
Abstract
Objective:
Previous observational studies reported that ankylosing spondylitis is closely related to hypertension. However, it is still controversial whether the association between ankylosing spondylitis and hypertension is causal. The effects of ankylosing spondylitis on diastolic and systolic blood pressure deserve further investigation. The objective of our study is to explore whether ankylosing spondylitis is causally associated with blood pressure.
Methods:
A bidirectional two-sample Mendelian randomization (MR) analysis was performed by employing five Mendelian randomization analysis methods. MR Egger regression, weighted median, inverse variance weighted, and weight mode methods were performed in the two-sample Mendelian randomization analysis. We performed Mendelian randomization to investigate the association between ankylosing spondylitis (finn-b-M13_ANKYLOSPON) and hypertension (ukb-b-14057), diastolic blood pressure (ebi-a-GCST90000062) and systolic blood pressure (ebi-a-GCST90000059). We also performed reverse Mendelian randomization between exposures and outcomes. Another new validation cohort (ukb-b-18194) was also performed. The heterogeneity, horizontal pleiotropy, and possible outliers were examined in the MR analysis results.
Results:
The inverse variance weighted results showed that ankylosing spondylitis has no genetic causal relationship with hypertension (p = 0.441, OR = 1.001, 95% CI: 0.999–1.002). The inverse variance weighted results showed that ankylosing spondylitis has no genetic causal relationship with systolic blood pressure (p = 0.301, OR = 1.006, 95% CI: 0.995–1.018). The inverse variance weighted results showed that ankylosing spondylitis has no genetic causal relationship with diastolic blood pressure (p = 0.778, OR = 1.002, 95% CI: 0.988–1.016). The reverse Mendelian randomization between exposures and outcomes is negative. Another new validation cohort also confirmed the results. No heterogeneity was observed by the MR-pleiotropy residual sum and outlier test. The “leave-one-out” analysis indicated that the results of MR analysis were not affected by a single nucleotide polymorphism.
Conclusion:
This study represents the first two-sample Mendelian randomization analysis aimed at investigating the causal genetic relationship between ankylosing spondylitis and blood pressure. Our Mendelian randomization analysis results revealed a lack of causal association between ankylosing spondylitis and hypertension, diastolic blood pressure, as well as systolic blood pressure.
Background
Ankylosing spondylitis (AS) is a chronic systemic inflammatory disease that primarily affects the axial skeleton, including the spine and sacroiliac joints. 1 The etiology of AS is unknown, and there is still a lack of effective treatment. 2 The previous studies have primarily focused on the impact of AS on the skeletal system, whereas recent research indicates that this disorder also exerts significant effects on the cardiovascular system. Studies have reported that patients with AS have an approximately 40% higher risk of cardiovascular disease. 3 Patients with AS may develop complications such as arteriosclerosis, arrhythmia, and aortic hypertrophy. In the study of Lin et al., 4 the incidence of acute coronary syndrome in AS was 1.787 times higher than that in the normal population.
Previous studies have reported an increased risk of elevated blood pressure in AS. Chen et al. 5 found a positive correlation between systolic blood pressure and Bath AS Metrology Index in AS through a cohort study. Candemir et al. 6 found that the systolic blood pressure in AS patients at night was significantly higher (108 ± 10 vs 101 ± 10 mmHg, p = 0.044). Haroon et al. 7 performed a population-based study and found that hypertension were more common in AS (23.2% vs 17.8%). The inflammatory environment of AS may cause vascular endothelial cell damage and reduce vascular elasticity, which may lead to hypertension.8,9 However, some studies suggest that there is no correlation between AS and hypertension.10,11
Traditional observational studies often cause bias due to the limited sample size, and the experimental results are difficult to avoid the interference of confounding factors. 12 Single nucleotide polymorphisms (SNPs) were used as instrumental variables (IVs) in the Mendelian randomization analysis to detect the causal relationships between exposure factors and outcomes, which can effectively reduce the interference of confounding factors. 13 To the best of our knowledge, Mendelian randomization has not been used to detect the association between AS and blood pressure. In this study, we applied bidirectional two-sample Mendelian randomization to investigate whether there is a causal relationship between the AS and blood pressure.
