
Abstract
Objective:
The prognostic factors of patients diagnosed with marginal zone B-cell lymphoma at the National Institute of Hematology and Blood Transfusion between January 2014 and January 2024 were analyzed.
Subjects and methods:
This cross-sectional descriptive study included 86 newly diagnosed and treated marginal zone B-cell lymphoma patients. Myelogram, histopathology, and immunohistochemical staining were performed for all patients. Diagnosis and classification were conducted according to the WHO 2008 criteria, while disease staging was determined using the Ann Arbor staging system.
Results:
All three subtypes of marginal zone B-cell lymphoma were identified: mucosa-associated lymphoid tissue lymphoma (73.3%), nodal marginal zone lymphoma (20.9%), and splenic marginal zone lymphoma (5.8%). The most frequently affected extranodal sites were the stomach (25.6%) and eyes (24.4%). The likelihood of stages III–IV disease was found to be 14 times higher in patients with B symptoms, 17 times higher in those with elevated lactate dehydrogenase, 34 times higher in those with increased B2-M levels, and 5.7 times higher in those with a Ki67 index > 30%. Bone marrow invasion was observed to be 14.8 times more likely in patients with elevated lactate dehydrogenase, 40 times more likely in those with increased B2-M levels, and 4.4 times more likely in those with a Ki67 index > 30%. A significant correlation was identified among hemoglobin concentration, lactate dehydrogenase, B2-M, and Ki67, indicating their potential as prognostic markers.
Conclusion:
Lactate dehydrogenase, B2-M, and Ki67 were found to be significantly associated with the prognosis of patients with marginal zone B-cell lymphoma.
Introduction
Marginal zone lymphoma (MZL) is a rare malignancy classified as a low-grade non-Hodgkin lymphoma (NHL). In the United States, MZL accounts for approximately 7% of all adult NHL cases, with an estimated 7460 new cases diagnosed in 2016. The average incidence rate is 19.6 per million individuals, with a slightly higher prevalence in males (20.5 per million) compared to females (19.1 per million). 1 MZL is categorized into three subtypes: extranodal MZL (EMZL), nodal MZL (NMZL), and splenic MZL (SMZL). EMZL, also referred to as mucosa-associated lymphoid tissue (MALT) lymphoma, is the most prevalent subtype, accounting for approximately 70% of cases. This subtype was first described in 1983. In contrast, NMZL and SMZL are less common, representing approximately 20% and 10% of cases, respectively.2,3
Several risk factors contribute to the development of MZL, including a family history of lymphoma, genetic predisposition linked to human leukocyte antigen variants, and autoimmune diseases. Infectious agents are also implicated in MZL pathogenesis, with Helicobacter pylori associated with gastric MZL, Chlamydia psittaci with ocular adnexal MZL, and Borrelia burgdorferi with cutaneous MZL. Additionally, hepatitis C virus infection, HIV infection, and a history of organ transplantation are recognized risk factors. 1
The clinical presentation of MZL is highly variable, depending on the affected organ. Due to its diverse manifestations, MZL is frequently misdiagnosed as other malignancies originating in the same anatomical region. 4 Survival outcomes for MZL patients vary by geographic region. The reported 5-year survival rates are 84.4% in the United States, 77.2% in the United Kingdom, 80% in the Netherlands, and 86.7% in Singapore. 1 These statistics suggest that MZL generally exhibits a favorable response to treatment, with prolonged survival and good quality of life.
However, prognostic outcomes differ among MZL subtypes. EMZL is associated with a more favorable prognosis compared to NMZL and SMZL. Additionally, tumor location significantly influences prognosis; gastrointestinal and pulmonary MZL subtypes are associated with poorer outcomes compared to those originating in the eye, skin, or thyroid. 4 Given the prognostic variability of MZL, accurate identification of tumor location, symptom onset, disease subtype, disease stage, and relevant prognostic markers is essential for optimal diagnosis, treatment planning, and patient management. This study aims to describe the clinical characteristics of MZL and investigate key prognostic factors influencing patient outcomes.
Methods
Study population
This study included 86 patients who were newly diagnosed with marginal zone B-cell NHL at the National Institute of Hematology and Blood Transfusion between January 2014 and January 2024. These patients were selected based on specific inclusion and exclusion criteria to ensure a consistent and reliable dataset for analysis.
