
Abstract
Introduction:
Primary healthcare is the most accessible and affordable form of healthcare for Nigerians. It offers primary prevention strategies such as routine immunization. Routine immunization at government facilities, including primary healthcares, is provided free of charge under Nigeria’s Expanded Program on Immunization. However, gaps such as a shortage of healthcare workers, inadequate infrastructure, and poor supply chain management can hinder the effective delivery of immunization services. This study assessed factors affecting the quality of immunization service delivery in Primary healthcares in Akinyele and Lagelu local government areas in Oyo State, Nigeria.
Methods:
A convergent parallel mixed-methods cross-sectional design was adopted, combining quantitative data from 127 healthcare workers across 40 primary healthcares from the two local government areas with qualitative data from 10 in-depth interviews. Quantitative data were analyzed using descriptive statistics and Chi-square tests, while qualitative data were analyzed thematically.
Results:
Across both local government areas, over 85% of healthcare workers received pre-service or onsite cold chain training and routinely provided immunization information. In Akinyele, onsite training was significantly associated with satisfactory cold chain management (χ2 = 10.039, p = 0.002), while in Lagelu, healthcare workers’ knowledge was associated with satisfactory cold chain practices (χ2 = 7.004, p = 0.008). Qualitative interviews revealed that Lagelu’s consistent Basic Healthcare Provision Fund funding facilitated regular outreaches, whereas Akinyele’s dependence on out-of-pocket payments led to intermittent services. Both local government areas faced cold chain equipment shortages and reliance on temporary staff. Quantitative and qualitative study findings show that reliable funding and targeted training ensure consistent outreach and effective cold chain management.
Conclusion:
While previous studies have documented funding and cold chain gaps, this study uniquely demonstrates how localized Basic Healthcare Provision Fund access specifically stabilizes outreach but fails to address workforce and infrastructure deficits. Expansion of Basic Healthcare Provision Fund-like financing across primary healthcares, transition to permanent, competitively compensated immunization staff, investment in renewable-energy cold chain technologies, and integration of community-driven outreach into the existing healthcare framework will improve immunization service delivery.
Keywords
Introduction
Immunization is one of the most effective and cost-efficient public health interventions, preventing over 4 million deaths annually. 1 The Expanded Program on Immunization (EPI) in Nigeria aims to protect under-five children against a range of vaccine-preventable diseases (VPDs), including polio, measles, diphtheria, whooping cough, tetanus, tuberculosis, yellow fever, hepatitis B, Haemophilus influenzae type b, pneumococcal diseases, rotavirus, human papillomavirus, and vitamin A deficiency.1–3
Immunization completeness in Nigeria is mainly assessed as 3 doses of the Pentavalent vaccine (Penta 3) recorded in an immunization card. 4 Improvements in healthcare access, disease prevention programs, and child survival interventions have contributed to a steady decline in under-five mortality in Nigeria over the past decades. 5 However, routine immunization (RI) coverage remains sub-optimal due to challenges including inadequate funding, resource limitations, and policy gaps. 5 Nigeria has a high proportion of children who did not receive or who missed vaccinations, accounting for 3 million of the world’s 20 million under- and unvaccinated children. 1 The national RI coverage in Nigeria stood at 57% in 2021, with Penta 3 as the coverage indicator. 6 Furthermore, only 36% of children aged 12–23 months received all recommended vaccines, while 18% of children in this age group did not receive any vaccinations. 6
Primary healthcare (PHC) is critical in delivering RI to children aged 0–23 months. It is the most accessible form of healthcare, with facilities often located within or near communities. 7 Inputs such as funding, availability of and accessibility to PHC facilities, availability of trained healthcare workers (HCWs), and the vaccine supply chain play integral roles in the delivery of EPI through PHC. However, vaccine shortages, inadequate storage, and staff limitations affect immunization service delivery and national RI coverage. 7 Available data indicate that Nigeria has an average of 17 health facilities per 100,000 people, yet only about 20% of these facilities operate under optimal conditions. 8 The current health workforce density is 0.4 doctors, 1.6 nurses, and 0.2 Community Health Extension Workers (CHEWs) per 1000 population.8–10 In comparison, the WHO recommends a minimum threshold of 4.45 doctors, nurses, and midwives per 1000 population to achieve universal health coverage, highlighting a significant shortage in Nigeria’s healthcare workforce. 11 The availability of these inputs at a quality level positively impacts health outcomes (national RI coverage).
Oyo State has historically exhibited poor RI performance, with sub-national coverage fluctuating between 22% and 33%. 12 According to the most recent Multiple Indicator Cluster Survey (MICS), 34% of children in Oyo State were fully vaccinated, 55% were partially vaccinated, and 11% were unvaccinated. Within the southwestern region, Lagos had the highest full immunization coverage at 66%, followed by Ekiti (62%) and Osun (47%), whereas Ogun and Ondo reported 39% and 30%, respectively. 6 This suboptimal coverage raises concerns regarding the effectiveness of RI service delivery in PHC facilities across the state. By 2028, Nigeria is expected to assume full financial responsibility for its immunization system, following its transition from Global Vaccine Alliance (GAVI) support. 13 The country’s readiness for this transition depends on having a resilient health system with skilled workers, appropriate immunization policies, and sufficient financial resources to sustain vaccine procurement, storage, and personnel. 14 Systemic challenges are at the root of Nigeria’s input and service delivery, especially health financing and governance. These hinder the availability of inputs and quality of service delivery, thereby hindering health outcomes. 15 Policies and governance alone cannot strengthen the PHC system without adequate inputs. Similarly, the EPI cannot achieve its intended impact of reducing under-five mortality without sufficient resources and workforce.
