
Abstract
Introduction and Objective:
In recent decades, caesarean section rates have increased dramatically worldwide and the reasons for this trend are not fully understood. This continuing trend has raised public health concerns regarding higher maternal and perinatal risks, high costs, healthcare efficiency, and inequality of services. The current study aimed to explore the perspectives and insights of healthcare providers and policymakers in the Israeli health system regarding the factors that drive caesarean section rates and the readiness and feasibility of implementing the Robson Ten Group Classification System for the first time.
Methods:
Semi-structured interviews were conducted (n = 12) with purposefully selected healthcare providers and policymakers in Israel. Data was analysed inductively using a thematic analysis approach.
Results:
The findings reflected the “changing landscape” in childbirth practices and attitudes that contributes to the rising caesarean section rate, including childbirth at older ages, birth planning, and a transition toward a more collaborative decision-making approach to childbirth. The participants emphasized the lack of a standardized classification or consistent data monitoring of caesarean section in the Israeli health system. Additionally, enablers to implement the Robson Ten Group Classification System in Israel (ease of use, data collection and recording, and the allocation of resources and personnel), as well as barriers (concerns over workload, limited resources, budget implications, and technological complexity), were found.
Conclusions:
This study revealed the multifaceted factors shaping caesarean section rates within Israel and underscored the perceived need for evidence-based monitoring and informed decision-making in healthcare practices. Our findings support the conclusion that empirical evidence and clear data are crucial for effective caesarean section use and are currently lacking in Israeli hospitals. Thus, it is recommended to adopt a globally standardized, accepted, and effective tool—the Robson Ten Group Classification System—to accommodate the “changing landscape” in alignment with evolving medical and societal dynamics, which consequently will assist in optimizing caesarean section use.
Introduction
Caesarean section (CS) serves as a vital and life-saving procedure in reducing maternal and neonatal morbidity and is one of the best maternal health services quality indicators. Despite its proven advantages, CS can lead to increased medical risks for both mothers and newborns, especially when performed without a medical indication.1–3
Thus, compared to vaginal births (VB), CS delivery is associated with various short- and long-term adverse maternal outcomes, such as a greater risk of postpartum mortality, infection, hemorrhage, anesthesia-related complications, adhesions, lacerations, extended recovery time, and risk of additional surgeries.4–6 There may be negative emotional and psycho-social outcomes regarding the mother–baby relationship, a higher risk of postpartum depression, and unsuccessful breastfeeding.7–9 In addition, the hormonal, physical, and bacterial exposures of newborns delivered by CS are different from those delivered by VB, which can lead to changes in physiology, a higher risk of developing allergies, breathing problems, a low Apgar score, childhood onset of type 1 diabetes, and even obesity in adulthood.2,8 Furthermore, increased rates of CS are associated with significantly higher costs than VB thus imposing an economic burden on the healthcare system, resulting from extended hospital stays, an increased probability of re-hospitalization, and more.5,8,10,11
Ideally, according to a statement by the World Health Organization (WHO) in 1985, 12 the CS rate should not be higher than 15% of all deliveries, excluding stillbirths. A more recent WHO statement in 2015 has advised that at the population level, CS rates higher than 10% from all live births are not associated with reductions in maternal and newborn mortality rates 13 ; a statement supported by recent data.14–16 Nevertheless, CS should be provided based on necessity, rather than aiming to achieve a specific rate. 17
In recent decades, CS has become more prevalent in developed and developing countries without a clear understanding of the main reasons and motivations. Available data (2010–2018) from 154 countries, covering 94.5% of worldwide live births, show that the global average CS rate is 21.1%. This rate has been rising in high-, middle-, and low-income countries by an average of 4% per year since 1990. Estimates indicate that by 2030, 28.5% of women worldwide will have given birth by CS.11,18–23
Israel is not exempt from this trend. According to the Israeli Ministry of Health, 24 the rate of CS has increased by 80% since 1999, and approximately one in five women giving birth in Israel undergo CS.6,25,26 Additionally, about 6000 CS procedures are performed in Israel each year without a medical indication, resulting in an excess of approximately 3.6 million dollars in healthcare costs (based only on the marginal resources directly associated with the CS procedure). 27
One of the main goals of WHO 2030 is to reduce maternal and newborn mortality and morbidity by ensuring the safety of the mother and baby during delivery and avoiding unnecessary CS. 14 In light of the potential risks associated with an increased CS rate, the economic burden, and the inequity in accessibility, since CS is an important indicator of maternal health services access and quality, optimizing CS use is currently a global health priority.5,11,21,28–30
Since 2015, WHO has recommended the adoption and application of the Robson Classification System, also known as the Robson Ten Group Classification System (RTGCS), as the most valid method to meet current local and international perinatal and CS monitoring needs.13,31–33 The RTGCS was also recommended by the International Federation of Gynecology and Obstetrics, and the European Board and College of Obstetrics and Gynecology (EBCOG).28,33,34
RTGCS classifies all women admitted for delivery into 1 of 10 groups that are mutually exclusive and totally inclusive, based on a set of predefined obstetric indicators: parity and previous CS, onset of labor, fetal presentation, number of fetuses, and gestational age. These easy and simple indicators are routinely collected during hospital admission for delivery.2,35,36 The RTGCS serves as an overall prospective structure for characterizing, evaluating, monitoring, and comparing CS rates within and between hospitals, in a standard, reliable, and indication-based way.23,37 Implementation of the system is associated with optimized CS use and reduced rates.38–41 Although the RTGCS is widely considered an applicable system,29,37 Israel has not yet implemented it and currently lacks an accepted method for characterizing and monitoring Israeli CS rates; a situation that reflects another importance of the present study.