Patients were eligible for inclusion if they were diagnosed with marginal zone B-cell NHL according to the World Health Organization (WHO) 2008 classification. 5 Additionally, only patients aged 16 years or older were considered. To maintain the integrity of the study, complete medical records were required to ensure sufficient clinical data for evaluation. Moreover, all participants were required to provide informed consent before being enrolled in the study.
Patients were excluded from the study if they had previously received treatment for marginal zone B-cell NHL at another medical facility before being admitted to the National Institute of Hematology and Blood Transfusion. Patients who lacked essential laboratory test results, including peripheral blood cell counts, bone marrow cytology, histopathology, blood chemistry, or imaging data, were also excluded, as these tests were necessary for assessing synchronous damage. Additionally, patients diagnosed with other concurrent malignant diseases were not included in the study. Finally, those with incomplete medical records were also excluded to ensure the reliability of the data.
Research design
This study was conducted using a retrospective cross-sectional descriptive design covering a 10-year period from January 1, 2014 to January 31, 2024. The diagnosis of marginal zone B-cell NHL was made according to the WHO 2008 classification. 5 To determine the disease stage, the Ann Arbor staging system was applied, which is a widely accepted method for staging lymphoma. 6
Criteria for evaluating laboratory parameters
Several laboratory indicators were assessed to evaluate disease severity and prognosis. Hemoglobin levels were categorized as normal (⩾12.0 g/dL), mild anemia (<12.0 and ⩾9.0 g/dL), moderate anemia (<9.0 and ⩾6.0 g/dL), and severe anemia (<6.0 g/dL). Platelet counts were classified as normal (⩾150,000 cells/µL) or low (<150,000 cells/µL).
White blood cell (WBC) counts were divided into three categories: high (>10,000 cells/µL), normal (4000–10,000 cells/µL), and low (<4000 cells/µL). Similarly, neutrophil counts were classified as high (>5500 cells/µL), normal (2800–5500 cells/µL), and low (<2800 cells/µL). Lymphocyte counts were considered high (>3000 cells/µL), normal (1200–3000 cells/µL), or low (<1200 cells/µL).
The lactate dehydrogenase (LDH) index was used to assess metabolic activity, with values classified as increased (>460 U/L) or normal (⩽460 U/L). Additionally, beta-2 microglobulin (B2-M) levels were recorded, with increased levels defined as >2.2 mg/L and normal levels as ⩽2.2 mg/L. Prognostic factors were assessed using the International Prognostic Index (IPI), which is commonly used for predicting outcomes in lymphoma patients. 7
Statistical analysis
All research data were compiled into an EpiData file and processed using SPSS version 23.0, IBM Corp. Descriptive statistics were used to summarize the data, with frequencies and percentages presented in tabular format. For analytical statistics, the chi-square test and relative risk (RR) were applied to determine the significance of relationships between variables, using a 5% significance level and a 95% confidence interval (CI). The odds ratio (OR) was also calculated to assess associations between risk factors and outcomes. For cases where the expected frequency was less than five, the Fisher exact test was used (P Yates correction applied). Additionally, the T-test was used to compare mean values between different patient groups.
Ethical considerations
This study was conducted following ethical guidelines and was approved by the Ethics Council of Hanoi Medical University under decision No. 4900/QĐ-DHYHN. All patient data were handled confidentially, and informed consent was obtained from all participants.
Results
A total of 86 patients diagnosed with marginal zone B-cell NHL were included in the study, comprising 63 cases of EMZL, 18 cases of NMZL, and 5 cases of SMZL. Among the 63 EMZL cases, the most frequently affected sites were the stomach (22 cases), eyes (21 cases), intestines (6 cases), parotid gland (4 cases), lungs (4 cases), liver (2 cases), skin (2 cases), thyroid gland (1 case), and mammary gland (1 case). Extranodal manifestations were observed in 73.3% of cases, making them the most common presentation, followed by nodal involvement in 48.8% of cases. Splenomegaly was exclusively detected in the SMZL group (100%), while extra-lymphatic involvement was observed only in EMZL cases (100%). No patients in the NMZL group exhibited either of these characteristics. Lymph node involvement was primarily observed in the sternocleidomastoid nodes (32.6%) and abdominal nodes (30.2%). Inguinal lymph node lesions were rarely found in the EMZL and SMZL groups, while axillary lymph node lesions were uncommon in NMZL cases. The majority of patients were diagnosed at stages I and II (72.1%), with a significantly higher proportion in the EMZL group (88.9%) compared to the NMZL (33.4%) and SMZL (0%) groups. This difference was found to be statistically significant (p < 0.001) (Table 1).
Clinical characteristics of MZL patients.