Immunization challenges in Nigeria, including cold chain deficiencies, workforce shortages, caregiver hesitancy, and socio-cultural norms, have been extensively documented at national and regional levels. 16 Despite evidence of suboptimal training outcomes in other Nigerian states, a critical gap remains in understanding localized health system dynamics in Oyo State. Specifically, facility-level HCW competencies in applying cold chain protocols and their adherence to immunization schedules are under-researched. 16 Studies in Sokoto and Ondo States have highlighted regional disparities in immunization coverage due to socio-cultural and infrastructural factors.17–20 Participatory action research has improved immunization coverage in areas like Remo North in Ogun State; however, its effectiveness in Oyo State, where coverage fluctuates between 22% and 33%, remains unexamined. 21 Moreover, detailed investigations into PHC service delivery challenges are scarce in Oyo State.
Addressing the lack of empirical evidence on Nigeria’s policy preparedness for the 2028 GAVI support cessation, particularly in workforce and governance adaptations for immunization financing, is crucial. 16 This study addresses critical gaps in our understanding of immunization challenges in Oyo State by evaluating healthcare provider competencies, systemic service delivery barriers, and governance preparedness within the PHC system. Specifically, immunization service delivery was assessed at PHC facilities in Akinyele and Lagelu local government areas (LGAs), focusing on the accessibility and affordability of services, the availability of HCWs, and their knowledge of immunization concepts and cold chain management. The findings will inform strategies to enhance RI coverage and ensure program sustainability beyond the GAVI funding period.
Materials and methods
Study area: This study was conducted in Oyo State, which comprises 33 LGAs. The focus was on Lagelu and Akinyele LGAs. According to the 2021 Multiple Indicators Cluster Survey/National Immunization Coverage Survey (MICS/NICS) survey, Oyo State had a Penta 3 coverage of 57%, with 20 of the 33 LGAs (61%) having a coverage above 50%. Specifically, Lagelu LGA had a coverage rate of 80.2%, while Akinyele had 46.3%. 6 Both Lagelu and Akinyele LGAs are located in the central part of Oyo State, making them easily accessible from other parts of the state, and they border each other. Lagelu LGA has a total population of about 215,149 and an under-five population of 43,030, while Akinyele LGA has a total population of about 211,811 and an under-five population of 42,362. 6
The two LGAs have similar amounts of available resources, including infrastructure, personnel allocation, vaccine supply chain, funding, and operational support, all of which are essential for effective PHC immunization service delivery. Despite these similarities, differences in immunization outcomes suggest that additional factors, such as service efficiency, community engagement, and health-seeking behavior, may influence RI coverage. The two LGAs also share similar geographical landscapes. The presence of both urban and rural settlements predisposes residents to regional differences in accessing basic health services, including the utilization of PHC facilities for RI. These disparities, in turn, impact overall health quality and immunization coverage outcomes.
Study design: A convergent parallel mixed-methods, health facility-based cross-sectional study was conducted in Akinyele and Lagelu LGAs, Oyo State, to assess immunization service delivery. This study design was adopted to enable the triangulation of quantitative and qualitative data, providing a more robust and comprehensive understanding of the intricate factors influencing service delivery. Quantitative methods (semi-structured questionnaires and observation checklists) were used to measure HCWs’ knowledge, availability of training, cold chain equipment, outreaches, and vaccines. Simultaneously, qualitative methods (in-depth interviews (IDIs)) explored the individual experiences, perspectives, and contextual barriers and facilitators to effective immunization programs. The concurrent collection of data and initial separate data analyses allowed the integration of findings at the interpretation stage. This integration, achieved through side-by-side comparisons and a joint display table, facilitated a more valid and contextualized interpretation of immunization service delivery than either method could provide alone, allowing for both a broad assessment and an in-depth understanding of the research problem (Table 1).
Joint display table for qualitative and quantitative findings.

The qualitative component of this study adopted IDIs to facilitate a flexible and exploratory approach, allowing for a detailed understanding of respondent perspectives and experiences. This method enabled the identification of contextual factors that structured questionnaires might overlook. These interviews, lasting 45–60 min, were conducted at PHC facilities and LGA offices to ensure confidentiality. Discussions, guided by literature, explored EPI implementation, including service access, HCW competence, and barriers, with a focus on identifying best practices for program improvement.16,22–24
The quantitative component utilized a semi-structured questionnaire, administered through the Kobo Collect developed by Kobo, and an observation checklist to assess immunization service delivery. The questionnaire, adapted from previous studies, evaluated facility profiles, HCW socio-demographics and knowledge, personnel availability, immunization schedule adherence, cold chain management, and service accessibility and affordability.7,9,16,25,26 The observation checklist, adapted from the WHO-UNICEF Effective Vaccine Management Assessment Tool (EVMAT), assessed input availability and service delivery practices during RI sessions. 27
Study population: The study targeted HCWs directly involved in RI services. This included Local Immunization Officers (LIOs), Cold Chain Officers (CCOs), and Routine Immunization Focal Persons (RIFPs) at all government-owned PHC facilities in Lagelu and Akinyele LGA.