We explored the perspectives and insights of healthcare providers and policymakers in the Israeli health system regarding the factors that drive CS rates and the level of readiness and feasibility of implementing a new classification system. Since healthcare providers and policymakers greatly influence systemic and effective processes, ascertaining their perceptions is a fundamental and initial step toward optimizing CS use through implementing the RTGCS in Israel for the first time.
Method
Qualitative methodology research was chosen to understand a critical issue on the public health agenda, namely, the rising rate of CS performed. This research method is gaining importance and recognition in health and healthcare, particularly when exploring key areas of uncertainty.42,43 Hence, this approach is appropriate for the study’s goals and topic.
To better understand healthcare providers’ and policymakers’ perspectives regarding the driving factors of CS rates and the feasibility of implementing the RTGCS in Israel, semi-structured in-depth interviews were conducted. Semi-structured interviews are one of the most common qualitative data collection methods, combining predetermined questions with open and flexible ad hoc questions initiated by the interviewer, thereby allowing interviewees to provide more detailed information based on their initial answers. The dynamic nature of semi-structured interviews enables revealing information about situations that cannot be observed directly. 44 This research tool is also defined as a “monologue on the research topic” due to the opportunity afforded to interviewees to express their thoughts and the development of the interview beyond the existing format of structured survey questions.45,46
Participants and sampling
The sampling methods were purposive, characterized by a focused effort to achieve variance among interviewees. 47 The interviews based on this sampling method are also called key informant interviews, meaning that the participants were experts chosen based on their comprehensive and in-depth knowledge due to their role or ability to translate and interpret the topic. 48 The final sample size was determined according to the “theoretical saturation” principle. 49
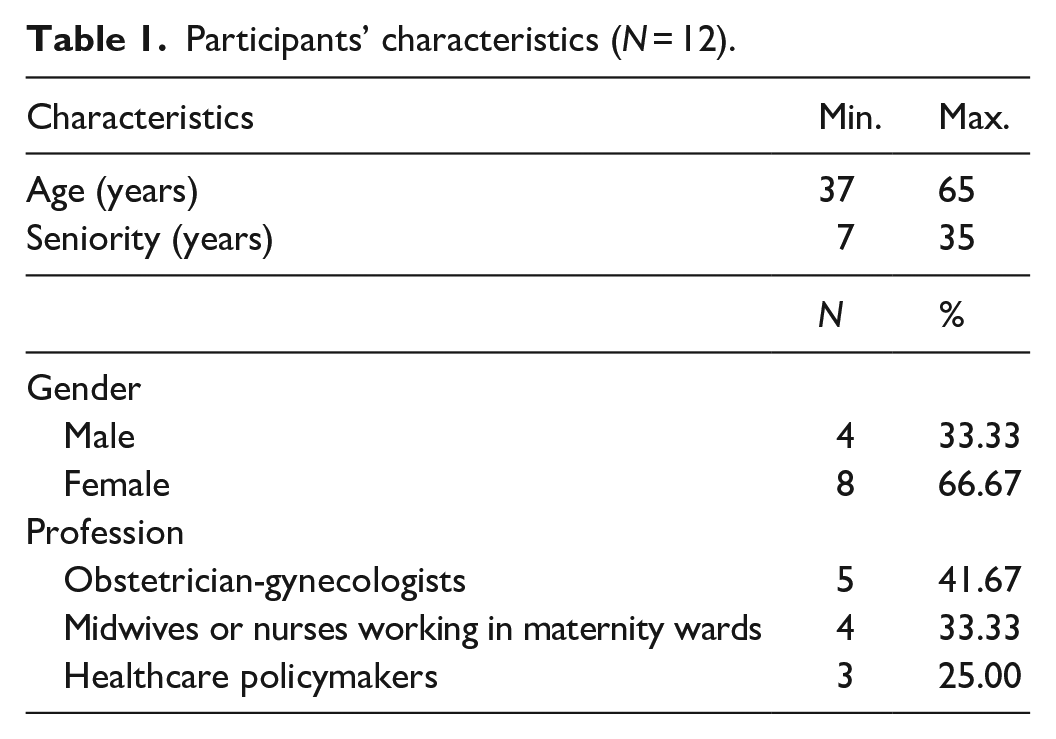
Initial contact with 16 potential participants was by phone or email and included a detailed explanation of the study. Four candidates declined for lack of time. Therefore, 12 interviews were conducted with a heterogeneous group of health professionals, including 5 obstetrician-gynecologists (4 who were also heads of a maternal-fetal medicine department, obstetrics department, or maternity ward), 4 midwives or nurses working in maternity wards, and 3 healthcare policymakers (who were also physicians). The participants were aged 37–65, and their seniority ranged from 7 to 35 years. Most were females (8). The sociodemographic characteristics of the study participants are described in Table 1.
Participants’ characteristics (N = 12).
Procedure