Material and methods
Study design
In this study, SNPs were defined as IVs and SNPs were selected from the genomewide association study (GWAS) database. The three basic principles of two-sample Mendelian randomization were strictly followed during this study: (1) All the selected IVs were closely correlated with exposure, and the relevant statistical parameters were set as p < 5 × 10−8 and F-statistic > 10; (2) All the selected IVs were independent between exposure and outcome factors; (3) All selected IVs effect outcome through exposure, the interaction between the two factors is direct and does not go through other pathways. F-statistics were calculated using the formula: F = R2(N − K − 1)/[K(1 − R2)]. K is the number of SNP-exposure association, and N is the sample size of the GWAS for the SNP-exposure association. 13 All the data in this article can be found in online repositories. The GWAS studies had previously gained ethical approval, and the present analysis was based on publicly available data, which did not need additional approval of the ethics committee. In this study the threshold of p < 5 × 10−8 for selection of IVs is robust and only 13 SNPs were available. Therefore, we choose p < 5 × 10−6 as the selection of IVs.
The selection of GWAS summary data for AS
GWAS summary data of AS were obtained from FINNGEN (r11.finngen.fi). The GWAS ID is “finn-b-M13_ANKYLOSPON” and the dataset comprised 166,324 European participants and 16,380,022 SNPs. 14 The validation cohort of AS was summarized from the UKbiobank (www.nealelab.is/uk-biobank). The GWAS ID is “ukb-b-18194” and the dataset comprised 462,933 subjects of European ancestry. 14 In order to reduce the impact of linkage disequilibrium (LD), the LD of SNPs that are highly associated with AS, and r2 has to meet the condition that lower than 0.001.
The selection of GWAS summary data for hypertension
GWAS summary data of hypertension were obtained from the UKbiobank (www.nealelab.is/uk-biobank). The GWAS ID is “ukb-b-14057,” and the dataset comprised 119,731 cases and 343,202 controls from 462,933 subjects of European ancestry. This dataset contained 9,851,867 SNPs. 14 The validation cohort of hypertension was summarized from European Molecular Biology Laboratory (EMBL, www.ebi.ac.uk/). The GWAS ID is “ebi-a-GCST90038604,” and the dataset comprised 484,598 subjects of European ancestry. 14 The M13 code in the International Classification of Diseases-10th Revision was used to define the included cases. Detailed information can be found on the UKbiobank website.
The selection of GWAS summary data for diastolic blood pressure
GWAS summary data of diastolic blood pressure was obtained from the UKbiobank (www.nealelab.is/uk-biobank). The GWAS ID is “ebi-a-GCST90000062” and the dataset comprised 810,865 subjects of European ancestry. This dataset contained 236,549 SNPs. 14 The validation cohort of diastolic blood pressure was summarized from EMBL (www.ebi.ac.uk/). The GWAS ID is “ieu-b-39,”and the dataset comprised 757,601 subjects of European ancestry. 14
The selection of GWAS summary data for systolic blood pressure
GWAS summary data of systolic blood pressure was obtained from the UKbiobank (www.nealelab.is/uk-biobank). The GWAS ID is “ebi-a-GCST90000059,” and the dataset comprised 810,865 subjects of European ancestry. This dataset contained 236,550 SNPs. 14 The validation cohort of systolic blood pressure was summarized from EMBL (www.ebi.ac.uk/). The GWAS ID is “ieu-b-4818,” and the dataset comprised 97,656 subjects of European ancestry. 14
The protocol for conducting MR analysis
First, we explored the genetic association between AS and hypertension. To further explore the effect of AS on blood pressure, we explored the genetic association between AS and systolic blood pressure, AS and diastolic blood pressure, respectively. In order to verify the reliability of our conclusions, we used another set of GWAS summary dates for validation. Finally, reverse Mendelian randomization was conducted to investigate the upstream and downstream regulatory mechanisms between the two groups. Figure 1 shows the protocol of Mendelian randomization.

