
Abstract
Objectives:
While existing research has indicated a potential link between gastroesophageal reflux disease (GERD) and chronic suppurative otitis media (CSOM), these findings primarily stem from observational studies, which are inherently limited by confounding variables and methodological biases, thereby reducing their reliability. This research sought to elucidate the causative link between GERD and CSOM.
Methods:
A two-sample bidirectional Mendelian randomization (MR) study was conducted using genetic data to assess the causal relationship between GERD and CSOM. Pooled genetic data for GERD and CSOM were obtained from published genomewide association studies. Independent single nucleotide polymorphisms, rigorously screened as instrumental variables, were used in the analysis. The primary analytical method was inverse variance weighting (IVW), with additional sensitivity analyses performed to assess the robustness and reliability of the results.
Results:
Per MR analysis, genetically predicted GERD positively associated with an increased CSOM risk (IVW: p = 0.001, odds ratio = 2.08, 95% confidence interval: 1.33–3.27). Per reverse MR analysis, genetically predicted CSOM did not associate with an increased GERD risk. Sensitivity analyses did not identify horizontal pleiotropy or heterogeneity.
Conclusions:
For the first time, GERD was identified as a risk factor for CSOM through a bidirectional MR study. This finding provides high-level causal evidence for the prevention and management of CSOM and forms a basis for future clinical and mechanistic studies. Clinicians should consider the potential impact of GERD when treating patients with CSOM, as GERD may be an important risk factor.
Keywords
Introduction
Chromic suppurative Otis media (CSOM) represents a frequent clinical entity in otology, defined by chronic inflammatory changes within the middle ear cavity or mastoid structures. It can lead to progressive hearing loss and potentially permanent disability, which can considerably impair patients’ quality of life.1 –4 Gastroesophageal reflux disease (GERD) is a prevalent upper gastrointestinal disorder in which gastric contents reflux into the esophagus, causing symptoms such as heartburn and acid regurgitation, along with complications. 5 A previous observational study has suggested a potential association between GERD and CSOM 6 ; however, these studies are susceptible to confounding factors and reverse causality, resulting in inconclusive or inaccurate outcomes.
In clinical practice, CSOM treatment focuses on controlling infection and clearing pathological secretions from the middle ear; however, the underlying pathogenesis of the condition remains insufficiently understood. As prior observational studies have not provided strong causal evidence to inform treatment strategies, clarifying the relationship between GERD and CSOM is essential for optimizing therapeutic approaches. Establishing a causal link between GERD and CSOM could provide clinicians with new insights into CSOM management. Additionally, this research may help reduce the incidence and burden of CSOM in patients with GERD through early screening and preventive measures. Therefore, investigating the GERD–CSOM relationship has important implications for both clinical practice and public health interventions.
Mendelian randomization (MR) leverages genetic polymorphisms as instrumental variables to infer causal associations, thereby circumventing biases inherent in conventional observational designs.7 –9 Genetic variants are randomly assigned at conception and are independent of environmental and lifestyle factors, thereby reducing the risk of confounding. Additionally, since genetic variants are present before disease onset, they help mitigate reverse causality. MR studies can, therefore, provide a more accurate assessment of the causal relationship between GERD and CSOM, offering a stronger basis for clinical prevention and treatment. 10
To date, the relationship between GERD and CSOM has not been investigated through genetically based studies. This study aimed to address this gap by using a bidirectional MR design to clarify the causal relationship between GERD and CSOM and provide new evidence for the prevention and management of CSOM. Clinically, understanding the GERD–CSOM relationship could deepen insights into CSOM pathogenesis and suggest new approaches for its treatment.
Methods
Study design
Figure 1 illustrates the design process of the bidirectional MR analysis. The MR study was based on three key assumptions 11 : (1) a robust association between genetic variants and the exposure of interest; (2) genetic variants are unaffected by confounding factors; (3) the genetic variants impact the outcome exclusively via the exposure pathway. This study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology using MR guidelines. 12

Overview of the general design of our Mendelian randomization study.