The interview guide was developed based on a literature review,50,51 and consultation with an expert panel in the researchers’ fields of specialization: public health, health promotion, obstetrics, and gynecology. As much as possible, the questions asked were broad and open-ended to allow the interviewees to express their subjective meaning attributed to the phenomenon being studied, following the inductive principle. For example: “To the best of your knowledge, what is the Ministry of Health’s position on CSs?”; “Based on your familiarity with the Israeli healthcare system, what are the factors that may promote the implementation of the Robson Classification System in Israel?”. The interview guide was revised by three experts from the field of specialization (public health, healthcare, health promotion, obstetrics, and gynecology), based on recommendations of the Consolidated Criteria for Reporting Qualitative Research (COREQ) for qualitative studies. 51 Furthermore, the interview guide was pilot-tested; Four preliminary interviews were conducted with midwives who were also students in health systems management to identify unclear or ambiguous wording. These interviews were excluded from the data analysis.
The interviews were conducted in Hebrew by the researchers. Since the TGCS has never been implemented in Israel, all researchers (PhD’s, and a PhD candidate) thoroughly studied the TGCS and the WHO Implementation Guide. The interviews were held between May and July 2023, partly face-to-face and partly through Zoom software at a time convenient for the interviewee. Interviews lasted between 30 and 45 min and were recorded and transcribed.
Data analysis and trustworthiness
The interviews were analyzed using the thematic coding method according to Braun and Clarke’s six analysis stages. 52 This approach involves systematic data immersion, initial code generation, and subsequent identification of themes by clustering-related codes. These themes are carefully reviewed, defined, and named to reflect meaningful patterns in the data. The final output is a coherent report that outlines the research process, presents the derived themes, and supports them with pertinent data excerpts. This flexible and iterative process provides a structured yet adaptable method for uncovering significant insights from qualitative data.
Qualitative research traditionally does not purport to produce absolute truths and its quality is measured by being trustworthy. 53 In the present research, the authors adhered to the standards suggested by Korstjens and Moser 54 : credibility, transferability, dependability, confirmability, and reflexivity. This included transparency of the research procedures, accurate transcription, the use of many citations, and database management. To avoid bias, each researcher analyzed the themes separately and then compared them and discussed the gaps, until the final themes were chosen.
Ethics
By nature, an interview is a platform for personal disclosure and developing a trusting relationship with the interviewees. Hence, the researchers made an effort to adhere to accepted ethical principles and to protect participants’ anonymity and confidentiality by avoiding identifying details and using pseudonyms. All participants provided verbal informed consent prior to enrolment in the study. It was emphasized to them that they could stop their participation at any given moment as well as skip questions. The transcripts were kept private and protected by a password. Our study was approved by Ariel University’s Ethics Committee (approval no. AU-HEA-LK-2023111).