The flow chart depicting the analysis of Mendelian randomization.
Statistical analysis
The “TwoSample MR” package in the R software (version 4.2.3, it is supported by the R Foundation for Statistical Computing, which is a non-profit organization based in Vienna, Austria.) was used to perform the two-sample MR analysis. The inverse variance weighted (IVW) was used as the main method, and the MR Egger, weighted median, simple mode, and weighted modes were used as supplementary methods. The IVW presupposes that all single-nucleotide polymorphisms are valid IVs, which can get the most accurate experimental results. 15 MR-Egger regression was used to evaluate the bias. When the intercept term has no statistically significance, the slope of MR-Egger’s regression represents the estimated value of the causal effect of the exposure on the outcome. 16 If half of the single-nucleotide polymorphisms were valid IVs, weighted median and weighted modes were used to predict the possible experimental results. 17 We accounted for multiple testing by applying a Bonferroni correction for the number of outcomes, resulting in p < 0.05/6 = 0.008 when blood pressure were considered as outcomes, and p < 0.05/2 = 0.025 when considering the AS as outcomes.
Heterogeneity and sensitivity test
The Cochran’s Q statistic for IVW analysis and Rucker’s Q for MR Egger were used to detect the heterogeneity of the MR results, with p > 0.05 indicating that there was no heterogeneity.18,19 Significant heterogeneity was indicated if p < 0.05, and a random-effect model would be adopted in the subsequent analyses, otherwise, a fixed-effect model would be adopted. When the intercept term has no statistically significance, the slope of MR-Egger’s regression represents the prediction of the possible experimental results.18,19 When the p-value in the MR-Egger regression is less than 0.05, the MR pleiotropy residual sum and outlier (MR-PRESSO) method was used to predict outlier single-nucleotide polymorphisms and potential horizontal pleiotropy. 20 The MR-PRESSO analysis can detect outliers, and the global test can detect horizontal pleiotropy, and p > 0.05 indicating that there is no horizontal pleiotropy. 21 A “leave-one-out” analysis was performed to indicate whether the causal relationship was affected by a SNP. 22 Figure 1 shows the flowchart of Mendelian randomization.
Results
MR analysis of AS and hypertension
We performed the MR analysis between AS and hypertension. Significant heterogeneity (Q = 67.493, p < 0.05) was found via the Cochran’s Q test, a random-effect model would be adopted in the analysis. The IVW (multiplicative random effects) results showed that AS had no genetic causal relationship with hypertension (p = 0.441, OR = 1.001, 95% CI: (0.999–1.002). In the reverse MR analysis, the heterogeneity was also significant. The IVW (multiplicative random effects) results showed no genetic causal between hypertension (p = 0.791, OR = 1.098, 95% CI: 0.549–2.199) (Table 1).
Causal estimates for the bidirectional Mendelian randomization between AS and blood pressure.

After conducting the validation cohort analysis, we observed no significant correlation between AS and hypertension. The IVW (multiplicative random effects) results showed no genetic causal between AS and hypertension (p = 0.056, OR = 2.749, 95% CI: 0.973–7.769). The IVW (multiplicative random effects) results showed no genetic causal between hypertension and AS (p = 0.531, OR = 0.999, 95% CI: 0.997–1.002) (Table 2).
Causal estimates for the bidirectional Mendelian randomization between AS and blood pressure using the validation cohort date.