Eligibility criteria
Inclusion criteria: The study included HCWs directly administering vaccines at selected PHC facilities, with a minimum of 6 months of experience, and who provided informed consent. Additionally, LIOs, CCOs, and RIFPs at the LGA and facility levels who consented were included.
Exclusion criteria: HCWs were excluded if they were not directly involved in immunization service delivery, had less than 6 months of experience in immunization-related roles, or were unavailable during data collection.
Sample size: The sample size for HCWs was determined using Cochran’s formula for a single population proportion in a cross-sectional study. Parameters employed included a 95% confidence interval (Z = 1.96), an estimated proportion (p) of 0.5 (based on HCW knowledge of vaccine cold chain management from an Ethiopian study, and a 5% margin of error (e = 0.05)). This calculation yielded an initial sample size of 384. 22
The total number of PHC HCWs in Akinyele and Lagelu LGAs was 190 (Akinyele LGA = 102, Lagelu LGA = 88). Given this finite population size (N = 190), a finite population correction was applied, as recommended for target populations below 10,000.28,29 This correction resulted in a final sample size of 127 HCWs.
Sampling technique
A multistage sampling approach was employed to select study participants.
Stage 1 (Selection of LGAs: Lagelu and Akinyele LGAs were purposively selected based on their contrasting Penta 3 immunization coverage, representing high (80.2%) and low (46.3%) coverage within the Ibadan metropolis, respectively. The selection of these LGAs, with their contrasting Penta 3 coverage, provided a basis for analyzing variations in immunization service delivery within the Ibadan metropolis.
Stage 2 (Selection of Health Facilities): All 40 government-owned PHC facilities (PHCs) offering RI services within the two LGAs were included in the study. This comprehensive inclusion, rather than sampling, ensured a thorough evaluation of immunization service delivery across all eligible PHCs.
Stage 3 (Selection of Respondents): All eligible HCWs directly involved in RI services at the selected PHCs were included. This included all HCWs responsible for vaccine administration, LIOs, and CCOs at the LGA level. No sampling was performed at this stage; instead, a complete enumeration ensured representation of all HCWs responsible for immunization service delivery.
Data collection
Qualitative data collection: IDIs were conducted to explore the implementation of EPI and the influence of input availability on immunization service delivery. Two qualitative researchers, a male and a female, conducted the interviews. Both researchers possess bachelor’s degrees in public health, maintain affiliations with the University of Ibadan, and underwent comprehensive training in qualitative methodologies and research ethics. They had no prior relationship with the participants and maintained reflexivity throughout the study by keeping detailed field notes documenting their assumptions and contextual observations.
A census approach was used to include all critical immunization roles across two LGAs: both LIOs (n = 2) and CCOs (n = 2) participated and six RIFPs (n = 6) from selected PHC facilities were purposively sampled based on their direct involvement in immunization service delivery and supply chain management. Participants were approached face-to-face at their workplaces, achieving a 100% participation rate with no refusals or dropouts. All interviews were conducted in private rooms at the participants’ workplaces to ensure confidentiality.
An IDI guide was developed specifically for the study and pilot tested with one representative from each role. The guide contained open-ended questions, with probing used to explore key issues and emerging themes in depth. LIOs and CCOs discussed topics such as policy implementation, resource allocation, and cold chain management, while RIFPs focused on facility-level operational challenges. Interviews lasted between 45 and 60 min, were audio recorded with consent, and supplemented by field notes.
The sample size was determined based on role relevance and the concept of data saturation. 30 Thematic analysis was conducted iteratively alongside data collection using inductive coding. Preliminary analysis after eight interviews (comprising two LIOs, two CCOs, and four RIFPs) indicated that saturation had been reached. To confirm, two additional RIFPs were interviewed; as no new themes emerged, the research team concluded that saturation was achieved at a total of ten interviews, ensuring comprehensive coverage of the study themes without unnecessary redundancy.
The quantitative data collection involved two tools: a semi-structured interviewer-administered questionnaire and an observation checklist. A semi-structured questionnaire was used exclusively for quantitative data collection among all eligible HCWs (n = 127) across the selected PHCs, including LIOs and CCOs. The questionnaire contained five sections, which included facility profile, socio-demographic characteristics of HCWs, PHC access and affordability for immunization services, availability of trained HCWs, and HCWs’ knowledge of basic immunization concepts, immunization services, and cold chain management.
An observation checklist, adapted from the WHO-UNICEF Effective EVMAT was used to assess input availability and service delivery practices during RI sessions at 40 government-owned PHCs, comprising 19 in Lagelu and 21 in Akinyele LGA.
Study variables: The study comprised both independent and dependent variables. The primary dependent variable was vaccine cold chain management practice, while independent variables included HCWs’ knowledge of cold chain management and participation in onsite training. Additional independent variables assessed included HCWs’ knowledge of immunization services, the availability of trained personnel, immunization outreaches, vaccines, and storage facilities. 22
Main study variable measurement: Knowledge of vaccine cold chain management was assessed using a 20-point questionnaire covering vaccine vial monitor (VVM) interpretation, the shake test, the first-expiry-first-out (FEFO) principle, and temperature monitoring. 22 A score of ⩾50% (⩾10 points) indicated adequate knowledge, a threshold informed by studies in similar low-resource settings where baseline knowledge is often limited.31,32
Vaccine cold chain management practice was measured using an 11-point checklist adapted from the WHO-UNICEF EVMAT, assessing vaccine handling, storage, and adherence to cold chain protocols. While the EVMAT does not establish rigid thresholds, its core principle lies in the necessity of continuous temperature monitoring and the implementation of timely corrective actions to maintain vaccine potency. 27 A 50% benchmark (⩾6 points) was applied to distinguish between adequate and inadequate practices, aligning with research in similar contexts where systemic constraints affect adherence to best practices.30,31 This threshold facilitates targeted interventions for quality improvement while ensuring alignment with EVMAT’s focus on progressive capacity strengthening rather than rigid pass/fail categorization. 27
Other study variables, such as the availability of trained HCWs, the availability of immunization outreach programs, and the availability of vaccines and storage facilities, were assessed through the use of structured questionnaires and facility observation checklists.
