
Abstract
Objectives:
This qualitative study aims to examine the enablers and barriers to portable ultrasound device utilization for antenatal care in rural Philippine health centers, with the goal of improving maternal outcomes and reducing maternal mortality.
Methods:
We conducted focus group discussions with 18 healthcare workers (midwives, a nurse, and a radiologic technician) and 20 pregnant women across 5 rural health centers. We used inductive thematic analysis to identify system-related, provider-related, and client-related enablers and barriers.
Results:
Enablers included free ultrasound services, hospital policies requiring prenatal scans, provider training, awareness creation, patient interest and acceptance, and confidence in HCWs’ capabilities. Barriers comprised resource limitations, distance to facilities, insufficient HCW skills, time constraints, emotional fears, traditional beliefs, misconceptions, and lack of trust in providers’ competence.
Conclusion:
Addressing resource gaps, ongoing provider training, and patient education may enhance portable ultrasound device uptake and significantly improve maternal health outcomes in low-resource settings.
Keywords
Introduction
Routine transabdominal ultrasound imaging is commonly performed during pregnancy because it can guide antenatal care. A basic obstetric ultrasound examination can provide information regarding cardiac activity, placental localization, fetal presentation, gestational age, fetal number, fetal anatomy, fetal biometry, amniotic fluid volume, and maternal anatomy. 1 It is generally considered safer than other imaging techniques because it relies on sound waves rather than ionizing radiation.
However, basic antenatal care in many rural Philippine health centers typically includes only fundamental services (e.g., blood pressure checks, abdominal palpation, and standard laboratory tests). Ultrasound scanning may not be part of routine care if resources or trained staff are lacking. Although the Philippines has national guidelines recommending at least four antenatal visits and two scans (first and mid-trimester), 2 implementation in remote areas varies widely. Consequently, the Philippines also has one of the highest maternal mortality rates in Southeast Asia. 2 According to the latest data from the Philippine Statistics Authority, there were 1219 maternal deaths in 2019, translating to a maternal mortality ratio of 121 per 100,000 live births, with rural areas disproportionately affected. 2
Rural health centers in the Philippines are not uniform. Some function as lying-in clinics or birthing facilities, while others refer high-risk cases to higher-level hospitals; many lack advanced diagnostic tools like ultrasound machines.3,4 This heterogeneity underscores the need for targeted approaches to improve antenatal care.
Extensive literature has linked ultrasound usage in antenatal screening with better maternal outcomes.5,6 Updated WHO guidelines also emphasize early ultrasound for a positive pregnancy experience. Previous research indicates that general practitioners, nurses, and midwives can be trained to operate portable ultrasound devices (PUDs) effectively.7,8 In the past year, several PUDs were donated to select rural health centers in Casiguran, Aurora; Tondo, Manila; Binondo, Manila; and Bantayan Island, Cebu. 9 Operating these devices helps detect high-risk pregnancies (e.g., fetal malpresentation, low-lying placentas, multiple gestations) for referral to higher-level facilities.7,10
According to pilot programs such as iBuntis®, 7 equipping rural health centers with PUDs helps healthcare workers (HCWs) better screen and manage high-risk pregnancies. Nevertheless, the gap remains in understanding how these devices integrate into basic antenatal services under varied resource constraints, and which factors facilitate or hinder their usage. Therefore, this article aims to determine the enablers and barriers to PUD utilization for antenatal care in rural Philippine health centers, shedding light on potential pathways to enhance maternal care.
Methods
Rural health centers in Lucban (Quezon), Tagkawayan (Quezon), Tondo (Manila), Binondo (Manila), and Bantayan Island (Cebu)—all equipped with PUDs—served as our primary sites. 2 We chose these centers due to recent PUD donations, geographic diversity (coastal, island, and urban-poor), and local official support. Although each center had a medical doctor, the majority of antenatal care and PUD operations fell to midwives and nurses.
Please note: “Barangay” is the smallest administrative division in the Philippines, similar to a village or district. “Kimbo” refers to the name of a Barangay Health Center.