MZL: marginal B-cell lymphoma; MALT: mucosa-associated lymphoid tissue; NMZL: nodal marginal zone lymphoma; SMZL: splenic marginal zone lymphoma.
The mean hemoglobin level was recorded at 12.7 ± 2.6 g/dL (range: 2.2–16.7 g/dL), with 27.9% of patients exhibiting decreased hemoglobin levels, primarily at a mild level (22.1%). Hemoglobin levels in the SMZL group were found to be significantly lower than those in the EMZL and NMZL groups (p < 0.05). The mean WBC count was 9800 ± 13,800 cells/µL (range: 2500–111,000 cells/µL), with 80.2% of patients having WBC counts within the normal range. Among the three subtypes, WBC counts in the SMZL group were significantly higher than those in the EMZL and NMZL groups (p < 0.05) (Table 2).
Characteristics of blood tests and bone marrow biopsy of MZL patients.

MZL: marginal B-cell lymphoma; MALT: mucosa-associated lymphoid tissue; NMZL: nodal marginal zone lymphoma; SMZL: splenic marginal zone lymphoma; Hb: hemoglobin; WBC: white blood cell; LDH: lactate dehydrogenase; B2-M: beta-2 microglobulin.
All 86 patients (100%) exhibited small tumor cells, confirming a uniform histopathological characteristic across all MZL subtypes. Lymphoepithelial lesions were present in 57% of cases, predominantly in the EMZL group (74.6%), while absent in NMZL and observed in 40% of SMZL cases. Large cell transformation was rare, detected in only 1.2% of cases (one EMZL patient). Dutcher bodies were found in 20.9% of cases, exclusively in the EMZL group. An increased number of plasma cells was noted in 38.4% of cases, most commonly in EMZL (41.3%) and NMZL (38.9%), but absent in SMZL. The Ki67 proliferation index >30% was observed in 15.1% of cases, with the highest prevalence in SMZL (40%), followed by NMZL (22.2%) and EMZL (11.1%) (Table 3).
Histopathological findings of the patient group.

MZL: marginal B-cell lymphoma; MALT: mucosa-associated lymphoid tissue; NMZL: nodal marginal zone lymphoma; SMZL: splenic marginal zone lymphoma.
The majority of patients were classified as low-risk, with a prevalence of 44.2%. The low-risk rate in the EMZL group was recorded at 50.8%, which was significantly higher than that in the SMZL group (0%), with a statistically significant difference (p < 0.05). No significant differences were observed in risk subgroups between EMZL and NMZL or NMZL and SMZL (Table 4).
Classification of risk groups according to the international prognostic score (IPI).

MZL: marginal B-cell lymphoma; MALT: mucosa-associated lymphoid tissue; NMZL: nodal marginal zone lymphoma; SMZL: splenic marginal zone lymphoma; IPI: international prognostic index.
Patients with stages III and IV disease were more frequently observed in those aged ⩾ 60 years, those presenting with B symptoms, and those with reduced hemoglobin levels (<120 g/L) or decreased platelet counts (<150 G/L). An abnormal WBC count (>10 or <4 G/L) and an increased lymphocyte count (>3 G/L) were also associated with a higher likelihood of advanced-stage disease. Additionally, bone marrow biopsy findings indicating marrow invasion, elevated LDH levels (>460 U/L), increased B2-M levels (>2.2 U/L), and a Ki67 index exceeding 30% were all significantly associated with stages III and IV disease (Table 5).
Some factors related to the disease stage.