Pretesting of data collection tools: The research instruments were pilot-tested among HCWs in Ona LGA, a site excluded from the main study. This pilot testing aimed to assess the clarity, relevance, and reliability of the questionnaire items in capturing the intended variables, as well as to ensure that the questions effectively addressed the study objectives without ambiguity. A pretest sample comprising 10% of the targeted HCW population was selected in line with best practices in survey research, which recommend using a small, yet representative, subset of the population to identify potential issues. 33
Data analysis: Quantitative data were analyzed using both descriptive and inferential statistics with STATA 15 developed by StataCorp. Descriptive analysis involved frequency, percentage, mean, and standard deviation, as appropriate. Associations between variables were tested using Chi-square at a 95% confidence interval (α = 0.05).
Data analysis, using Atlas.ti version 9 developed by Lumivero, LLC, occurred concurrently with data collection, guided by a grounded theory approach. Two researchers independently coded transcripts using inductive coding, iteratively developing a code book to categorize themes such as resource allocation and cold chain management.34,35 This approach allowed theory to emerge directly from the data, reinforcing the grounded theory methodology. Data saturation, reached after 10 interviews (eight preliminary, two confirmatory), was defined as the absence of new themes.
Preliminary findings were validated through member checking with all participants, despite time constraints preventing full transcript return. Coder triangulation and participant quotations (‘Cold chain inadequacy causes logistical challenges–RIFP_003’) ensured consistency between raw data and findings.34,35 Major themes included resource gaps and policy implementation barriers with minor themes such as travel time to access immunization services also identified.
Duration of the study: The study was conducted over 2 months, from November to December 2023.
Ethical considerations
The Oyo State Ministry of Health’s Ethical Review Committee granted ethical approval for the study (NREC number: NHREC/OYOSHRIEC/10/11/22). Participants provided both verbal and written informed consent, were fully briefed on the study’s objectives, and were assured of the confidentiality of their data.
Results
The quantitative study involved 127 HCWs aged 20–62, with a mean age of 39.6 ± 10.6 years. Of these, 122 (88.2%) were female, 78 (69.1%) identified as Christians, all were of Yoruba ethnicity, and 99 (78%) were married. Regarding education, 65 (51.2%) held Ordinary National Diploma (OND)/diploma degrees, and 34 (26.8%) were CHEWs. Professional experience ranged from 1 to 39 years, with a mean of 14.5 ± 9.7 years, while experience in RI services ranged from 1 to 30 years, with a mean of 10.2 ± 8.3 years. A majority (59.8%) had over 10 years of professional experience, and 44.1% had over 10 years of experience in immunization services (Table 2). The qualitative interview included two LIOs, two CCOs, and six RI service providers.
Socio-demographic characteristics of healthcare workers.
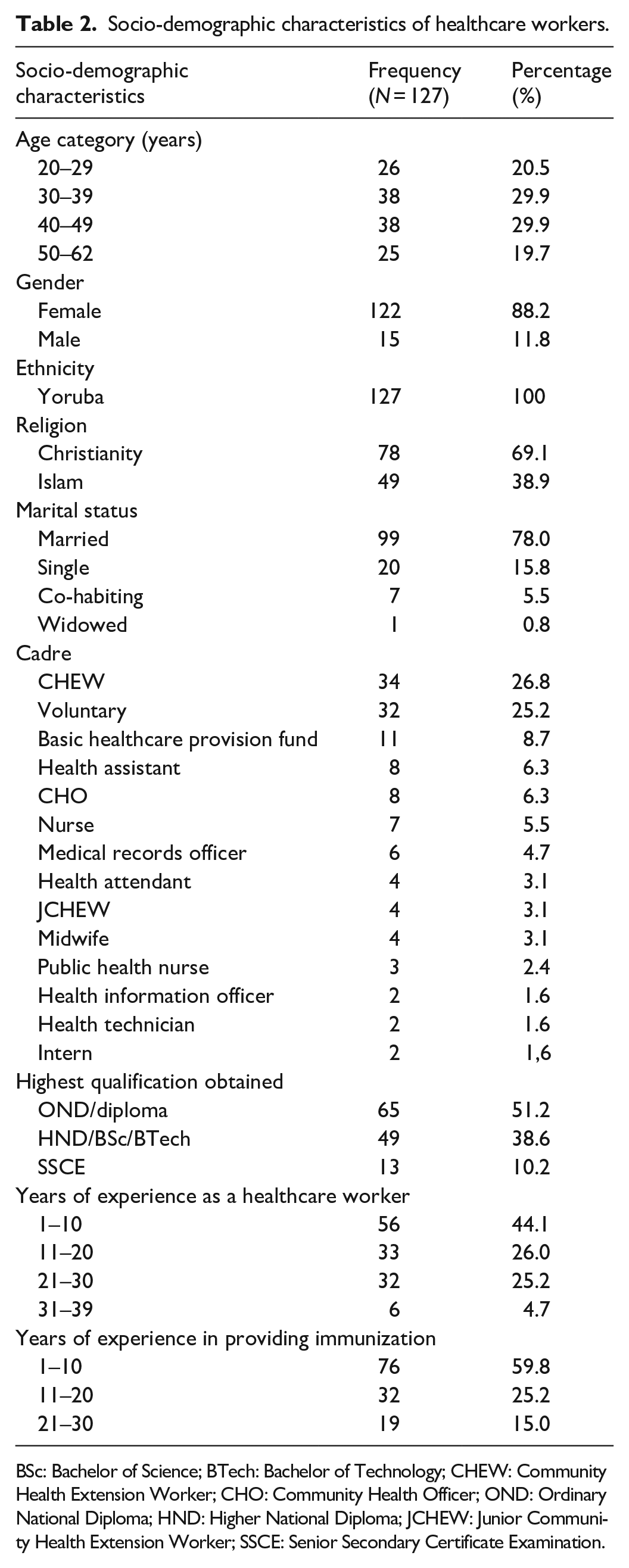
BSc: Bachelor of Science; BTech: Bachelor of Technology; CHEW: Community Health Extension Worker; CHO: Community Health Officer; OND: Ordinary National Diploma; HND: Higher National Diploma; JCHEW: Junior Community Health Extension Worker; SSCE: Senior Secondary Certificate Examination.