We used a descriptive qualitative approach and conducted focus group discussions (FGDs) in five rural health centers across Quezon, Cebu, and Manila. Eighteen HCWs (16 midwives, 1 nurse, 1 radiologic technician) and 20 pregnant women participated. Both HCWs and patients were recruited through purposive sampling to include those with direct experience in PUD-based antenatal care. Basic socio-demographic characteristics (e.g., approximate age range and years of experience for HCWs) were also recorded to contextualize participants.
HCWs and patients (pregnant women) who were directly involved in the provision of antenatal care using PUDs were included in this study; those who did not consent were excluded. The interviews were conducted in the local language (Tagalog and Cebuano), transcribed, and translated into English for analysis.
All FGDs were conducted and facilitated by two female physicians who were employed as medical school faculty at the time of the study. They had formal training in qualitative research methods, having completed multiple workshops on FGDs and thematic analysis. They had no prior personal relationship with any participants before data collection. Participants were informed that the study aimed to understand enablers and barriers to PUD use for antenatal care, and the facilitators were introduced as neutral researchers without direct clinical authority at their facilities.
Ethical approval for this study was obtained from the Ateneo de Manila University Institutional Review Board (Ref #ASMPH_01_2019). All participants provided written informed consent, and confidentiality and anonymity were maintained throughout the study.
FGDs were conducted separately among HCWs and patients to encourage open discussion. Each FGD included about 5–10 participants, was moderated by one of two physician researchers, and followed a semi-structured interview guide with open-ended questions (e.g., “What factors encourage or hinder you from using the PUD?”). This guide was pilot-tested with about 5% of the total participants (e.g., one nurse, one midwife, and two pregnant women) to ensure clarity. It has not undergone formal validation in other studies, so we note this as a minor limitation in the Discussion. Audio recordings were made of each session, and field notes were taken immediately afterward to capture nonverbal observations and contextual details. Each FGD lasted approximately 45–60 min.
Participants did not receive transcripts for further comment or correction due to time constraints. No repeat interviews were carried out. Data saturation was reached by the fifth FGD when no new themes emerged.
Data were analyzed using inductive thematic analysis. Two researchers independently coded the transcripts line by line using a word processor (no specialized software). They then met for peer debriefings to resolve coding discrepancies and refine subthemes. A preliminary coding tree was developed based on emerging patterns, and final themes (system-related, provider-related, and client-related factors) were agreed upon through consensus with the broader team.