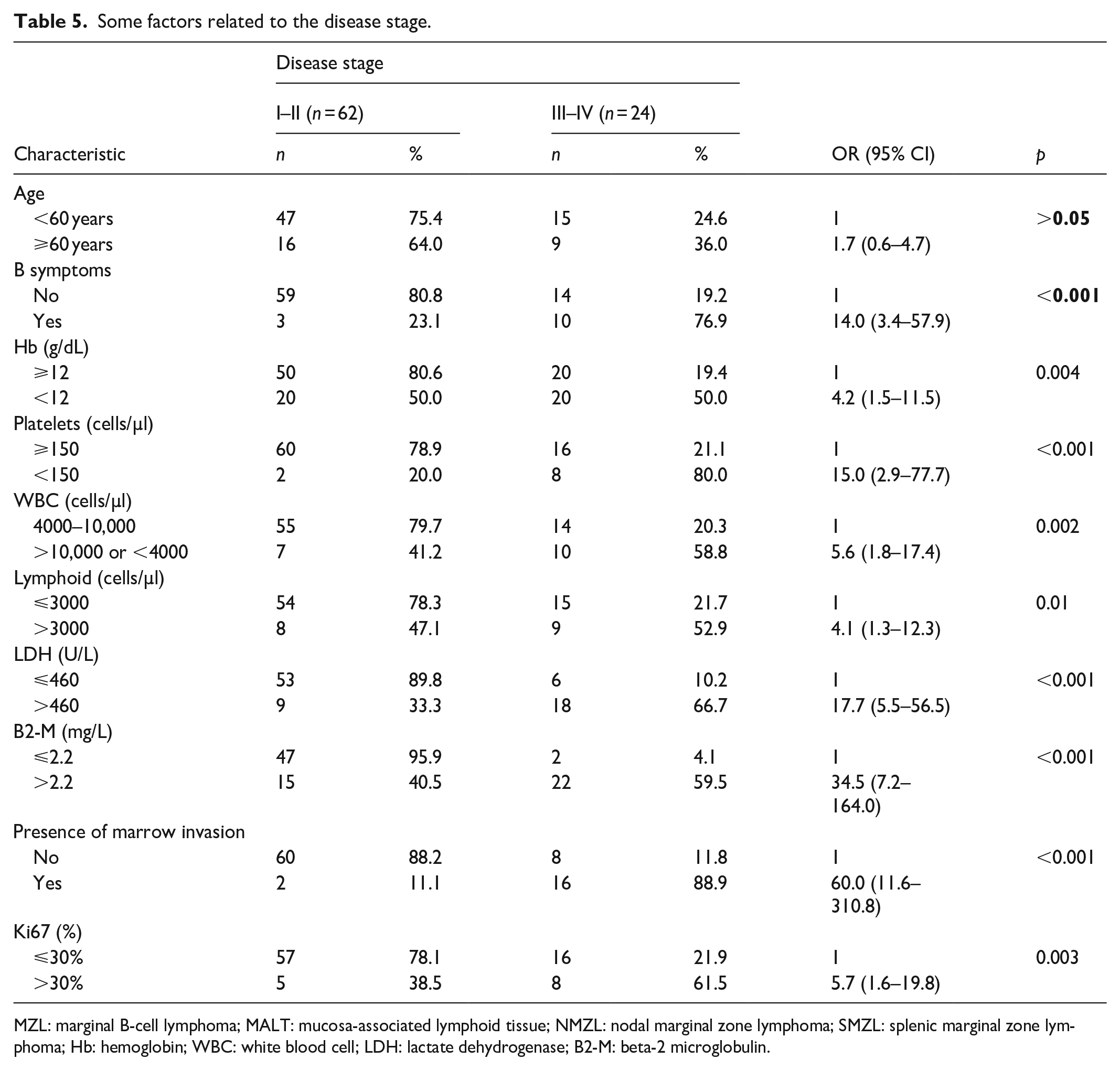
MZL: marginal B-cell lymphoma; MALT: mucosa-associated lymphoid tissue; NMZL: nodal marginal zone lymphoma; SMZL: splenic marginal zone lymphoma; Hb: hemoglobin; WBC: white blood cell; LDH: lactate dehydrogenase; B2-M: beta-2 microglobulin.
Bone marrow invasion was identified in 18 patients (20.9%), with several clinical and laboratory factors significantly associated with its occurrence. Patients aged ⩾60 years had a 3.3-fold higher likelihood of bone marrow involvement (p = 0.03). The presence of B symptoms was strongly associated with marrow invasion, with affected patients showing a 6.6-fold increased risk (p = 0.002). A hemoglobin level <12 g/dL and platelet count <150,000 cells/µL were also significant predictors, increasing the risk by 9.3-fold (p < 0.001) and 67.0-fold (p < 0.001), respectively. Abnormal WBC counts (>10 or <4 G/L) and lymphocyte counts >3 G/L were linked to 3.7-fold (p = 0.02) and 5.2-fold (p = 0.003) higher risks, respectively. Elevated LDH levels (>460 U/L) and B2-M levels (>2.2 mg/L) were among the strongest predictors, increasing the likelihood of bone marrow invasion by 14.8-fold (p < 0.001) and 40.8-fold (p < 0.001), respectively. Additionally, a Ki67 proliferation index > 30% was associated with a 4.4-fold increased risk (p = 0.02), further indicating a correlation between aggressive disease markers and bone marrow involvement (Table 6).