Results
Continuously with the purpose of the study, exploring the perspectives and insights regarding the factors that drive CS rates and the level of readiness and feasibility of implementing a new classification system, three interrelated themes that emerged from the thematic analysis process are presented: Motives for the increase in CS rate, Monitoring the CS rate in Israel and Readiness to implement the RTGCS. A meticulous consideration was given to the identification and selection of themes, based on their prominence and relevance to the research objective.
Motives for the increase in CS rate: A changing landscape?
The first theme focuses on the causes and motives underlying the increase in the CS rate, both in a broad sense and particularly within Israel’s context as a high-fertility population. This “changing landscape” theme that characterizes the last decade and has influenced the rising CS rate includes several key aspects: the mother’s socio-demographic characteristics, the cultural-societal context, and the transition from a medical paternalistic approach to childbirth toward a more collaborative and shared decision-making approach. We propose that these aspects are intertwined, reflecting a mutually influencing and simultaneous process in both the sociocultural and medical domains.
The first aspect of the “changing landscape” is the mother’s socio-demographic characteristics. The interviews presented a contemporary trend wherein women experience childbirth at more advanced ages due to late marriage, acquisition of higher education, and career development. Childbirth at older ages is associated with a higher risk of CS. For example, P1 (gynecologist, head of the birth and maternity ward at a large hospital) stated: This is due to a global trend that, first of all, women now tend to postpone pregnancy because there are more academics, waiting for “prince charming” . . . they are career women. It makes a lot of sense to me. . . This increase is not because of women who suddenly decide they want to give birth through the abdomen.
A similar trend was mentioned in another interview as well: P2 (gynecologist, head of the birth and maternity ward at a large hospital): . . .The western world trend is that everything should be fast and planned, with a minimum of malfunctions—a CS is seen as such.
Thus, this socio-demographic change reflects a current broad cultural-societal context where more women express a desire for a predictable and prearranged birth, scheduled in advance, allowing them to proactively prepare amidst the demands of their active lifestyles.
Another aspect deals with the transition from a traditional medical-paternalistic approach to childbirth toward a more collaborative and shared decision-making approach that puts the mother’s autonomy in the center (alongside the more prominent presence of defensive medicine in this context). The interviews revealed that in recent years a higher rate of pregnant women request a CS without a medical indication. This is leading to a change in CS use, previously performed mostly or solely for medical indications.
P3 (midwife at a large hospital): . . . more women are in a hurry to undergo a CS. The indications for a CS remain the same, but the desire is increasing. I meet more and more women who prefer a CS. . . If you compare it to 10–15 years ago when I started working, you can see a difference. . . Hospitals used to have strict rules regarding CS, but today the woman decides what to do with her body.
The rise in demand for a CS at mothers’ request appears to be a noteworthy shift that must be taken into consideration: P4 (nurse in a former obstetrics and maternity ward and researcher in health sciences): . . .I noticed that suddenly women began asking for CS. . . what should we do about it? “Asking” is not an indication for a CS. . . There are many ethical aspects here that have not been considered. Perhaps progress and technology are ahead of ethical and moral regulation.
It is evident from the interviewees that respect for the value of patient choice is becoming more and more acceptable. There is a gradual transition from the traditional paternalistic approach regarding birth as a medical event controlled by experts toward a more collaborative approach where the woman is the expert and has autonomy over her body. As such, even if there is no medical indication, she can choose to undergo birth by CS.
P5 (physician, holding a senior position in the Ministry of Health): The reason for the increase is the woman’s autonomy. This tends to change paternalistic perceptions. More liberal perceptions of a woman’s right to her body and autonomy have entered. This is a significant change. . . Health providers have also adjusted to social changes more than medical changes and they understand they have to respect the mother’s request.
The role of health providers in the process is to provide information and reflect on the possible risks to allow the mother to make an informed choice.
P6 (midwife at a medium-sized hospital): . . . When a woman gives birth and asks for a CS without a medical indication, I remind her that it involves risks and has consequences. The choice to undergo surgery like this makes me uncomfortable. . . Indeed, we see negative outcomes. I believe this is the main cause of the increase in the CS rate.