Availability of trained HCWs providing immunization services and information about immunization services
In Akinyele, 89.9% (n = 71) of HCWs received preservice training, compared to 83.3% (n = 40) in Lagelu. Onsite vaccine management training was received by 87.3% (n = 69) of Akinyele HCWs and 85.4% (n = 41) of Lagelu HCWs. Supervision and technical support were provided to 97.5% (n = 77) of Akinyele HCWs and 97.7% (n = 47) of Lagelu HCWs. Access to updated immunization information and resources was reported by 96.2% (n = 76) of Akinyele HCWs and 100% (n = 48) of Lagelu HCWs. Health Information System (HIS) tools were accessible to 98.7% (n = 78) of Akinyele HCWs and 97.9% (n = 47) of Lagelu HCWs. HIS tool training was received by 39.2% (n = 31) of Akinyele HCWs and 43.7% (n = 21) of Lagelu HCWs. Finally, immunization information was provided to mothers and caregivers by 98.7% (n = 78) of Akinyele HCWs and 100% (n = 48) of Lagelu HCWs (Table 3).
Distribution of trained healthcare workers providing immunisation services and information about immunisation services.

IDIs across both LGAs revealed that while trained HCWs are available, their numbers are inadequate, impacting immunization service delivery in PHCs. Health facilities depended on voluntary and ad-hoc staff provided by the local government, resulting in only two to three trained HCWs per facility. This staffing shortage contributed to work overload, with the majority of qualified HCWs being CHEWs and CHOs, and the remaining staff being volunteers.
Several of my colleagues hold BSc degrees. I also have a BSc in Public Health and I am a senior CHEW- RIFP_003 Many HCWs are retired, and there is a shortage of skilled workers—RIFP_005 Qualified staff are adequately trained; when ad hoc staff are employed, the qualified personnel assume leadership and the ad-hoc staff provide only assistance—RIFP_004 We rely solely on volunteers; for example, PHC A has only two permanent staff, and there is just one in some locations. No permanent staff are available in certain cases, and facilities are managed by ad hoc personnel or volunteers. At PHC B, an ad hoc worker leads the facility, and PHC C currently employs only two staff—LIO_001
While both LGAs faced staffing constraints, state-employed staff were prioritized for professional training. In contrast, volunteers and ad hoc staff typically received capacity-building mainly during polio supplemental immunization activities (SIAs).
We lack sufficient staff to conduct capacity training regularly. Except during supplementary immunization activities, when retraining is mandated. There is a significant shortfall in capacity building—LIO_002 They are ad hoc staff. They are not trained enough. Who wants to train them? They don’t count them as staff and whenever we are being trained, they don’t ask us to come along with them—RIFP_001
HCWs in both LGAs provided health education to mothers and caregivers, covering WHO’s key messages on topics like adverse events following immunization, breastfeeding, family planning, benefits of immunization, and the RI schedule.
During RI sessions, we provide health education to caregivers, focusing on six key messages about immunization. These include informing them about the vaccines their children receive, the diseases these vaccines prevent, potential mild side effects (also known as Adverse Events Following Immunization, or AEFI), and their management. Additionally, we educate caregivers on personal hygiene, the importance of safeguarding immunization cards, and the necessity of adhering to scheduled vaccination appointments to ensure children receive all necessary immunizations without omission—RIFP_002
Knowledge of HCWs on basic immunization concepts, immunization services, and cold chain management
In Akinyele LGA, 100% (n = 79) of HCWs demonstrated satisfactory knowledge of VPDs, compared to 93.7% (n = 45) in Lagelu LGA. Knowledge of the Penta III vaccination schedule was satisfactory in 97.5% (n = 77) of Akinyele HCWs and 85.4% (n = 41) of Lagelu HCWs. For the Rota II vaccination schedule, satisfactory knowledge was observed in 82.3% (n = 65) of Akinyele HCWs and 77.1% (n = 37) of Lagelu HCWs. The correct temperature range for vaccine storage was known by 83.5% (n = 66) of Akinyele HCWs and 72.9% (n = 35) of Lagelu HCWs.