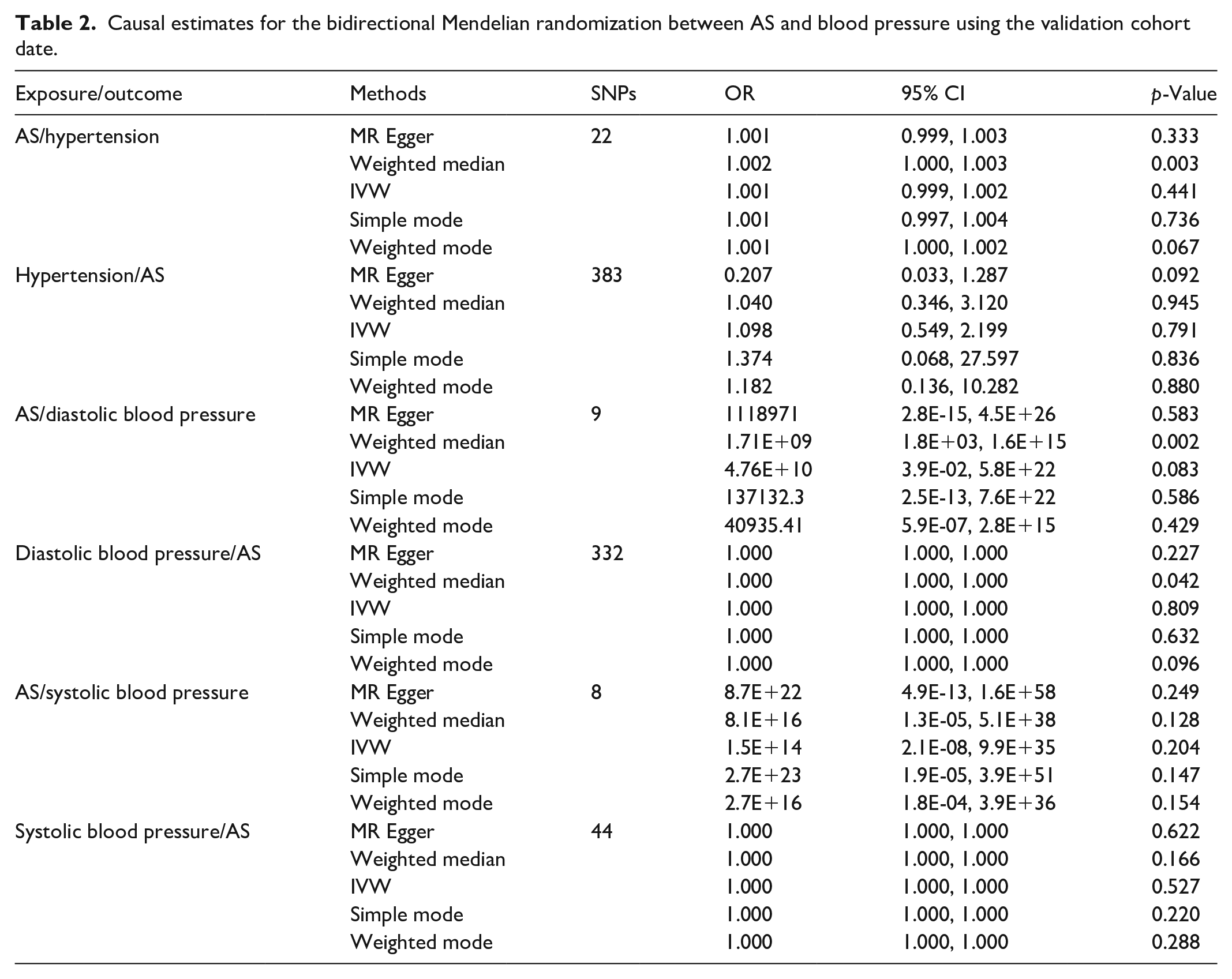
No directional pleiotropy was found in the MR-Egger regression between AS and hypertension (intercept = 0.000, se = 0.001, p = 0.529) and MR-PRESSO Global test (p = 0.628). In the same way no directional pleiotropy was found in the MR-Egger regression between hypertension and AS (intercept = 0.013, se = 0.008, p = 0.054) and MR-PRESSO Global test (p = 0.128). In the validation cohort analysis, no directional pleiotropy was found in the MR-Egger regression and MR-PRESSO Global test (Figures 2–5).