Some factors related to invasion of the marrow.

MZL: marginal B-cell lymphoma; MALT: mucosa-associated lymphoid tissue; NMZL: nodal marginal zone lymphoma; SMZL: splenic marginal zone lymphoma; Hb: hemoglobin; WBC: white blood cell; LDH: lactate dehydrogenase; B2-M: beta-2 microglobulin.
The likelihood of bone marrow invasion was found to be higher when hemoglobin concentration decreased to <120 g/L, platelet count decreased to <150 G/L, lymphocyte count increased to >3 G/L, LDH levels increased to >460 U/L, B2-M levels increased to >2.2 U/L, and the Ki67 index exceeded 30% (Table 6). An inverse correlation was observed between hemoglobin concentration and LDH, B2-M, and Ki67 levels. In contrast, LDH, B2-M, and Ki67 levels exhibited a positive linear correlation with each other (Table 7).
Correlation between some prognostic indicators.
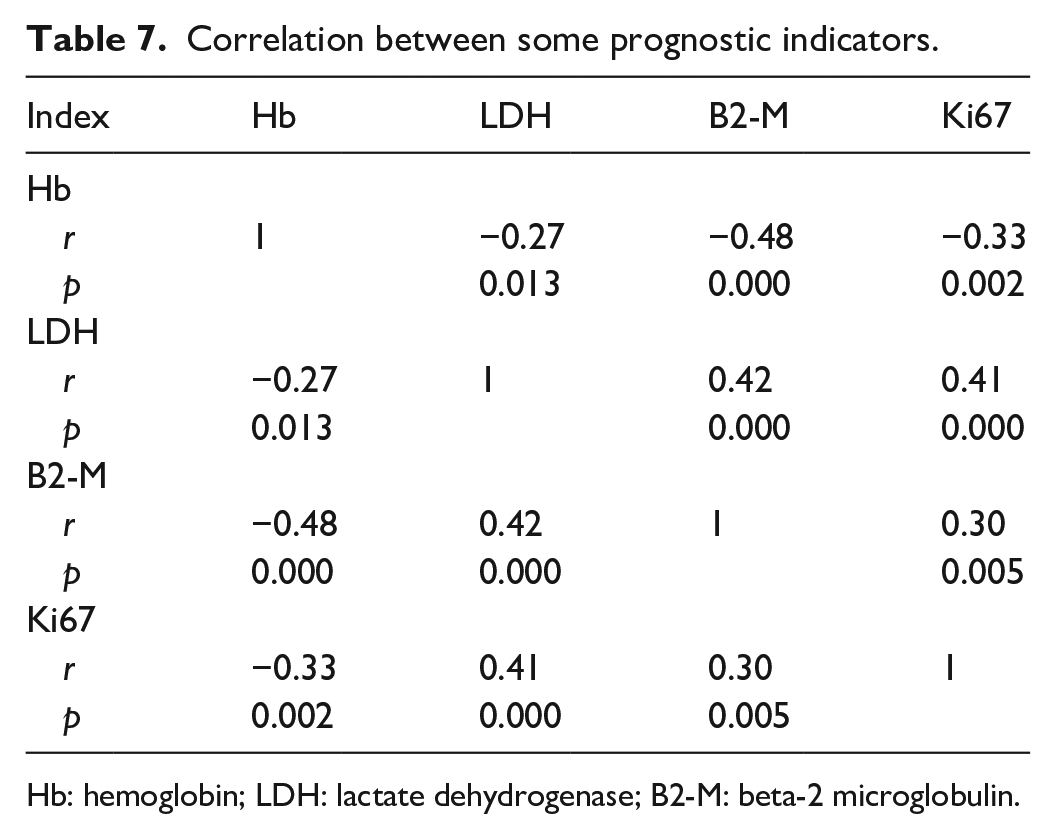
Hb: hemoglobin; LDH: lactate dehydrogenase; B2-M: beta-2 microglobulin.