Data sources and single-nucleotide polymorphism selection for GERD and CSOM
Given the large number of SNPs tested in GWAS for GERD and CSOM, a more stringent significance threshold is necessary. With approximately 1,000,000 tested SNPs, the Bonferroni-corrected p-value threshold is 0.05/1,000,000 = 5 × 10−8. We used this genomewide significance threshold of p < 5 × 10−8 to identify SNPs significantly associated with the phenotype, 13 excluding SNPs with linkage disequilibrium (R2 < 0.001) and palindromic sequences (Table 1).
Details of data sources of study.

To improve SNP selection reliability, the MR-PRESSO test was employed to detect and remove SNPs associated with horizontal pleiotropy. When permissible under MR analysis, the threshold was relaxed to p < 5 × 10−6, and SNPs with chain disequilibrium (R2 < 0.001) and palindromic sequences were also excluded. The R2 threshold of <0.001 ensures minimal linkage disequilibrium and reduces the risk of horizontal pleiotropy problems.
Bidirectional two-sample MR analysis
A two-sample MR analysis was conducted to investigate the causal relationship between GERD and CSOM. Inverse variance weighting (IVW), a commonly used meta-analysis method, was employed as the primary analysis. IVW improves causal effect estimation by weighting each SNP according to its effect size and variance. A random-effects model was applied to account for SNP heterogeneity and ensure robust causal estimates. 14
Sensitivity analyses—including the weighted median method, MR-Egger method, leave-one-out analysis, Cochran’s Q test (for SNP heterogeneity), and the MR-Egger intercept test (for horizontal pleiotropy)—were performed to validate the robustness of the findings.15 –18 Scatter plots were used to illustrate causal effects and funnel plots were employed to assess IV heterogeneity.
In the bidirectional MR analysis, two independent tests were conducted to evaluate the causal relationship between GERD and CSOM. To control the overall false-positive rate at 5% (0.05), Bonferroni correction was applied, setting the significance threshold at p < 0.025 (0.05/2). p-values between 0.025 and 0.05 were considered suggestive of potential associations.
Statistical Analysis
All statistical analyses were conducted using the “Two Sample MR” and “MR-PRESSO” packages in R (version 4.2.3, R Foundation for Statistical Computing, Vienna, Austria). The F-statistic was calculated using the formula F = Beta2/Se2. 19 SNPs with F-statistics greater than 10 were selected, as this threshold is commonly used to ensure strong IVs.
Results
Characterization of the selected SNP
We identified 80 SNPs significantly associated with GERD and ultimately selected 75 SNPs as IVs for GERD (Supplemental Table S1).The detailed information of the screened SNPs in the outcome gene data shows that the p-values of these SNPs are not significant, indicating that they are not related to the outcome as instrumental variables (Supplemental Table S3). For the reverse MR analysis, we identified three SNPs as IVs for CSOM (Supplemental Table S2). All IVs had F-statistics greater than 10, indicating strong associations with their respective exposure.
Causal relationship between GERD and COSM
MR analysis revealed that genetic liability to GERD significantly elevated CSOM susceptibility (IVW OR = 2.09, 95% CI: 1.33–3.27; p = 0.001). The weighted median method results were consistent with those from the IVW analysis; in contrast, the MR-Egger test did not yield statistically significant results. No substantial horizontal pleiotropy was detected, so the random-effects IVW model was considered the primary analytical result (Figure 2). Scatter plots depicting the association between GERD and CSOM are shown in Supplemental Figure S1.
