conclusions
After the presented analyses, it is observed that, thanks to the intervention, there is an increase in attitude and knowledge. However, this increase does not depend on gender, category (Player, Coach), education level, or age, demonstrating that the intervention works for all participants, regardless of the initial situation, as shown in Table 3.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251341107 – Supplemental material for Effect of basic cardiopulmonary resuscitation training on the knowledge and attitudes of professional football players and coaches
Supplemental material, sj-docx-1-smo-10.1177_20503121251341107 for Effect of basic cardiopulmonary resuscitation training on the knowledge and attitudes of professional football players and coaches by Rafael González-Moret, Isabel Almodóvar-Fernández, Sara Simón-Montolio, Héctor Usó-Vicent, Paula Sánchez Thevenet and Antonio Real-Fernández in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge Villarreal Football Club, Elche Club De Fútbol, Levante Unión Deportiva, and all participants for their contribution to the study. To all the players and coaches who made this study possible.
ORCID iDs
Ethical considerations
Ethical approval for this study was obtained from Biomedical Research Ethics Committee of CEU Cardenal Herrera University (CEEI22/286).
Consent to participate
Written informed consent was obtained from all subjects before the study.
Author contributions
Rafael González-Moret: Conceptualization; Data Acquisition; Formal Analysis; Investigation; Methodology; Writing Original Draft; Writing Review and editing; Agrees to be held accountable for all aspects of work, ensuring integrity and accuracy. Isabel Almodóvar-Fernández: Conceptualization; Data Acquisition; Formal Analysis; Investigation; Methodology; Writing Original Draft; Writing Review and editing; Agrees to be held accountable for all aspects of work, ensuring integrity and accuracy. Sara Simón-Montolio: Conceptualization; Data Acquisition; Investigation; Methodology; Writing Original Draft; Writing Review and editing; Agrees to be held accountable for all aspects of work, ensuring integrity and accuracy. Héctor Usó-Vicent: Conceptualization; Data Acquisition; Investigation; Methodology; Writing Original Draft; Writing Review and editing; Agrees to be held accountable for all aspects of work, ensuring integrity and accuracy. Paula Sánchez Thevenet: Conceptualization; Data Acquisition; Formal Analysis; Investigation; Methodology; Writing Original Draft; Writing Review and editing; Agrees to be held accountable for all aspects of work, ensuring integrity and accuracy. Antonio Real-Fernández: Conceptualization; Formal Analysis; Investigation; Methodology; Writing Original Draft; Writing Review and editing; Agrees to be held accountable for all aspects of work, ensuring integrity and accuracy.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IA-F and HU-V were employed by Villarreal Football Club. The remaining authors declare no conflict of interest.
Trial registration
Impact of Basic Cardiopulmonary Resuscitation on the Knowledge and Attitude of Professional Football Players and Coaches (VILRCP): NCT06812312.
Repositorio
10.5281/zenodo.14674449.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.