It is noteworthy that among interviewees holding policy-making positions, defensive medicine emerged as a significant factor in this context. Namely, a concern regarding potential legal repercussions exists if physicians were to decline a woman’s request for a CS without a medical necessity, especially if any resultant harm were to occur. This concern serves as a driving factor contributing to the rising rates. Physicians practice defensive medicine, find themselves obligated to navigate risks, and in many cases opt for surgery even in the absence of a medical indication.
P7 (physician, holding a senior position in the Ministry of Health): This is a field with a lot of lawsuits, and physicians stressed managing risks. P8 (physician, holding a senior position in the Ministry of Health): In the medical aspect, the highest rate of lawsuits is for CS. The physicians are not neutral for this reason and it influences their decision-making. That is why it is difficult for the Ministry of Health to get down to individual adjustments and provide a clear position on the issue.
Monitoring the CS rate in Israel: Recognizing the need
The second theme highlights the emerging need for monitoring CS rates in Israeli hospitals to optimize utilization of the procedure. Clearly emerging from the interviewees was the lack of an accepted classification system or consistent monitoring method for CS use. No interviewee was exposed to official position papers concerning CS utilization. This reality makes it difficult to understand the current status and to develop data-based interventions.
For example, P9, a gynecologist at a large hospital, expressed concern regarding the lack of relevant data and comparison standards: Currently, I have no relevant data, except how many women last month underwent CS in this hospital. . . They say we are below average, like average, but what does that mean? It’s just a random number. . . Is it acceptable or not? . . . I’m not sure these rates are justified because I have no comparison standard.
Later on, the gynecologist emphasized the need for monitoring to make informed decisions and plan ahead, given the expected increase in the population and the economic burden on the health system: . . . I feel that this is necessary, also because of the expected increase in the population. . . we will have to control resources, and CS is a valuable resource. . . longer hospitalizations, higher risk of re-hospitalization, and a heavy economic burden on the health system. . .
Similarly, P10, a midwife at a medium-sized hospital, supported this idea: . . . as a hospital, we do not have an official and declared discussion about CS. . . I know the rate, but that’s all. Therefore, my answer is yes, we need to promote and optimize the use of CS in Israel.
Even policymakers acknowledge the need for routine CS examination to ensure its justification. P2, a gynecologist and head of the birth and maternity ward at a large hospital, admitted: We don’t routinely examine whether every CS is justified. There have been attempts in the past, but unfortunately, they have been unsuccessful.
Thus, a conclusion is that for effective CS use, there is a fundamental need for empirical evidence and clear data, which is currently lacking in Israeli hospitals.
P7 (physician, holding a senior position in the Ministry of Health): If there is overuse to consider, we need clear evidence. . . Only then can a discussion be sparked and action taken to improve. Until we have clear data, how can we harness professionals to the issue and develop interventions?
Readiness to implement the RTGCS: Enablers and barriers
Interviewees were asked if they were familiar with the RTGCS. Except for one interviewee, none had heard previously of the system. Therefore, during the interview, the interviewers described the RTGCS, its method, and its goals. Then, they asked about possible factors that might promote or hinder the system implementation in Israeli hospitals.
As CS use in Israel is changing and monitoring it is essential, the third theme addresses enablers and barriers relating to the first implementation of the RTGCS in the Israeli health system. It is evident that these factors reflect the interviewees’ perceived advantages and disadvantages of this system.
Enablers include ease of use, ease of data collection and recording, and the allocation of resources and personnel. Healthcare providers’ familiarity with the system and its contribution is another enabler. Several interviewees suggested holding a formal presentation on the system for staff and appointing a leading professional to manage the initial implementation. Interestingly, another promoting factor suggested by some of the interviewees holding senior positions is implementing the RTGCS as a quality measure. For example, P11 (a gynecologist and former head of the maternity ward in a large hospital) stated: I recommend obtaining exclusive funding from the Ministry of Health to implement the system and fund participating hospitals. It is also possible to compare with an audit department. The hospitals can say: “We use validated criteria and indicators” with pride. The Ministry of Health will credit this method for its effectiveness.
Barriers to implementation include: concerns regarding manual data collection or using a new and complex technological system that delays work procedures or adds to the existing workload; limited personnel resources; concerns regarding the system’s impact on the hospital’s budget for CS; and lack of familiarity with the system.
P12, a gynecologist, and head of a large hospital’s maternity ward, summarized the theme: I will address both questions together because they are oxymoronic. First, if this system is easy, accessible, and simple to use, we do not have to log in to a special program and enter a username and a password. . . That is, a minimum of effort will be required from the medical staff in terms of computing and technology. . . Second, we must benefit from the system; the system will demonstrate efficiency and help in work processes. . . In the opposite situation, if the system is not easy, accessible, or simple for medical staff, this is the number one factor that will delay its implementation.