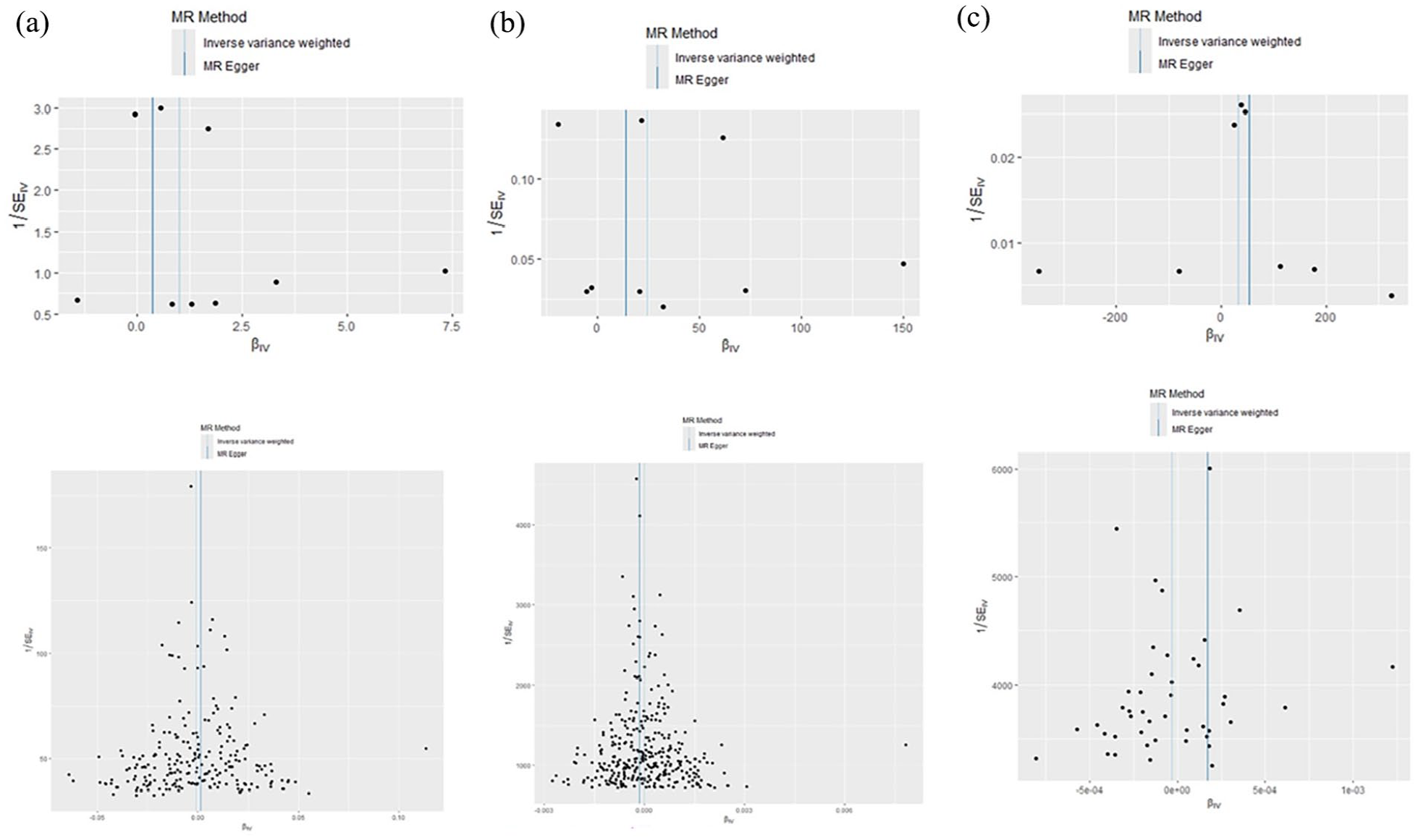
The scatter plot of the Mendelian randomization results. The slope of each line corresponding to the estimated MR effect in different models. (a) AS on hypertension, (b) AS on diastolic blood pressure, and (c) AS on systolic blood pressure.