Discussion
During the 10-year period from 2014 to 2024, a total of 86 cases of MZL were diagnosed and treated at the Central Institute of Hematology and Blood Transfusion. All three subtypes of MZL were identified, with EMZL accounting for the highest proportion (73.3%), followed by NMZL at 20.9%, and SMZL at 5.8%. These findings are consistent with other studies. In a study conducted in Turkey, Türkkan et al. 4 retrospectively analyzed 64 cases of MZL, reporting that EMZL accounted for 78.1%, NMZL for 21.9%, and no cases of SMZL were detected. 4 Similarly, Mazloom et al. 8 identified 275 cases of MZL, of which 77% were EMZL, 10% were NMZL, and 13% were SMZL. In Korea, Kang et al. 9 found that 70% of cases were EMZL and 30% were NMZL, with no SMZL cases reported. In the United States, Heilgeist et al. 10 studied 144 patients, detecting 67% EMZL, 22% NMZL, and 11% SMZL. Furthermore, a large-scale analysis by Olszewski and Castillo 11 involving 15,908 MZL patients showed an overall incidence of 62.1% for EMZL, 29.7% for NMZL, and 8.2% for SMZL. The predominance of EMZL has been attributed to its association with chronic infections, including Helicobacter pylori (gastric MZL), Chlamydia psittaci (ocular adnexal MZL), Borrelia burgdorferi (cutaneous MZL), hepatitis C, and HIV. 1 Genetic mutations and family history also contribute to MZL susceptibility, while environmental factors such as occupational exposure, pesticides, industrial solvents, and environmental pollutants have been implicated, as noted by Cerhan and Habermann. 1
Regarding prognosis, each MZL subtype has a specific prognostic scoring system, including MALT-IPI for EMZL, SMZLG for SMZL, and FLIPI for NMZL. Previous studies have demonstrated that these scoring systems are significantly correlated with patient survival outcomes. However, to facilitate a comparative analysis of all three subtypes, this study utilized the IPI for low-grade NHL. The results showed that the majority of patients were classified as low-risk (44.2%). The low-risk rate for the EMZL group was notably higher at 50.8%, whereas none of the SMZL patients (0%) were categorized as low-risk, with the difference being statistically significant (p < 0.05). No significant differences in risk classification were observed between NMZL and EMZL or NMZL and SMZL. MZL presents in three distinct subtypes—EMZL, NMZL, and SMZL—each characterized by unique lesion locations, clinical manifestations, and laboratory findings. Consequently, prognostic indicators such as age, disease stage, lymph node involvement, hemoglobin levels, platelet count, LDH, and B2-M levels must be tailored to each MZL subtype for an accurate risk assessment. In a study by Heilgeist et al., 10 the progression-free survival and overall survival (OS) rates for low-to-intermediate-risk patients (FLIPI scores 0–2) were 92% and 95%, respectively, compared to 56% and 62% in high-risk patients (FLIPI scores 3–5). The authors suggested that FLIPI is a more reliable prognostic tool for EMZL and SMZL, but not for NMZL. Similarly, Mazloom et al. 8 reported that IPI scores were not significantly correlated with 5-year survival, as the intermediate-low-risk group had a survival rate of 77%, compared to 100% in the high-risk group. However, FLIPI scores also did not demonstrate a strong predictive value for survival beyond 5 years, with survival rates of 91% in the low-risk group and 88% in the intermediate-risk group. These findings have led researchers to propose subtype-specific prognostic tools for each MZL variant. According to the research team, the IPI prognostic score does not adequately distinguish the clinical characteristics of EMZL, NMZL, and SMZL, emphasizing the need for further studies to identify key prognostic factors for each MZL subtype.
Factors related to disease stage
Cancer staging systems are commonly used to guide treatment decisions and predict prognosis. The Ann Arbor classification system remains the most widely used staging method for NHL, although alternative approaches are currently being explored. 12 In particular, stages III and IV disease is characterized by involvement of more than two organs, extranodal manifestations, splenic involvement, and damage to multiple tissues and organs.
Regarding age, no significant correlation was observed between patient age and disease stage in this study (Table 5). This finding differs from the study by Oh et al., 12 which analyzed 94 stage IV MZL patients and reported that only 47.9% were ⩾60 years old, whereas 52.1% were <60 years old. Another large-scale analysis by Olszewski and Castillo 11 identified age as a significant prognostic factor for MZL, with the risk of death increasing by 1.7 times for every 10-year increase in age. This trend is consistent with NHL prognosis in general and MZL prognosis in particular. Research by Knauf et al. 2 further supports this finding, showing that with every 10-year increase in age, the risk of death increases by 1.99 times, with EMZL cases showing a 2.44-fold increase and non-EMZL MZL cases increasing by 1.94 times. Similarly, Mazloom et al. 8 demonstrated that the 5-year survival rate was significantly higher in patients aged <60 years (94%) compared to those aged ⩾60 years (78%), with the difference being statistically significant (p = 0.005). Given that older patients are more likely to be diagnosed at later disease stages, their overall prognosis tends to be poorer.
