
Abstract
Objective:
This pilot study aims to assess how individuals with rhythm perception, particularly musicians, are able to maintain the predefined chest compression rate during cardiopulmonary resuscitation compared to people without rhythm perception.
Methods:
The study was conducted at the Pilsen Emergency Medicine Conference (Czechia) using a simulation-based cohort design. Participants performed chest compressions on a manikin for 120 s, with the first 10 s guided by a metronome. Participants were grouped based on self-reported rhythmic perception, such as playing a musical instrument. The primary outcome was the average chest compression rate per minute.
Results:
A total of 67 participants were included. Both groups provided chest compression rate within the recommended limits. Musicians maintained a better chest compression rate (mean 110.56 compressions per minute) compared to nonmusicians (mean 107.31; T-test, p = 0.00074). Those with any rhythmic perception experience also performed better (T-test, p = 0.036931). Secondary factors, including gender, clinical experience, and prior resuscitation training, did not significantly affect the results.
Conclusion:
This study demonstrates that individuals with rhythm perception, especially musicians, follow the predefined frequency of chest compressions more effectively.
Introduction
Maintaining the correct chest compression rate together with depth, chest recoil, and hand position during cardiopulmonary resuscitation (CPR) is crucial for successful resuscitation and improving the chances of return of spontaneous circulation. The European Resuscitation Council Guidelines 2021 recommend a rate of 100–120 compressions per minute.1,2 Various melodies, rhythms, and songs have been suggested to help rescuers maintain the correct compression rate.3 –6 The use of feedback devices during training and providing CPR was recommended by International Liaison Committee on Resuscitation (ILCOR) already in 2020 with some limitations: the authors suggested the use of feedback devices that provide directive feedback on compression rate, depth, chest recoil, and hand position while when feedback devices are not available, they suggested the use of at least tonal guidance (music or metronome). 7 Recent ILCOR Consensus on Science with Treatment Recommendations generalise its use and strongly recommends the use of CPR feedback devices during resuscitation training for healthcare and lay providers (with moderate certainty of evidence). 8
Rhythm refers to the system of organizing sounds over time, characterized by repetition and regularity. 9 It is a fundamental aspect of musical composition, providing the structure that determines the tempo and flow of the melody.9,10 Musicians rely on the ability to feel and interpret rhythm, making rhythm education essential at all levels of musical training. 9 Rhythm also plays a role in psychology and education, as the ability to recognize and reproduce rhythms is important for cognitive development.11–13 Research shows that synchronization with rhythm can positively affect learning abilities and social interactions. 10 However, not everyone has a natural sense of rhythm, raising the question of whether playing music to guide the correct compression rate will work universally.
The aim of this study is to assess the ability of individuals with rhythmic perception to maintain the predefined chest compression rate during CPR.
Material and methods
Study design
This is a pilot prospective simulation-based cohort study designed to explore the relationship between rhythmic perception and the ability to maintain the correct and predefined chest compression rate during resuscitation.
Setting
The study took place at the Pilsen Emergency Medicine Conference (Czech Republic) held from February 29 to March 1, 2024. All medical professionals attending the conference were asked to join the study and their participation was fully voluntary.
The resuscitation was performed using a Resusci Anne QCPR manikin (Laerdal Medical, Norway), provided by SNT Plus s.r.o. company. Data collection was facilitated by a SimPad Plus with Skill Reporter software version 8.7 (Laerdal Medical, Norway).
The manikin was placed on the floor in the hotel lobby where the conference was held, on a resuscitation mat to ensure comfort for the rescuers. A metronome on a mobile phone was used to provide an initial rhythm.
In the first 10 s of simulated chest compressions, a loud metronome at a rate of 110 compressions per minute was used to set the pace. The remaining 110 s were conducted without the metronome, requiring participants to maintain the correct rate on their own. The software connected to the manikin recorded both the compressions and the success rate of chest compressions and recoil. Each recording was divided into 10-s intervals, during which the average compression rate was calculated.
Participants
As this was a pilot study, it was not possible to conduct a valid power analysis to predetermine the number of participants. The selection was random, including representatives from various professions within emergency medicine and nursing who attended the medical conference. After completing the questionnaire and providing informed consent, participants performed a 2-min chest compression sequence. Inclusion criteria: medical professional at any level and completed questionnaire and informed consent. Exclusion criteria: not medical professional, health condition that might limit the quality of CPR (e.g., acute illness, disability) and not willing to complete the questionnaire and/or informed consent.
A standardized questionnaire was developed to assess participants’ experience with rhythmic perception, such as playing a musical instrument or dancing (the level of experience was self-reported on a scale from 1 to 10; where 1 is a beginner and 10 is a professional musician). The English version of the questionnaire is part of the Supplemental materials. The questionnaire was piloted on the student paramedics (10 students that represents 15% of the population tested) and amended for better clarity based on their comments. Based on the responses, participants were divided into cohorts for post hoc data analysis. The study was blinded; participants were unaware of the study’s objectives, and the researchers did not know the cohort assignments. A subset of experienced musicians, defined as those who rated their experience playing a musical instrument as 5 or higher, was selected for more accurate hypothesis testing. All participants were informed of their right to withdraw consent at any time.