Funnel plots of Mendelian randomization results. The funnel plots show the inverse variance weighted MR estimate of different models. (a) AS on hypertension, (b) AS on diastolic blood pressure, and (c) AS on systolic blood pressure.

The scatter plot of the Mendelian randomization results using the validation cohort date. (a) hypertension on AS, (b) diastolic blood pressure on AS, and (c) systolic blood pressure on AS.
Funnel plots of Mendelian randomization results using the validation cohort date. (a) hypertension on AS, (b) diastolic blood pressure on AS, and (c) systolic blood pressure on AS.
MR analysis of AS and diastolic blood pressure
We performed the MR analysis between AS and diastolic blood pressure. Significant heterogeneity (Q = 53.550, p < 0.05) was found via the Cochran’s Q test, a random-effect model would be adopted in the analysis. The IVW (multiplicative random effects) results showed that AS had no genetic causal relationship with diastolic blood pressure (p = 0.778 OR = 1.002, 95% CI: 0.988–1.016). In the reverse MR analysis, the IVW results showed no genetic causal between diastolic blood pressure (p = 0.400 OR = 0.903, 95% CI: 0.711–1.462). After conducting the validation cohort analysis, we observed no significant correlation between AS and diastolic blood pressure (Tables 1 and 2).
No directional pleiotropy was found in the MR-Egger regression between AS and diastolic blood pressure (intercept = −0.004, se = 0.010, p = 0.724) and MR-PRESSO Global test (p = 0.796). In the same way, no directional pleiotropy was found in the MR-Egger regression between diastolic blood pressure and AS (intercept = 0.024, se = 0.018, p = 0.240 and MR-PRESSO Global test (p = 0.124). In the validation cohort analysis, no directional pleiotropy was found in the MR-Egger regression and MR-PRESSO Global test (Figures 2–5).
MR analysis of AS and systolic blood pressure
We performed the MR analysis between AS and systolic blood pressure. Significant heterogeneity (Q = 28.703, p < 0.05) was found via the Cochran’s Q test, and a random-effect model would be adopted in the analysis. The IVW (multiplicative random effects) results showed that AS had no genetic causal relationship with systolic blood pressure (p = 0.301, OR = 1.006, 95% CI: 0.995–1.018). In the reverse MR analysis, the IVW results showed no genetic causal between systolic blood pressure (p = 0.671, OR = 0.903, 95% CI: 0.564–1.445). After conducting the validation cohort analysis, we observed no significant correlation between AS and systolic blood pressure (Tables 1 and 2).
No directional pleiotropy was found in the MR-Egger regression between AS and diastolic blood pressure (intercept = −0.006, se = 0.007, p = 0.500) and MR-PRESSO Global test (p = 0.886). In the same way, no directional pleiotropy was found in the MR-Egger regression between diastolic blood pressure and AS (intercept = 0.015, se = 0.008, p = 0.063 and MR-PRESSO Global test (p = 0.457). In the validation cohort analysis, no directional pleiotropy was found in the MR-Egger regression and MR-PRESSO Global test (Figures 2–5).
Discussion
To the best of our knowledge, this is the first study to employ Mendelian randomization analysis in investigating a potential causal genetic association between AS and blood pressure. No causal association was found between AS and blood pressure. The two-sample Mendelian randomization results suggested no causal genetic association between AS and blood pressure, and this is different with previous observational studies. We also tested the results for heterogeneity and pleiotropy. Therefore, our results were reliable and were conformed to the three assumptions of Mendelian randomization.
We found that there is no causal association between AS and hypertension, and that MR results between AS and diastolic blood pressure and systolic blood pressure were negative. This means that AS does not have an effect on blood pressure. For the integrity of the study, we conduct a reverse Mendelian randomization between blood pressure and AS. No causal association was found in hypertension and its secondary subtypes. The evidence presented indicates that AS is not influenced by fluctuations in blood pressure. The MR results using another validation cohort is negative. All these make our conclusions more complete and rigorous.