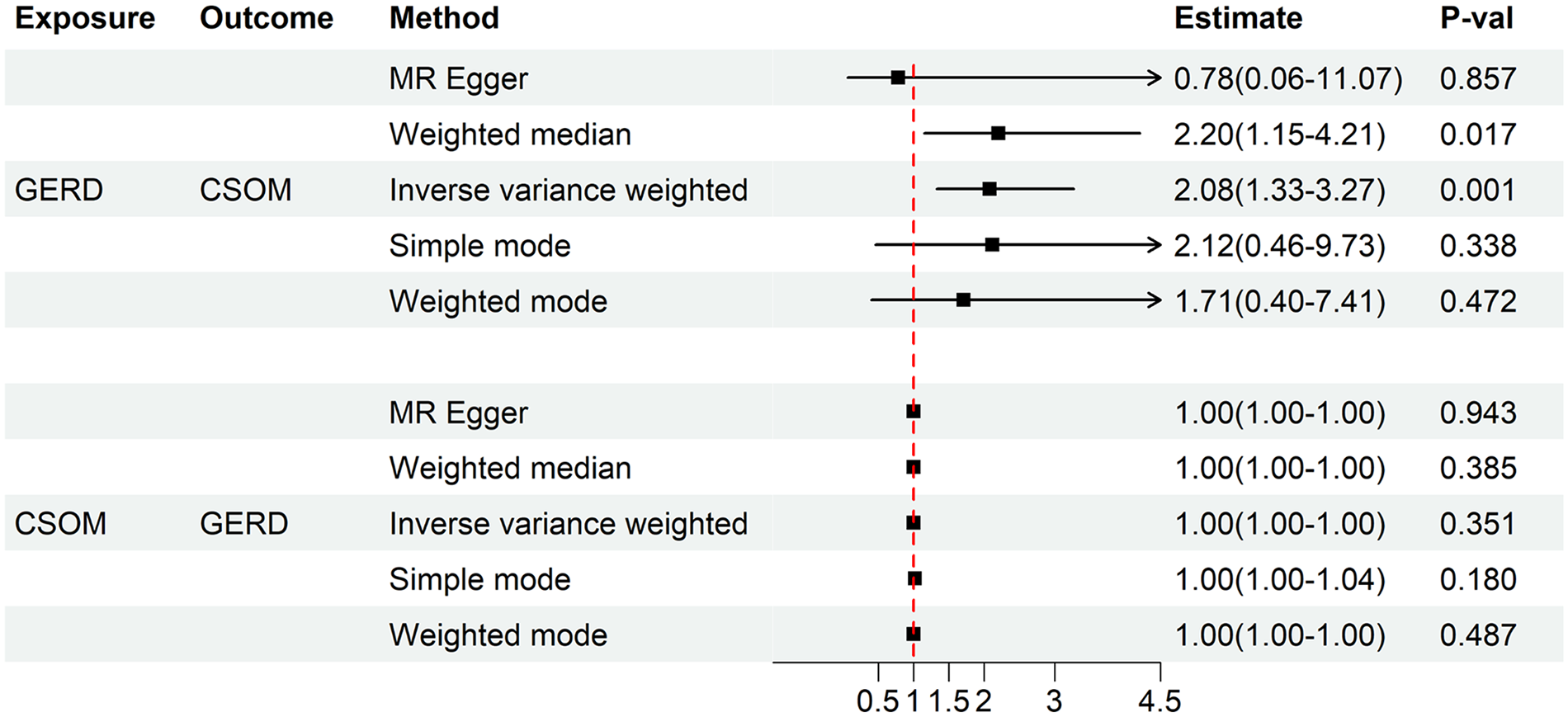
Causal relationship between GERD and CSOM.
Causal relationship between CSOM and GERD
In the reverse analysis, we found no significant association between genetically predicted CSOM and GERD risk (IVW: p = 0.35, OR = 1.00, 95% CI: 0.99–1.00). Although the three selected SNPs had high F-statistics, suggesting strong associations with CSOM, using only three SNPs as IVs may not fully capture the genetic variation underlying CSOM. This limitation IVs may have affected our ability to detect any potential causal effect of CSOM on GERD. Future studies with larger sample sizes and more comprehensive genetic data are needed to further explore this relationship.
Sensitivity analysis
The MR-PRESSO test did not detect any SNPs with significant horizontal pleiotropy in either causal analysis (Supplemental Table S4), supporting the reliability of our results. The MR-Egger intercept method showed an intercept of 0.03 (standard error = 0.04, p = 0.46) for the GERD-to-CSOM analysis and an intercept of 0.01 (standard error = 0.004, p = 0.42) for the CSOM-to-GERD analysis, indicating no significant horizontal pleiotropy.
Cochran’s Q test indicated no heterogeneity in the GERD-to-CSOM analysis (Q = 65.48, 73 degrees of freedom, p = 0.72) or the CSOM-to-GERD analysis (Q = 0.08, 1 degree of freedom, p = 0.78). The results of the tests for pleiotropy and heterogeneity are shown in Table 2. A leave-one-out analysis showed that no single SNP significantly impacted the overall results (Supplemental Figure S2), confirming the robustness of our findings.