No participant feedback (i.e., transcript/member checking) on final themes was performed. However, verbatim quotes were selected to illustrate key points and ensure data–findings consistency.
The dataset used for this study is available through the Dryad Repository with DOI http://datadryad.org/stash/share/jxUtTgDKNe_XaYklKLbWmig1Zszss9aZP5sg0XDVM9c.
Results
An inductive thematic analysis was used to analyze the FGDs. Three major themes were developed: system-related factors, provider-related factors, and client-related factors (Figure 1).
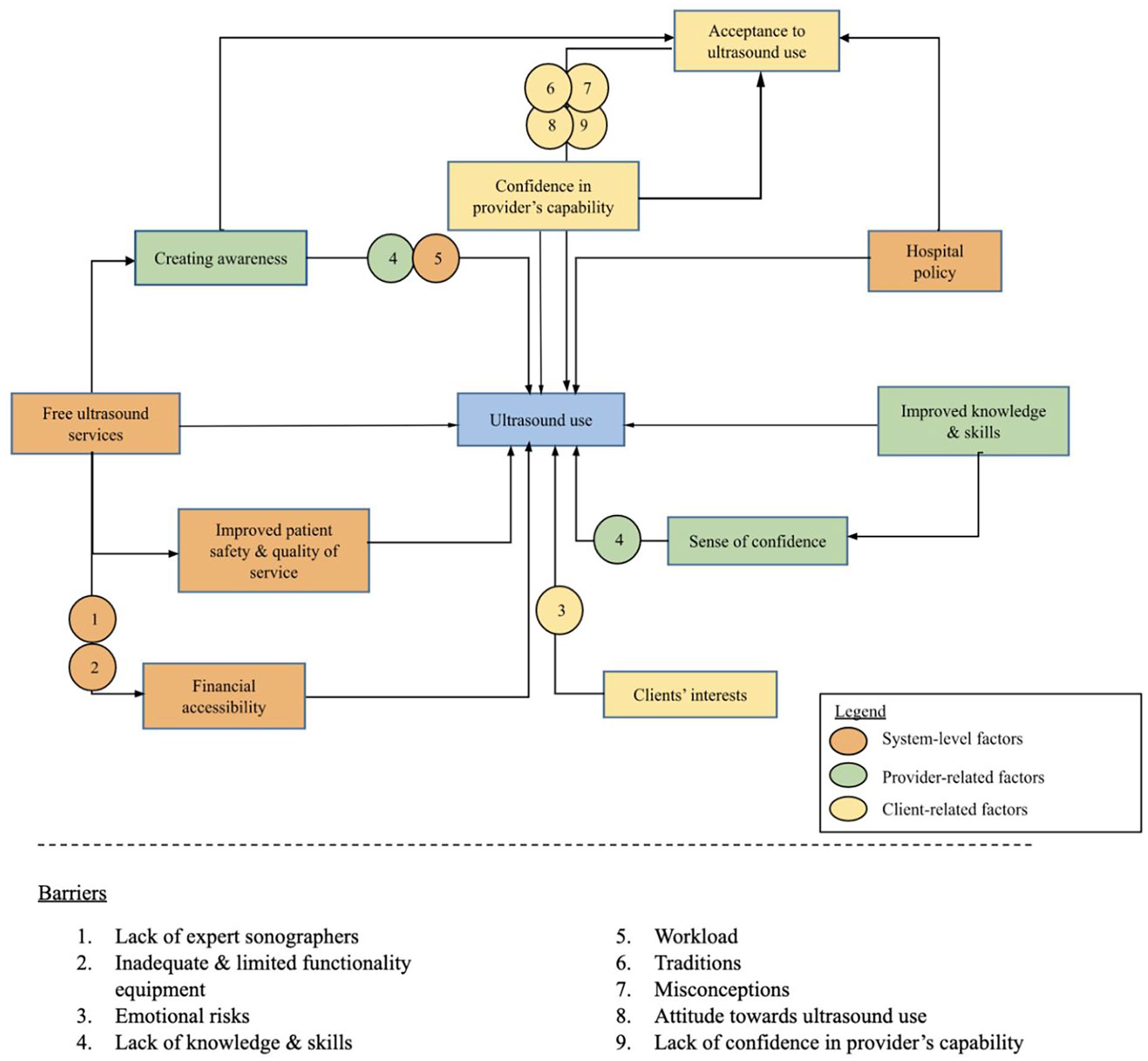
Enablers of and barriers to ultrasound use in rural health centers in the Philippines 1. Lack of expert sonographers, 2. Inadequate equipment, 3. Emotional risks, 4. Lack of capabilities, 5. Workload, 6. Traditions and beliefs, 7. Misconceptions, 8. Attitudes toward ultrasound use, 9. Lack of confidence in provider capabilities.
Figure 1 provides a visual overview of how various system-level, provider-level, and client-level factors collectively influence ultrasound use in rural Philippine health centers. The central box, labeled “Ultrasound use,” is linked to key enablers (e.g., free ultrasound services, improved knowledge and skills, hospital policy, confidence in providers, and client interest), while the barriers—such as lack of expert sonographers, inadequate equipment, emotional risks, misconceptions, and workload—are listed below. The figure highlights how these multi-level factors interact to affect whether and how pregnant women access and benefit from ultrasound services in resource-limited settings.
Enablers of ultrasound use
System-related enablers
Availability of free ultrasound services
HCWs were more likely to promote, use, and provide ultrasound services if a device was available in their center. Having readily available ultrasound devices also supported evidence-based decision-making among the HCWs. This improved overall patient safety and quality of care.
While ultrasound services are also available in private clinics in the area, the 400–1000 Philippine Pesos (PHP) fee in these clinics was prohibitive for most patients. The knowledge that their rural health center provided free ultrasound services encouraged patients to seek ultrasound services there.
It makes me more excited to ask patients to do their prenatal checkups here in San Nicolas Health Center. That’s one of the reasons to encourage patients. – Midwife
The availability of ultrasound equipment encouraged HCW providers to conduct assessments that provided information to support evidence-based decision-making and improved patient safety and quality of care. Participants indicated that ultrasound machines made it possible to assess the health condition of the mother and child, including the location of the placenta, the heartbeat, and the baby’s position. If any complications were detected—for instance, if the baby was in a breech position—the client was referred to the appropriate healthcare facility.