Variables
The primary objective of the study is to determine whether individuals with rhythm perception are able to maintain the predefined chest compression rate compared to those without or fewer rhythm perception. The main rhythm perception was defined as playing a musical instrument.
The main outcome measure is the number of compressions in each 10-s interval during the 110-s total resuscitation time, from which the average chest compression rate per minute will be calculated. The rational for separation the time into 10-s cycles is to observe performance in time and to manually calculate every compression provided.
The secondary objective is to examine other factors that may influence rhythmic perception, such as experience with dancing. The relationship between years of professional experience and prior CPR training will also be evaluated.
Statistical analysis
To analyse the data, Kolmogorov–Smirnov Test of Normality was first applied, followed by calculations for means and variances based on the results. Cohort homogeneity (in the area of age, experience and last CPR training) was assessed using the Chi-square test or T-test, depending on the nature of the data. Differences between cohorts were evaluated using a T-test for two independent means. A significance level of p < 0.05 was set for the tests.
Results
Population
A total of 67 participants were included in the study. A detailed description of the population is provided in Table 1. The cohorts did not show significant differences in terms of gender, age, years of professional experience, or time since the last CPR training.
Population characteristics.
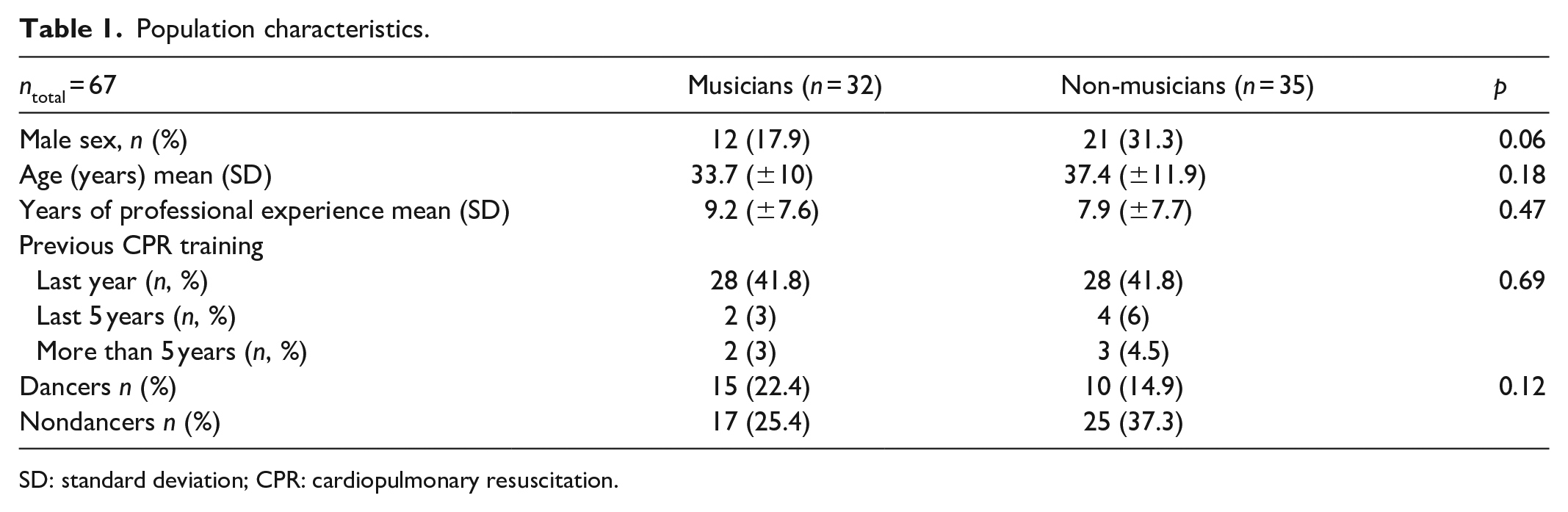
SD: standard deviation; CPR: cardiopulmonary resuscitation.
Primary outcomes
The variance in the average compression rate during the 10-s intervals was 2.09 among musicians, while it was 3.31 among nonmusicians. The overall mean compression rate was 110.56 compressions per minute for musicians and 107.31 for nonmusicians. Musicians were significantly closer to a predefined specific compression rate than nonmusicians (T-test; p = 0.00074). Experienced musicians (self-reported skill as 5 or more) also demonstrated better compliance with predefined compression rate compared to nonmusicians (T-test; p = 0.001714).
Both groups provided average chest compressions rate within the limits (100–120 per min) recommended by the guidelines during whole 2 min.