Concerning the VVM, 77.2% (n = 61) of Akinyele HCWs demonstrated satisfactory knowledge, compared to 68.8% (n = 33) of Lagelu HCWs. Understanding of the shake test was satisfactory in 83.4% (n = 66) of Akinyele HCWs and 93.7% (n = 45) of Lagelu HCWs.
In Akinyele LGA, 78 (98.7%) HCWs exhibited satisfactory vaccine cold chain management knowledge. In Lagelu LGA, 45 HCWs (93.8%) exhibited satisfactory knowledge of vaccine cold chain management.
In Akinyele LGA, 62 HCWs (78.5%) demonstrated satisfactory vaccine cold chain management practices, compared to 33 HCWs (68.8%) in Lagelu LGA.
Participants exhibited knowledge of core immunization concepts, encompassing antigen types (oral and injectable), the RI schedule, and administration procedures.
Oral polio and Rota vaccines are administered orally, whereas Penta, BCG, HBC, PCV, IPV, MCV, MEN A, and Tetanus toxoid are administered as injectables—RIFP_007 Measles vaccinations are scheduled at 9 months for the first dose and 15 months for the second dose—RIFP_008
Participants discussed the use of immunization cards as trackers to monitor children’s adherence to the RI schedule.
A vaccination history card is used alongside a tracker bag at each facility to monitor missed appointments. This system enables staff to follow up with caregivers to determine the reasons behind missed vaccinations—CCO_001
Participants were knowledgeable about vaccine cold chain management practices, with training conducted periodically, especially before polio SIAs.
Training sessions are regularly conducted, particularly in advance of campaigns. For example, despite recently completing a microplanning training where many participants have yet to submit their plans, a follow-up session was held last week—CCO_002
Affordability in terms of payment for immunization and travel time required to access immunization services
Travel time to health facilities negatively impacts mothers’ and caregivers’ adherence to children’s vaccination schedules, particularly for rural residents who often spend over 20 min reaching the nearest facility. Increased out-of-pocket expenses associated with travel further discourage adherence.
Many, especially those in rural areas, complain about transportation costs—RIFP_003
Participants emphasized the need for intensified outreach efforts to mitigate transportation costs for rural dwellers. However, the high cost and challenging terrain associated with reaching these settlements pose logistical barriers
Rural residents take about 2 h to reach the health facility, increasing outreach costs for HCWs—RIFP_005
Government policy mandates the provision of free immunization services across both LGAs. Imposing fees would create a barrier to access for mothers and caregivers at the PHC level, thereby compromising the government’s established health equity objectives for immunization programs.
It is free. If we charge, they won’t come. We assure them it’s free since the government supplies the vaccines. Although I used my own money to pick them up, I didn’t charge anyone—RIFP_004
A participant reported accepting incentives, specifically soaps, from mothers and caregivers, asserting that these were voluntary.
They occasionally donate soap voluntarily, sometimes providing 1 kg when requested. However, since we are already persua-ding people to visit the health facility, contributions are not guaranteed—RIFP_006
Accessibility of PHC services for immunization: Availability of vaccines and cold chain equipment
Most HCWs in Akinyele (76.0%, n = 60) and Lagelu (77.1%, n = 37) LGAs reported that RI vaccines are consistently available. In Akinyele LGA, all facilities had Bacillus Calmette-Guérin (BCG), Hepatitis B (HEP B), the third dose of Pentavalent (Penta III), the third dose of Pneumococcal Conjugate Vaccine (PCV III), and Yellow Fever (YF) vaccines available, while 95.2% (n = 20) had the Measles, Mumps, and Rubella (MMR) vaccines and the third dose of the Rotavirus (Rota III) vaccines. In Lagelu, all facilities had BCG, Penta III, MMR I, and YF vaccines, while 94.7% (n = 18) had HEP B and PCV, and 73.7% (n = 14) had the Rota III vaccine.
Overall, vaccines were generally readily available, except the Rota vaccine, which was inconsistently available across both LGAs.
Rota is currently unavailable; they have just gone to collect it, but it has not yet been delivered—LIO_001
All facilities in both LGAs had vaccine carriers and ice packs. In Akinyele LGA, all facilities had cold boxes, compared to 68.4% (n = 13/19) in Lagelu LGA. Thermometers were present in 95.2% (n = 20/21) of Akinyele facilities and 73.7% (n = 14/19) of Lagelu facilities. Solar direct drive (SDD) was available in 61.9% (n = 13/21) of Akinyele facilities and 52.6% (n = 10/19) of Lagelu facilities. Freezers were present in 9.5% (n = 2/21) of Akinyele facilities and 15.8% (n = 3/19) of Lagelu facilities.
All facilities in both LGAs had auto-disable syringes and safety boxes. Waiting areas for mothers and caregivers were present in 95.2% (n = 20/21) of Akinyele facilities and 100% of Lagelu facilities. Emergency trays were available in 85.7% (n = 18/21) of Akinyele facilities and 89.5% (n = 17/19) of Lagelu facilities. Access to water was more common in Akinyele (85.7%, n = 18/21) than in Lagelu (36.8%, n = 7/19).