Knowing this means we will not experience emergency cases during delivery because we, and the patient as well, will be aware about their condition, and we can refer them immediately to the nearest hospital due to complications of pregnancy. – Midwife
Hospital policy
Local government mandates require ultrasounds to be performed at regular intervals during pregnancy.
11
Patients are typically advised to acquire an ultrasound scan during their first consultation.
It is a requirement. It is being asked for in the hospital, so we must follow the instructions. - Patient Most of the time, for the patient’s first visit, they are required to get an ultrasound. Most of the time, that’s the first thing the doctor asks for on their first visit. – Midwife
Provider-related enablers
Improved knowledge and skills
Proper training increased operator confidence among providers. Prior to training, a radiologist technician reported that he “was always scared whenever a pregnant patient was referred to [him].” He would choose to refer these patients to other health centers or specialists. However, the workshop “broadened his knowledge, enhanced his skills, and boosted his confidence to operate an ultrasound alone.”
A supportive learning environment also contributed to better knowledge and skills transfer. Following training, the HCWs were thankful that they could “recognize [their] mistakes.” However, it is important to note that confidence levels tended to vary wildly. While confidence was generally higher after their training, some HCWs claimed that they “still had doubts.” This suggested that the proficient use of an ultrasound machine develops with time and experience. There may be a role for continuous training, frequent practice, and supportive supervision.
Creating awareness
Patients were more likely to acquire ultrasound scans when they were actively informed about the availability of free services face-to-face, through text messaging, or through phone calls. Some patients also learned about the free services from other members of the barangay, such as when a patient would take a friend to accompany her to her appointment.
In general, scheduled appointments increased ultrasound utilization. Patient education about the benefits of antenatal ultrasound screening also increased utilization. A nurse reported that her patients were more likely to request an ultrasound “when they acknowledged the benefits of the procedure.”
My colleague mentioned that it’s free, so I came with her. – Patient If the patient acknowledges the benefits of ultrasound, that they can be easily diagnosed with the help of the ultrasound, and somehow, you won’t have a hard time requesting them to get an ultrasound. – Nurse
Client-related enablers
HCW client’s interests
Ultrasound scans contributed to a sense of preparedness, peace, and assurance among patients. Patients primarily wanted to get an ultrasound scan to check their own health status and that of their baby’s. Patients appreciated knowing that their baby’s heartbeat and movements were normal. These scans also provided patients with essential information, such as the fetal age, due date, and gender, which helped them prepare for delivery.
As long as I know that there’s a heartbeat, I can be at peace since one of my children died, my middle child. – Patient . . .Sometimes, I am not sure if the baby’s movements are normal. At least, if I know that my baby’s heartbeat is normal, then that also means the baby is healthy. – Patient . . .My husband wants to know the gender of our baby. . .because he wants to prepare the baby’s things. He’s excited. – Patient
Ultrasound scans also allowed the HCWs to detect complications early, which resulted in timely referrals to the appropriate healthcare facility. Patients felt that they would be more ready for emergencies if they had ultrasound results. Patients with previous unplanned abortions were also more likely to seek ultrasound scans.
Acceptance of ultrasound by clients
Ultrasound services seem widely accepted by the patients in this study. Acceptance was higher among patients who were aware of its benefits and that it was required by hospital policy. In general, patients reported that there was no reason why they would decline an ultrasound. HCWs claim that patients often ask for scans actively.
The patients want it. Midwife All of our patients here always inform us whenever they haven’t received their ultrasound request. – Midwife
Client’s confidence in HCW provider’s capabilities
Ultrasound utilization was higher when the patient believed in the HCW’s ability to perform the scan properly. Most patients also trusted the results provided by their HCWs.
Barriers to ultrasound use
System-related barriers
Lack of resources
Lack of resources decreased ultrasound utilization. While some health centers had PUDs, the number remained inadequate for the population being served. In some centers, 10 barangays shared a single machine. Additionally, the device was sometimes used only for quick triage (e.g., confirming fetal heartbeat) rather than a detailed assessment of pregnancy complications due to limited training or staff availability.