Heterogeneity test and pleiotropy test.

GERD: gastroesophageal reflux disease; CSOM: Chronic suppurative otitis media; SE: standard error.
Finally, funnel plots were constructed to assess IV heterogeneity (Supplemental Figure S3). No significant asymmetry was observed, indicating that our results were not influenced by publication bias.
Discussion
In this study, we employed bidirectional MR to explore the causal relationship between GERD and CSOM. Our findings demonstrate a significant association between genetically predicted GERD and an increased risk of CSOM. However, reverse MR analysis showed no significant association between genetically predicted CSOM and GERD risk, tentatively confirming a unidirectional causal relationship between GERD and CSOM.
CSOM is a common condition in clinical practice that primarily results from acute otitis media. The condition may lead to the invasion of the middle ear mucosa, ossicles, or even the bone, causing irreversible damage and becoming a significant cause of preventable hearing loss.20 –22 Treatment typically involves surgery, with complications such as taste loss, labyrinthine fistulae, facial paralysis, and intracranial issues. 23 The associated hearing loss and treatment burden can significantly impact patients’ quality of life, emphasizing the importance of disease prevention.
Previous research has explored the relationship between pharyngeal reflux and middle ear disease. Han and Lv 24 found that 77.4% of 31 patients with COM had positive Ryan scores. Lechien et al. 25 analyzed 1624 pediatric and 144 adult patients with OM, reporting LPR and GERD prevalences to be 28.7% and 40.7%, respectively. Despite similarities with pharyngeal reflux, limited research has focused on the effects of GERD on CSOM. A study from the Middle East reported that 72.4% of 58 patients with COM had GERD, 26 aligning with our findings. However, that study identified only a correlation; in contrast, our MR study addressed confounding factors and reverse causality to establish causality.
GERD may contribute to CSOM through several mechanisms. One possible pathway involves the reflux of gastroesophageal contents, leading to eustachian tube dysfunction. GERD symptoms such as acid reflux, nausea, vomiting, and heartburn stem from esophageal mucosa damage by activated pepsin. 27 Unlike the esophageal mucosa, the nasopharyngeal and eustachian tube mucosae are more susceptible to damage from gastric acid and pepsin due to a lack of protective barriers and bicarbonate neutralization. 28 Animal studies have demonstrated that repeated exposure to pepsin in hydrochloric acid impair eustachian tube function in rats. 29 Eustachian tube dysfunction is widely considered the first step in the development of ear diseases, including CSOM. 30 This dysfunction causes negative middle ear pressure, which may lead to irreversible tympanic membrane and middle ear mucosal damage, contributing to CSOM development. 31
Gastric contents can also directly damage the middle ear mucosal. Abdel-Aziz et al. 32 found higher pepsin concentrations in middle ear effusions than in plasma in patients with COM. Tasker et al. 33 reported that 91% of the middle ear exudates contained pepsin, with concentrations exceeding serum levels. Klokkenburg et al. 34 detected bile acids in 32% of middle ear effusions, with concentrations 3.1–19.7 times higher than serum levels. Under negative pressure, gas absorption in the tympanic cavity may induce microaspiration through the eustachian tube, allowing gastric contents to reach the middle ear. Once there, pepsin hydrolyzes peptide bonds and disrupts tight junction proteins, causing mucosal epithelial damage. 35 These contents may also elevate cytokine levels such as those of IL-5, IL-8, and IL-1α, recruiting immune cells and triggering inflammation. 36 Huo et al. 37 showed that refluxing acid and bile salts generate reactive oxygen species, promoting pro-inflammatory cytokine production and triggering GERD-associated inflammation. A similar mechanism may drive middle ear inflammation, exacerbating CSOM. Inflammation of the middle ear mucosa can impair eustachian tube function, creating a vicious cycle of disease progression. 38
To the best of our knowledge, our study is the first to identify the genetic influence of GERD on CSOM pathogenesis, providing high-quality evidence for a causal relationship and laying a foundation for future clinical and mechanistic studies. Poelmans et al., 39 demonstrated that antacid therapy significantly improved otitis media symptoms in 217 patients with otitis media and reflux symptoms. This underscores the importance of considering GERD treatment in patients with CSOM, particularly those with refractory or recurrent CSOM. Our findings also highlight the potential value of implementing CSOM risk screening in patients with GERD. Early identification and management of GERD may improve patient prognosis and reduce the burden of CSOM. Future studies could explore the effective implementation of these screening programs in clinical practice and investigate public health interventions aimed at reducing CSOM incidence. Hearing screening for patients with GERD could enable early detection and intervention for middle ear disease. However, it is premature to recommend widespread screening or intervention based solely on MR findings. Further basic research is needed to clarify the specific mechanisms by which GERD contributes to CSOM.