Electricity access was higher in Akinyele (95.2%, n = 20/21) than in Lagelu (42.1%, n = 8/19). Generator availability was 76.2% (n = 16/21) in Akinyele and 36.8% (n = 7/19) in Lagelu. SDD was available in 61.9% (n = 13/21) of Akinyele facilities and 47.4% (n = 9/19) of Lagelu facilities. Fire safety equipment was present in only 4.7% (n = 1/21) of Akinyele facilities, and not present in any Lagelu facilities.
All facilities in Akinyele stored vaccines separately from other items, compared to 73.7% (n = 14/19) of Lagelu facilities. All facilities in Akinyele arranged vaccines according to the FEFO principle, as did 73.7% (n = 14/19) of Lagelu facilities. Insect-free storage areas were present in 95.2% (n = 20/21) of Akinyele facilities and 100% of Lagelu facilities. In Akinyele, 85.7% (n = 18/21) of facilities arranged vaccines for expiry date visibility, compared to 88% (n = 14/19) of Lagelu facilities. The required temperature range was maintained in 71.4% (n = 15/21) of Akinyele facilities and 63.2% (n = 12/19) of Lagelu facilities (Figure 1).
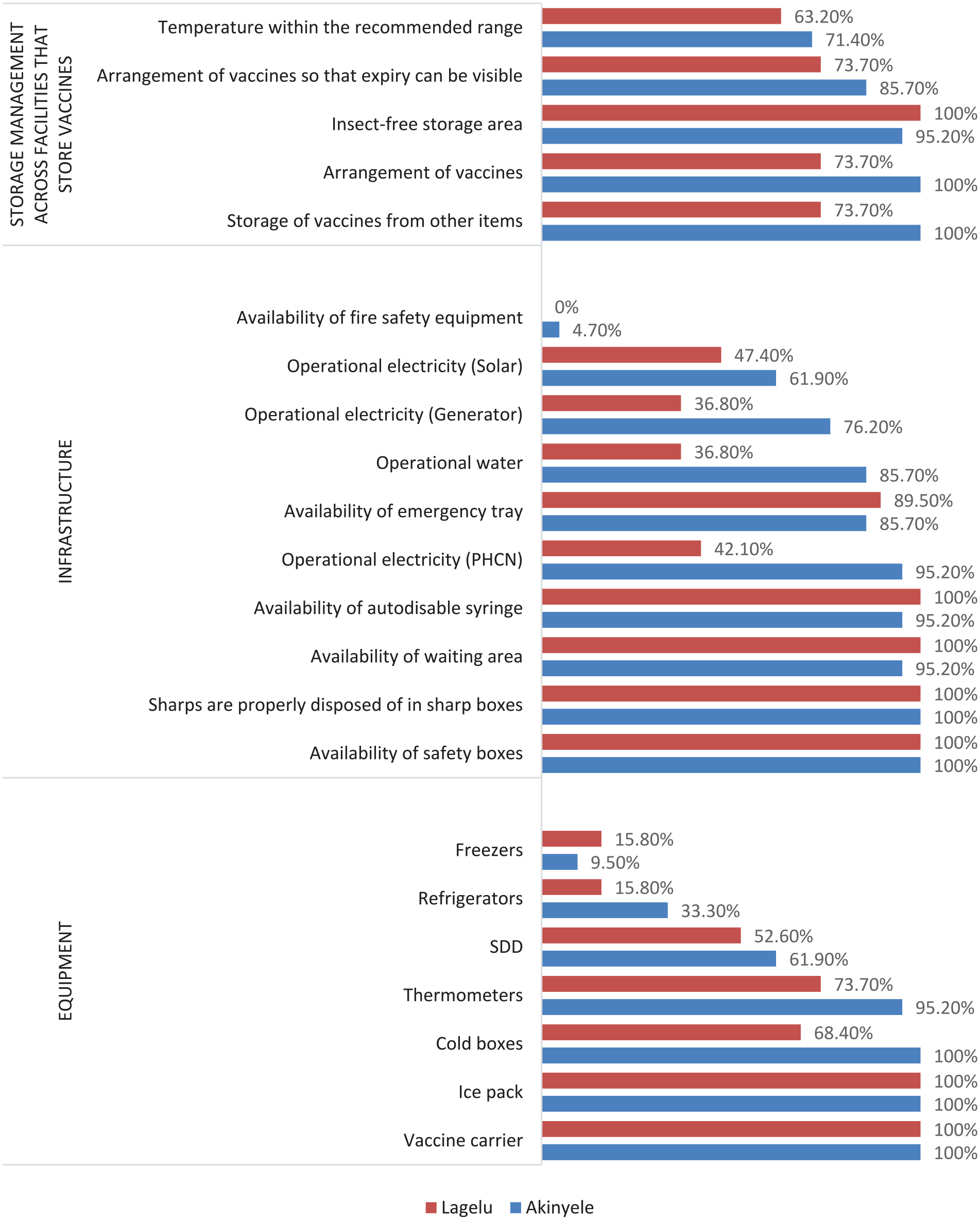
Availability of storage facilities, infrastructure, and equipment across health facilities in the two LGAs.
Most health facilities offer immunization services once or twice a week. However, the lack of adequate cold chain equipment hinders the consistent application of vaccine cold chain management knowledge. SDD is used where available; facilities without it receive weekly vaccine supplies from the LGA cold chain store.