Regarding B symptoms, patients presenting with these symptoms were 14 times more likely to be diagnosed at stages III–IV compared to those without B symptoms (p < 0.001, Table 5). However, in the study by Oh et al., 12 B symptoms were not a common finding, appearing in only 18.1% of stage IV patients. The presence of B symptoms has been associated with lymph node involvement, which is considered an indicator of poor prognosis. 2 According to Mazloom et al., 8 the 5-year survival rate was significantly higher in patients without B symptoms (91%) compared to those with B symptoms (41%), with a statistically significant difference (p < 0.001). In terms of OS, patients exhibiting B symptoms had a 3.76-fold increased risk of death compared to those without B symptoms (95% CI = 1.22–11.62, p = 0.021). Similarly, Olszewski and Castillo 11 found that the risk of death increased in patients with B symptoms, with rates 1.81 times higher for EMZL, 2.25 times higher for NMZL, and 1.81 times higher for SMZL. 11 However, a study by Teckie et al. 13 did not find a significant difference in recurrence risk between patients with and without B symptoms. The research team suggests that the presence of B symptoms may indicate advanced-stage disease and could serve as a potential prognostic factor for poor outcomes.
Blood test characteristics and bone marrow invasion
Patients diagnosed at stages III and IV exhibited lower hemoglobin (Hb) levels, reduced platelet counts, and higher lymphocyte counts compared to those at stages I and II (Table 5). In a study by Mazloom et al., 8 the 5-year survival rate for patients with low hemoglobin levels was 70%, significantly lower than the 91% survival rate observed in patients with normal hemoglobin levels. This finding aligns with the observation that advanced-stage disease is often accompanied by hematologic abnormalities. In MZL, lesions affect both hematopoietic and extralymphatic organs, resulting in blood test variations depending on the site of disease involvement. The study by Mazloom et al. 8 also demonstrated that anemia was present in 14% of EMZL cases, 30% of NMZL cases, and up to 70% of SMZL cases. Similarly, Oh et al. 12 reported that among stages III and IV patients, 42.2% had reduced hemoglobin levels, while 57.8% maintained normal hemoglobin levels, and 74.7% exhibited increased lymphocyte counts. This trend corresponds with the findings of the current study. The research team suggests that significant hematologic changes, particularly decreased hemoglobin concentration and increased lymphocyte counts, may serve as indicators of advanced-stage disease.
Regarding bone marrow invasion, results from bone marrow biopsy analysis revealed that patients with marrow involvement were 60.0 times more likely to be diagnosed with stages III and IV disease than those without marrow invasion (p < 0.001, Table 5). Several studies have confirmed that bone marrow infiltration on histopathological examination strongly correlates with advanced-stage MZL. 14 In a study conducted by Boveri et al. (2009), which analyzed 120 MZL patients (including 48 SMZL, 59 EMZL, and 13 NMZL cases), significant differences in bone marrow invasion rates were identified among clinical subtypes. 15 The study reported that bone marrow invasion was most common in SMZL (90%), whereas it was observed in 22% of EMZL cases and 54% of NMZL cases. These findings are consistent with those of the current study. Since the bone marrow serves as the primary site for hematopoiesis, it is among the most susceptible organs to malignant infiltration in both NHL and MZL. The research team suggests that the detection of bone marrow invasion through biopsy could serve as a critical prognostic indicator for late-stage disease progression.
LDH, B2-M, and Ki67 as predictive markers for advanced-stage MZL
Patients with elevated LDH levels (>460 U/L) and B2-M levels (>2.2 mg/L) were found to be at a higher risk of advanced-stage (III–IV) MZL (Table 5). The LDH and B2-M indices are widely recognized as key prognostic markers in both NHL and MZL, as their levels tend to increase in response to cellular damage or heightened tumor cell activity. Previous research has supported these findings; Yoo et al. 16 reported a strong correlation between elevated B2-M concentrations and stages III and IV NHL. Additionally, in a study by Mazloom et al., 8 patients with serum B2-M levels <2.5 mg/L had a 5-year OS rate of 96%, whereas those with B2-M levels ⩾2.5 mg/L had a significantly lower OS rate of 74% (p < 0.001). Further supporting this, Knauf et al. 2 found that the risk of disease progression was 2.36 times higher in EMZL cases and 2.33 times higher in non-EMZL cases when LDH levels were normal compared to cases where LDH was elevated. The authors concluded that increased LDH levels are strongly linked to disease progression. Given that MZL is a slow-growing form of NHL, the research team believes that elevated LDH and B2-M levels serve as indicators of increased tumor metabolism or disease progression.