Our study has several strengths. Unlike traditional observational studies, this MR study explored bidirectional causality between GERD and CSOM, controlling for confounders and reverse causality. The robustness and reliability of our findings were ensured through rigorous IV selection and multiple sensitivity analyses. Additionally, we used data from distinct GWAS sources to prevent sample overlap.
Nonetheless, this study has some limitations. Our study population was limited to European adults, limiting the generalizability of our findings to other ethnic groups and children. Additionally, the lack of a multisample meta-analysis slightly reduces the strength of our conclusions, necessitating cautious interpretation.
Conclusions
To our knowledge, this represents the inaugural application of bidirectional Mendelian randomization (MR) methodology in exploring the causal interplay between GERD and CSOM. Our findings suggest that genetically predicted GERD may increase the risk of developing CSOM, offering new insights into CSOM’s etiology and identifying GERD as a potential risk factor.
Although this study provides preliminary evidence of a causal link between GERD and CSOM, validation in larger and more diverse populations is necessary. Subsequent studies ought to prioritize mechanistic explorations to unravel the biological pathways connecting GERD and CSOM, which could enhance our understanding of GERD’s role in CSOM pathogenesis and provide a stronger foundation for clinical prevention and treatment strategies.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251332151 – Supplemental material for Causal relationship between gastroesophageal reflux disease and the risk of chronic suppurative otitis media: a mendelian randomization analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121251332151 for Causal relationship between gastroesophageal reflux disease and the risk of chronic suppurative otitis media: a mendelian randomization analysis by Qianyou Zheng, Ce Wu, Yaru Li, Jing Wu, Wenrui Tang, Qiuyang Zhu, Shaokang Ren, Xiaowen Zhang, Shenling Li and Tao Fu in SAGE Open Medicine
Footnotes
Acknowledgements
Ethical considerations
This study utilized publicly available data from genomewide association studies (GWASs). The original GWASs received relevant agency approval, waiving the need for informed consent and ethical approval for this study.
Author contributions / CRediT
Qianyou Zheng (First Author): Writing-Original, Conceptualization, Investigation, Softwate; Ce Wu: Data Curation, Formal Analysis, Software, Writing-Review; Yaru Li: Methodology, Validation; Jing Wu: Investigation, Resources; Wenrui Tang: Software, Resources; Qiuyang Zhu: Software, Resources; Shaokang Ren: Investigation, Resources; Xiaowen Zhang: Supervision, Writing-Review; Shenling Li: Validation, Writing-Review; Tao Fu (Corresponding Author): Writing-Review, Supervision.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Gastroesophageal reflux disease (GERD) data were sourced from genomewide association studies (GWAS)
1
conducted at the Berghof Institute for Medical Research, primarily using data from the UK Biobank (www.ukbiobank.ac.uk) and the Qskin study.
2
These cohorts included 78,707 patients with GERD and 288,734 controls. The UK Biobank is a comprehensive biomedical database with over 500,000 participants, covering genetic and phenotypic data; in contrast, the QSkin study investigates genetic and environmental factors in skin cancer and other health conditions. GWAS data for chronic suppurative otitis media (CSOM) were obtained from the FinnGen database, which classified cases and controls according to the International Classification of Diseases, 10th edition (ICD-10). The CSOM dataset included 2101 cases and 352,571 controls. Detailed data sources are summarized in ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.