Table 2 below summarizes the enablers and barriers that reflect the degree of readiness to implement the RTGCS from healthcare providers’ and policymakers’ perspectives:
Enablers and barriers.

Discussion
A primary goal of maternity care is to provide safe outcomes for mothers and newborns during childbirth. The worldwide CS rate has increased dramatically in recent decades and the reasons for this trend are not fully understood. The continuing rise in CS rates is a public health concern due to higher maternal and perinatal risks, high costs, the need for healthcare efficiency, and inequality of access to services.11,19–23,55 This study aimed to examine the viewpoints of healthcare providers and policymakers within the Israeli health system concerning the determinants influencing CS rates, as well as assess the preparedness and feasibility of implementing the RTGCS. This study was based on the assumption that involving healthcare professionals is essential to promoting systemic and effective processes. Thus, understanding their perceptions is a fundamental and initial step toward optimizing CS use in Israel. Moreover, those viewpoints are particularly relevant to policy and practice decisions since qualitative research often describes the setting in which policies will be applied. 56
In examining the motives behind the increase in CS rates, our study uncovered a dynamic “changing landscape” in childbirth practices and attitudes. It underscores the multifaceted influences contributing to the rise in CS rates, including the changing socio-demographic characteristics of mothers and the cultural-societal context. Additionally, a significant factor that emerged is a transition from a traditional medical-paternalistic approach to a more collaborative decision-making model that empowers mothers’ autonomy in childbirth choices alongside increased maternal requests for a CS delivery without strict medical necessity. This shift during the years in Israel regarding the concept of providing a customer-oriented medical service highlights that ethical and societal considerations are intertwined with medical decisions.
These findings outline that Israel’s motives are similar to findings in other countries. Several studies mentioned motives such as the socio-demographic characteristics of the mother and/or a change in healthcare providers’ attitudes and perceptions toward the woman’s right to choose her delivery mode,55,57,58 as major contributors to the increasing prevalence of CS. The extensive research literature has also shown an increase in CS by maternal request.59–61
Notably, our study found that defensive medicine plays a role in increasing CS rates. According to Panda et al., 55 physicians’ “perceived fear” of legal implications due to clinicians’ past experiences, societal attitudes, and the media, influences decision-making and contributes to rising CS rates. Minkoff 62 stated that it is still unclear whether fear of litigation contributes to, or even drives, rising CS rates. The participants in our study explicitly expressed how this factor is taken into consideration during decision-making processes and may affect CS use.
Our findings imply that the abovementioned aspects are interconnected, both in the socio-cultural domain and the medical domain, reflecting simultaneous changes in society’s perceptions and medical practices related to childbirth. The changing landscape represents a perception of orientation toward the client’s wishes and encompasses these trends thereby shaping the increase in CS rates. As society’s perception of childbirth changes, healthcare providers adapt, respecting patient autonomy while emphasizing informed decision-making. This evolving landscape presents both challenges and opportunities for healthcare systems.
Another key finding in this study sheds light on the necessity for monitoring CS rates in Israel and emphasizes the lack of standardized classification or consistent data monitoring methods in Israeli hospitals. This void poses a challenge to understanding the current status of CS use and to developing data-based interventions. It seems that policymakers and healthcare professionals recognize the need for routine CS rate examination to ensure its justification, optimize its utilization, and make informed decisions and plans, given the expected increase in Israel’s population and the potential economic burden on the health system.
The research literature shows that monitoring maternal health practices, including CS use, is essential to assess progress toward health goals.35,36,63 It also provides a platform for data-based discussions; a CS rate is considered appropriate and optimal only if data is available to explain and justify it. 21 Furthermore, other systemic factors with significant influence may be considered when evaluating and interpreting these rates and results. For example, health system factors (models of care, payment systems for health care providers and facilities, staffing or resource availability), or clinical processes may vary between maternity units (diagnosis of labor, fetal distress, electronic fetal monitoring, or indications for CS).35,63
Participants in this study had shown support for the importance of empirical evidence and clear data as crucial for effective CS use and that these are currently lacking in Israeli hospitals. Therefore, the implementation of an acceptable and effective system is needed to address this issue. In this context, we argue that the collection of high-quality routine data and its classification for improving healthcare quality should be a priority on policymakers’ lists to enable data-based decision-making regarding desirable CS strategies. As stated by Robson et al., 36 “It is the professionals’ responsibility to practice evidence-based medicine, but they should also collect the evidence to ensure their patients receive high-quality care.”