Regarding the Ki67 index, an increase in Ki67 levels was associated with a 5.7-fold higher likelihood of being diagnosed with stages III and IV disease compared to patients with a Ki67 index ⩽30% (p < 0.05, Table 5). In a study analyzing 215 MZL cases, Hashmi et al. 17 sought to determine the optimal Ki67 cutoff value for prognostic assessment. The findings indicated that the average Ki67 index in MZL was 28.5%, and the authors emphasized its importance as an immunohistochemical marker in distinguishing early-stage from advanced-stage NHL. Since Ki67 is an intracellular antigen reflecting malignant cell proliferation, its levels are directly correlated with tumor growth rate. Further supporting this, Szczuraszek et al. 18 classified the Ki67 index on a 0–3 scale for NHL prognosis: <5% (0 points), 5%–15% (1 point), 16%–30% (2 points), and >30% (3 points). Their findings revealed a significant difference in prognosis between the Ki67 ⩽ 30% group and the Ki67 > 30% group, which aligns with the results of the present study. The research team suggests that the Ki67 index may serve as a valuable predictive marker for advanced-stage MZL.
Bone marrow invasion and related factors
Bone marrow invasion is recognized as a prognostic factor that aids in disease staging and treatment selection. Although marrow involvement is typically expected in advanced stages, its confirmation requires a bone marrow biopsy and the expertise of a pathologist to accurately interpret the specimen. Several hematological and biochemical markers, including hemoglobin, platelets, lymphocytes, LDH, B2-M, and Ki67, have been found to be significantly associated with bone marrow invasion. Specifically, the risk of marrow involvement was found to be 9.3 times higher in patients with low hemoglobin levels, 67 times higher in those with reduced platelet counts, 5.2 times higher in cases with elevated lymphocyte counts, 14.8 times higher in those with increased LDH, 40.8 times higher in those with elevated B2-M levels, and 4.4 times higher in patients with a Ki67 index >30% (Table 6). These findings are consistent with the study conducted by Kent et al., 19 which analyzed marrow invasion in 39 MZL patients, including 25 EMZL, 12 SMZL, and 2 NMZL cases. The study reported that bone marrow invasion occurred in 35% of EMZL patients, 50% of NMZL patients, and 100% of SMZL patients. In the EMZL group, low lymphocyte counts were observed in 4 out of 22 patients, whereas in the SMZL group, increased lymphocyte counts were recorded in 7 out of 10 patients with corresponding bone marrow invasion. 19 Another study by Boveri et al. (2009), which examined 120 MZL patients (48 SMZL, 59 EMZL, and 13 NMZL cases), found that bone marrow invasion was present in 90% of SMZL cases, 22% of EMZL cases, and 54% of NMZL cases. 15 The study also established a strong correlation between marrow invasion and several prognostic indicators, including disease stage (Ann Arbor classification), B symptoms, involvement of multiple lesion sites, B2-M concentration, and the IPI (p < 0.05). These findings align with those observed in the current study. Since bone marrow involvement is associated with poor prognosis, hematological and biochemical markers such as hemoglobin, LDH, B2-M, and Ki67 may serve as valuable predictors of marrow invasion and aid pathologists in confirming diagnoses.
Study limitations
Several limitations were identified in this study. First, due to the small sample sizes of NMZL (18 cases) and SMZL (5 cases), it was not possible to perform a subtype-specific analysis of prognostic factors. Second, despite the availability of separate prognostic scoring systems for each MZL subtype, the IPI score was used for comparison across all three subtypes, which may not fully capture subtype-specific prognostic differences.
Conclusion
LDH, B2-M, and Ki67 were found to be significantly associated with the prognosis of patients with MZL.
Footnotes
Ethical considerations
The authors confirm that the Ethics Committee of IRB-Hanoi Medical University, Vietnam, approved this research with number 4900/QĐ-DHYHN.
Consent to participate
Written informed consent was obtained from all subjects before the study.
Author contributions
Binh Duc Vu and Hung Quang Nguyen designed, collected, and analyzed the study. Hieu Van Nguyen helped with data collection and analysis. Cuong Ba Nguyen, Tuong Quang Le, Anh Vu-Bao Nguyen, Tai Phu Le, and Thanh Hoang Nguyen contributed to the study design and helped interpret the results. All authors contributed to writing the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is available from the corresponding author on request.