Previous studies on the association between AS and blood pressure remain controversial. However, it is worth noting that increased blood pressure is accompanied by arterial plaque formation, vascular intima thickening and obesity, and other metabolic problems.23,24 Resorlu et al. 25 found that carotid intima-media thickness was 0.76 ± 0.19 in the AS and 0.57 ± 0.12 mm in the control (p < 0.05), and epicardial adipose tissue thickness was 4.35 ± 1.56 in the AS and 3.03 ± 0.94 mm in the control (p < 0.05), respectively. The level of triglyceride and blood pressure were correlated with the Bath AS Functional Index. 25 The blood pressure may be affected by confounding factors, whether there is a genetic causal association still need to be further studied.
As our results suggest, there is no causal genetic association between AS and hypertension. But the results do not account for nongenetic influences, such as environmental exposures or lifestyle factors. They may interact with each other through intermediate factors. Nonsteroidal anti-inflammatory drugs (NSAIDs) are recommended as first-line medications in the treatment of AS. 26 However, clinical studies shown that NSAIDs can increase blood pressure in people with normal blood pressure. 27 Continuous NSAID use in AS patients was associated with an approximately 12% increased risk for hypertension during the follow-up. 28 According to these studies, it is more likely that the changes in habits and the side effects during the drug treatment caused the fluctuation of blood pressure. Al of these are environmental factors and do not come from genetic factors.
AS can lead to internal environment disturbance. Related studies reported that total cholesterol, low-density lipoprotein and uric acid in AS were significantly higher than control. 29 However, all these factors may contribute to the increase of cardiovascular risk. Some studies have also shown that body fat content is significantly increased in AS.30,31 Patients with AS have a higher prevalence of obstructive sleep apnoea than in control. 32 All of the above factors may act as confounding factors which may lead to the change of blood pressure.
Many studies have conducted Mendelian randomization analyses on the correlation between cardiovascular risk and AS. Peng et al. 33 demonstrated an increased risk of heart failure in individuals with AS (OR: 1.0132, 95% CI: 1.0043–1.0221, p = 0.003). The MR analysis results did not demonstrate a causal relationship between AS and other cardiovascular diseases, such as atrial fibrillation, coronary artery disease, ischemic stroke, myocardial infarction, and valvular heart disease (all p > 0.05). Lu et al. 34 found that AS was associated with a high risk of heart failure and ischemic stroke, while negatively genetic susceptibility was found between AS and peripheral atherosclerosis. Based on the conclusion of this study, although AS has no impact on blood pressure, it indeed leads to an increase in cardiovascular risk.
Our study also has limitations. First, the GWAS database is always updated and conclusions may be updated as more research results obtained. Second, all the hypertension cases included were patients with self-measured high blood pressure, and the categories of hypertension and the basic information of the patients were not deeply studied. Furthermore, all the enrolled patients were European, and the results may not be generalizable to Asians due to racial differences. Given the significant difference in variants identified by the Finnish GWAS study, there may be the genetic risk profile of this group matches that of the remaining European population.
Conclusion
This study represents the first two-sample Mendelian randomization analysis aimed at investigating the causal genetic relationship between AS and blood pressure. Our Mendelian randomization analysis results revealed a lack of causal association between AS and hypertension, diastolic blood pressure, as well as systolic blood pressure.
Footnotes
Ethical considerations
Ethical approval was not sought for this study because *REASON*. All the data in this article can be found in online repositories. The GWAS studies had previously gained ethical approval, and the present analysis was based on publicly available data, which did not need additional approval of the ethics committee.
Consent to participate
Informed consent was not sought for the present study because the original research participants provided written informed consent.
Author contributions
Weiran Hu and Kai Zhang: analysis of data, drafting and revising manuscript, and final approval. Guang Yang: design, acquisition, analysis of data, drafting and revising manuscript, and final approval. Haoxu Wang: data collection and final approval. Yanzheng Gao: conception and design of work, drafting and revising manuscript, and final approval
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Research Program of Henan Province (242102310107) and the Medical Science and Technology Research Program of Henan Province (LHGJ20240006).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All of the data are described in the manuscript. Data available on request from the authors.