Health centers also had to contend with paper shortages, which prevented them from printing the ultrasound results. Health centers had no choice but to refer patients to private clinics for antenatal ultrasound scans, but the price points at these places were beyond the financial reach of some.
Before, we didn’t have paper here, so we couldn’t print the scan. We also don’t have something like Kimbo and cannot use the ultrasound machine, so we just refer our patients to private clinics. Thus, they have to pay 800 pesos. . . The problem is that because they cannot afford the price of getting an ultrasound, they can bear not getting one. – Midwife
Distance from the health center
Patients from far-flung areas remain grossly disadvantaged. Patients sometimes have to travel long distances to reach the health center with an ultrasound device.
Provider-related barrier
Lack of capabilities
HCWs with low knowledge, skills, and confidence were less likely to promote ultrasound services. These HCWs tended to describe their level of knowledge as “primary” or “basic,” whereas they referred to physicians as “professional” or “superior.” Some HCWs stated that the two-day training workshop was inadequate because it was “short,” “basic,” “non-continuous,” or a “one-time thing.” Some skills also seemed harder to acquire. In particular, some HCWs expressed difficulty with identifying placental location, as to whether it was “anterior or posterior.” Some HCWs also noted that scans are harder to perform in early pregnancies.
It’s hard to have confidence in doing it. If it’s just the heartbeat or the baby’s position, we can do it. However, it’s really hard for us to determine the location of the placenta, whether it is posterior or anterior. – Midwife
HCWs were also hesitant to promote ultrasound services when they felt inadequately equipped to provide additional information. Some patients “want more [answers], but [the HCWs] are unable to provide these because [they] also do not know.”
Client-related barriers
Time constraints
Several factors, such as work commitments, time and distance to the health center, and personal reasons, prevented patients from acquiring ultrasound scans.
Emotional risks
Some patients deferred getting scanned because they were “scared” of potential findings and the possible side effects from perceived radiation exposure.
As for me, I don’t want to because I’m scared to know if there will be complications or not. – Patient In my case, mostly the other doctors or midwives press hard. That’s what I fear. . . When there’s a mistake in reading the result. – Patient . . .Fearsome is the radiation. – Patient
Traditions and beliefs
Some patients insist that routine ultrasounds are unnecessary because these were “not practiced” by their relatives.
Misconceptions
Misinformation about the benefits and risks of ultrasounds also reduces patient compliance. Some patients believed that ultrasounds can cause miscarriages, whereas others believed that a good first pregnancy was an adequate indication of good succeeding pregnancies.
I had an experience with a patient who had miscarriages a number of times. She thought that she was bleeding because of the ultrasound. So of course, she was traumatized. – Midwife
Attitude toward ultrasound use
Some patients also believed that the information garnered from an ultrasound scan, such as fetal gender, was unnecessary. These patients “want[ed] to be surprised during birth” and were willing to accept any outcome. Still, other patients felt like a single ultrasound was sufficient and representative of the entire pregnancy.
Lack of confidence in provider’s capabilities
Patients who perceived their HCW as poorly trained were less likely to get an ultrasound scan. As a corollary, some patients perceived their HCWs to be trainees only and, thus, were unable to perform a scan properly and independently.
Discussion
The results of this study highlight the critical role of understanding the enablers and barriers of ultrasound use in rural health centers in the Philippines, taking into account the unique characteristics of the Philippine healthcare system. Our findings indicate that (1) the provision of free ultrasound services and (2) hospital mandates pertaining to ultrasound use were substantial system-related enablers. The presence of ultrasound devices in health centers facilitated the promotion, use, and provision of ultrasound services, ultimately leading to enhanced patient safety and quality of care.
Our investigation also revealed the significance of proper training and fostering learning environments for building knowledge, skills, and confidence among HCWs. Patients were more inclined to request ultrasound scans when informed about the benefits of the procedure and the availability of free services. In addition, patients who trusted their HCWs and believed in their capabilities were more likely to undergo ultrasound scans.