Additionally, as CS use in Israel is changing and its monitoring is essential, the current study revealed enablers and barriers to the first implementation of the RTGCS in Israel. Despite limited initial familiarity, healthcare professionals recognized the system’s potential benefits, including user-friendliness, ease of data collection, and potential quality improvement. Conversely, barriers, such as concerns over workload, limited resources, budget implications, and technological complexity, were perceived by our participants as potentially hindering successful implementation.
Empirical evidence shows that the RTGCS easily can be adapted for local use. The size and CS rate of each of the 10 groups can provide useful information about care quality in a particular region or setting and can be used to compare interventions’ impact. Therefore, the RTGCS data, as based on a perinatal classification system, can provide valuable insight regarding not only the CS rate but also obstetric populations and outcomes.37–41,64 Hence, this effective system has the potential to improve obstetric practices in Israel; for the first time, it will be possible to compare and characterize Israeli CS rates and usage patterns, and so the great importance of its implementation in health services. The RTGCS provides an initial structure for analyzing additional epidemiological variables, processes, and perinatal outcomes as well as CS. In this context, The TGCS may serve as a promising starting point. 65
Despite its importance, this research is not without limitations. This study used purposive sampling, a non-probability sampling technique that researchers use to select subjects or units from a population. Non-probability sampling, however, has limitations due to the subjective nature of participant selection and thus the sample may not be representative of the general population of policymakers and health professionals in the health systems. 66 It is recommended that a further examination be conducted among a wider and more representative sample. In addition, most interviewees had no prior knowledge of the RTGCS and this may have influenced their responses. In this regard, it is advisable to explore the enablers and barriers of the RTGCS after the first implementation to improve and adjust the system’s use and adapt to both the Israeli culture and the computerized medical information system used in Israel. Finally, considering the findings, it is advisable to examine the relationship between fear of litigation and CS use in a quantitative follow-up study to improve understanding of these variables.
Conclusion
In conclusion, the present innovative and exploratory study revealed for the first time the perceptions of healthcare providers and policymakers in the Israeli health system regarding CS usage and rates and proposes the implementation of an international classification system that has not been applied yet in Israel. Overall, this study demonstrates the multifaceted factors shaping CS rates within Israel and also underscores the broader perceived need for evidence-based monitoring and informed decision-making in healthcare practices. It indicates the significance of adopting a globally standardized, accepted, and effective tool—the RTGCS—as a prenatal and CS classification system, to align with changing landscapes and evolving medical and societal dynamics. Consequently and hopefully, it will assist in optimizing labor and delivery, including CS use, in Israel.
Furthermore, data collection and interpretation are central elements in medical treatment and decision-making. We suggest that rather than goal-oriented data collection, a contemporary and more up-to-date research paradigm can be used based on big data collection through RTGCS implementation and analysis with advanced tools. Thereby, perhaps new insights can be reached on CS use for quality improvement and benchmarking.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241237447 – Supplemental material for Optimizing caesarean section use and feasibility of implementing the Robson classification system: Perspectives of healthcare providers and policymakers
Supplemental material, sj-docx-1-smo-10.1177_20503121241237447 for Optimizing caesarean section use and feasibility of implementing the Robson classification system: Perspectives of healthcare providers and policymakers by Noa Shtainmetz, Riki Tesler, Cochava Sharon and Liat Korn in SAGE Open Medicine
Footnotes
Acknowledgements
We thank all our participants for their time and insights.
Author contributions
Conceptualization: N.S., R.T., C.S., L.K.; Methodology: N.S., R.T., L.K.; Analysis, N.S., R.T., L.K.; Writing: N.S.; Supervision: N.S., R.T., L.K.; Project administration: N.S., C.S.
Data availability statement
Data can be made available from the corresponding author upon request for non-commercial purposes.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our study was approved by Ariel University’s Ethics Committee (approval no. AU-HEA-LK-2023111).
Consent for publication
All authors gave consent for publication.
Informed consent
All participants gave verbal informed consent prior to enrolment in the study. The Ethics Committee of Ariel University did not condition the conduct of the interviews by actively signing written informed consent.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.