When comparing participants with any rhythmic perception experience (musicians and dancers) to those with no rhythmic perception experience, the compliance of mean compression rate with the predefined 110 per min was significantly better in the group with rhythm perception (T-test; p = 0.036931).
Secondary outcomes
All secondary outcomes did not reach statistical significance. There was no proven effect of gender (T-test; p = 0.897182), length of clinical experience (T-test; p = 0.293882), time since the last CPR training (T-test; p = 0.412842), experience with dancing (T-test; p = 0.660641), or even among experienced dancers (T-test; p = 0.475419).
Discussion
This pilot simulation study demonstrates that individuals with rhythmic perception experience, particularly those with musical instrument training, are better able to maintain predefined chest compression rate during CPR. The simulation was conducted without a predetermined sample size, reflecting the exploratory and pilot nature of the study.
Dalla Bella et al., 14 emphasize that music provides an excellent model for studying the relationship between perception and action, as listening to music often prompts physical movement, such as dancing. Brain regions typically associated with motor control, including the basal ganglia and cortical motor areas, are activated when listening to rhythmic sequences, even without actual movement. Their research suggests that hearing rhythmic patterns triggers motor areas of the brain, creating an urge to move in sync with the rhythm. The study also highlights that the ability to perceive and synchronize to rhythm is a universal skill that can be enhanced through musical training. 14 Musicians consistently perform better than nonmusicians in rhythm perception and synchronization tasks. On the other hand, some individuals, even without neurological conditions, may struggle significantly with rhythm perception or synchronization, and this difficulty may be exacerbated by neurodegenerative disorders.14 –16
Musicians tend to outperform nonmusicians in tasks involving rhythm perception and synchronization. 15 Musical training improves one’s ability to extract rhythmic patterns, analyse their structure, and reproduce them. 15 Additionally, musicians demonstrate more precise motor synchronization to rhythm compared to nonmusicians, as seen in tasks like tapping to rhythmic sequences such as a metronome or music. 15
The findings of this simulation study could have practical implications for CPR training. While playing a metronome or music to maintain the correct chest compression rate may benefit some, it may not be the ideal teaching tool for everyone. Individuals who lack a natural sense of rhythm may require alternative techniques to help them maintain the correct compression rate during resuscitation. Teaching groups with cognitive or neurodegenerative deficits should also rely on alternative instructional methods, rather than using music as a guide. These individuals may benefit more from techniques that focus on visual or tactile cues, structured practice with real-time feedback, or technology-assisted tools that help maintain the correct compression rate during CPR. Tailoring the approach to their unique needs is crucial for optimizing their learning and performance in resuscitation training. On the other hand, in practice medical dispatch centres may have the option to use metronome when providing telephone assisted CPR and results of this study showed that people were able to follow the correct rate for the rest of 2 min interval. The use of metronome in telephone-assisted CPR may be of benefit.
Limitations
This is a simulation study with a priori designed protocol. Nevertheless, certain limitations must be acknowledged. The simulation was conducted without a predetermined sample size, reflecting the exploratory and pilot nature of the study. The voluntary recruitment process introduces the potential for selection bias. Additionally, the utilization of a simulated environment with manikins may not entirely replicate real-life scenarios. It is imperative to bear these limitations in mind while interpreting the study results, emphasizing the necessity for further research to validate our findings in a more representative setting.
Conclusion
This pilot study demonstrates that individuals with rhythm perception experience, particularly musicians, maintain the predefined chest compression rate during CPR more effectively. While rhythm-based tools like metronomes or music can aid some learners, they may not be suitable for everyone. Further research is essential to develop personalized training approaches that meet the diverse needs of healthcare providers and lay rescuers.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241312968 – Supplemental material for The impact of rhythm perception on chest compression rate during CPR: Insights from a pilot simulation study
Supplemental material, sj-docx-1-smo-10.1177_20503121241312968 for The impact of rhythm perception on chest compression rate during CPR: Insights from a pilot simulation study by David Peran, Pavel Bohm, Matej Petru and Jana Kubalova in SAGE Open Medicine
Footnotes
Acknowledgements
We extend our sincere appreciation to SNT Plus s.r.o. company for their technical support in the simulation research, particularly for providing the high-fidelity mannequin. ChatGPT 4.0 was used for language corrections of finished manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Authors’ contributions (CRediT author statement)
DP: Conceptualization, Methodology, Formal Analysis, Writing – original draft; PB: Resources, Writing – Reviewing and Editing; MP: Data, Writing – original draft; JK: Conceptualization, Writing – Reviewing and Editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Student Grant Competition CTU SGS24/071/OHK5/1T/17.
Ethics approval and consent to participate
Ethical approval for this study was waived by the Ethics Committee of the Emergency Medical Services of the Karlovy Vary Region, under Number 3136/24/ZZSKVK with the rational that it is a simulation study without any intervention provided on humans. All participants provided written consent to participate in the simulation study and have the option to cancel the consent at any time.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.