The study identified several barriers to ultrasound use. Resource limitations, such as a scarcity of trained staff and ultrasound devices, contributed to reduced ultrasound utilization in rural health centers. Geographical distance from the health center also constituted a significant barrier for patients in remote areas. Existing work commitments, time constraints, and emotional concerns, including the fear of potential findings and misconceptions about ultrasound use, posed additional barriers to ultrasound utilization. Patients who doubted their HCWs’ capabilities were less likely to request ultrasound scans. Moreover, it is crucial to note that false positives or false negatives in ultrasound results could undermine patient confidence, delay necessary referrals, and contribute to anxiety, underscoring the need for thorough training and quality control.
Our findings reinforce that rural Philippine health centers face multiple challenges in providing consistent antenatal ultrasound services. Key enablers included free ultrasound availability and supportive hospital policies, while resource deficits and distance to health centers emerged as major barriers. These results align with existing evidence (e.g., iBuntis®) 7 showing improved detection rates of complications through portable ultrasound in low-resource settings.
Further, our findings parallel those from other low- and middle-income countries (LMICs) where similar patterns of resource constraints, training gaps, and patient misconceptions hinder the integration of portable ultrasound into routine antenatal care.5,6,8 For instance, prior studies in sub-Saharan Africa and parts of South Asia have likewise reported that provider confidence and community acceptance are crucial for the successful uptake of point-of-care ultrasound.5,6 This broader alignment suggests that while our study is situated in the Philippine context, the enablers (e.g., free ultrasound services and clear policy support) and barriers (e.g., lack of trained staff and limited equipment) may hold relevance in other LMIC settings facing similar infrastructural and human resource challenges.
The study offers several implications for PUD utilization in rural Philippine health centers. Firstly, free ultrasound services can alleviate financial barriers to antenatal care. Secondly, training programs can bolster provider confidence and competency. Thirdly, patient education programs can increase patient awareness and willingness. Fourthly, policy-level resource reallocation should be considered to augment the availability of PUDs and trained operators in rural health centers.
This study acknowledges several limitations. First, the research was conducted in a restricted number of rural health centers, which may limit the generalizability of its findings. Second, the study relied on self-reported data from HCWs and patients, potentially introducing recall bias. Third, our semi-structured interview guide underwent only pilot testing (rather than formal validation), which may have limited its scope and precision. Finally, the study did not explore policymakers’ perspectives, which could offer valuable insights into the provision and utilization of PUDs in rural health centers in the Philippines. Nevertheless, future research could investigate the possible impact of policy changes on the availability and utilization of PUDs.
The feasibility of scaling up PUD usage hinges on on-the-job and preservice training, cost analyses for consumables (e.g., gel and printing supplies), and quality-control processes (regular audits, refresher courses). While initial donations reduce hardware costs, consistent usage demands policy-level support, resource reallocation, and stronger partnerships with NGOs or private stakeholders to sustain training and maintenance.
Addressing these barriers—limited operator confidence, mistrust among patients, and distance constraints—can boost PUD adoption, bridging essential diagnostic gaps. However, false positives/negatives remain a risk, underscoring the need for robust training and supervision to maintain diagnostic quality.
Conclusion
This study demonstrates that enablers (e.g., free ultrasound services, strong policies, skilled providers, and patient awareness) and barriers (e.g., limited resources, travel distance, low provider confidence, and patient misconceptions) collectively influence PUD utilization in rural Philippine health centers. Tackling these system, provider, and client factors through well-resourced programs and continuous education can significantly improve maternal outcomes and reduce maternal and fetal mortality rates.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251330991 – Supplemental material for Enablers and barriers to the use of portable ultrasound devices for antenatal care in rural health centers in the Philippines
Supplemental material, sj-docx-1-smo-10.1177_20503121251330991 for Enablers and barriers to the use of portable ultrasound devices for antenatal care in rural health centers in the Philippines by Jacob Anthony Batuhan, Reynan Hernandez, Florentina Villanueva, Airen Sigue, Kevyn Yu, Kate Wad-asen, Beatriz Carandang and Jeremie Bartelheimer in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the healthcare workers and patients at the rural health centers in Lucban, Quezon; Tagkawayan, Quezon; Tondo, Manila; Binondo, Manila; and Bantayan Island, Cebu, who participated in this study and generously shared their experiences. Their insights were invaluable to the research. We also acknowledge the logistical and technical support provided by the Department of Health, Philippines, and the local health units involved.
Statements and declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.