While some facilities collect supplies monthly, those without cold chain storage collect them weekly—LIO_001 Many of them collect vaccines on the day of RI and return any leftovers to the local government office afterward. A small number, however, are equipped with SDD units for vaccine storage—LIO_002 Although our cold chain equipment is currently non-functional, we collect our monthly vaccines (antigens) from the National Program on Immunization unit at the LGA headquarters. To ensure the vaccines remain potent, we store them at a nearby PHC center equipped with a functional SDD. On Mondays and Wednesdays, which are our RI days, we only take the vaccine doses required for that day’s activities, and any unopened, unused vaccines are returned to the PHC, where they are stored. We have reported the faulty equipment and have been assured a replacement will be provided—RIFP_004
Accessibility of PHC services for immunization: Availability of outreach services
In Akinyele LGA, 88.6% (n = 70) of HCWs reported conducting outreach services, with 88.0% (n = 64) conducting them twice a month. Similarly, in Lagelu LGA, 83.3% (n = 40) of HCWs reported conducting outreaches twice a month.
Participants stated that outreach programs improve the quality of RI and increase vaccination completeness among infants. These outreaches, conducted twice monthly, primarily target rural and semi-urban areas across both LGAs.
We conduct outreach in hard-to-reach areas by going house-to-house to vaccinate children, bringing the vaccines directly to them. On outreach days, we ensure children receive all due antigens by meeting with mothers and checking their vaccination card—RIFP_002 These outreaches have expanded our reach to more villages, significantly boosting our Outpatient Department (OPD) attendance. Our consistent presence has built familiarity and trust, showing communities we offer more than just immunizations. Consequently, pregnant women are more likely to register with us, further increasing OPD numbers. During vaccination campaigns (SIAs), our familiar faces ensure greater acceptance of vaccines during house-to-house visits, unlike unfamiliar visitors—RIFP_007
At least 14 health facilities in Lagelu LGA received funding from the Basic Healthcare Provision Fund (BHCPF) under the National Primary Health Care Development Agency Impact Project. In contrast, Akinyele LGA facilities reported funding through the LGA and out-of-pocket payments.
Basic Health has been providing some financial support, at least a small payment. Within our LGA, they are currently sponsoring at least 14 healthcare facilities that are part of their business plan for conducting vaccine outreach activities—CCO_002 Basic Health currently funds outreach, we don’t have partners funding it for now—RIFP_006 It is from the coffers of the health facility that I get money to use for outreach—RIFP_003
Health facilities are required to conduct outreaches, which are included in their monthly reports, to boost vaccination coverage within their catchment areas.
The participants also said they have been able to reduce vaccine hesitancy and increase uptake, especially from non-nationals such as Cotonous and Egedes who live far away from the health facilities with the use of outreaches.
Previously, some Egede individuals did not seek immunization for their children. However, we have observed a positive change, with some now doing so. Similarly, despite initial resistance from some Cotonou residents, we have seen an increase in awareness of the value of immunization, and some are now vaccinating their children. Furthermore, some Egede individuals are now ensuring their children complete the full immunization schedule—LIO_001
Association between vaccine cold chain management practice and knowledge of vaccine cold chain management and onsite training on vaccine cold chain management
There was a significant association between satisfactory vaccine cold chain management practice and onsite training on vaccine cold chain management in Akinyele LGA (χ2 = 10.039, p = 0.002). There was a significant association between satisfactory vaccine cold chain management practice and satisfactory knowledge of vaccine cold chain management in Lagelu LGA (χ2 = 7.004, p = 0.008; Table 4).
Association between onsite training on vaccine cold chain management practice and knowledge of vaccine cold chain management, and onsite training on vaccine cold chain management.

Significant p-value < 0.05.
Discussion
This research demonstrated significant differences in immunization coverage between Lagelu and Akinyele LGAs in Nigeria, largely due to systemic disparities in the availability and distribution of financial resources. 36 Despite similar sociodemographic and infrastructural conditions, Lagelu’s consistent access to the BHCPF facilitated effective outreach programs and reliable service delivery. However, inconsistent access to BHCPF in Akinyele resulted in inconsistent immunization efforts and lower coverage. Furthermore, the limitation of BHCPF allocation to only one PHC per political ward further restricts funding availability. 37 Through a mixed-methods design, the study’s use of data triangulation provided a comprehensive analysis of systemic challenges. While quantitative data indicated a high proportion of HCWs with pre-service and on-site training, qualitative findings revealed operational challenges, including the prevalence of temporary staffing and deficiencies in cold chain infrastructure. This methodological approach underscored the limitations of relying solely on quantitative indicators, emphasizing the importance of incorporating qualitative narratives to inform policy development.
Systemic barriers: Financing and resource gaps
The most significant distinction between the LGAs was financial stability. Lagelu’s BHCPF allocation provided consistent funding for outreach programs, vaccine acquisition, and facility upkeep, enabling structured planning, regular immunization campaigns, and timely logistical responses. In contrast, Akinyele’s reliance on inconsistent out-of-pocket payments from health facilities and the LGA generated financial instability, restricting outreach frequency and vaccine availability. These findings are consistent with research in Nigeria and other resource-limited contexts, where financial instability is directly associated with reduced immunization coverage.38–40 For example, similar funding limitations in Bauchi and Cross River States disrupted vaccine supply and workforce retention, paralleling the challenges observed in Akinyele.16,41
Beyond financial factors, both LGAs experienced systemic limitations in trained HCWs, functional cold chain equipment, and specific funding for immunization strategies. While Lagelu’s BHCPF allocation offered some mitigation, Akinyele’s resource deficits were compounded by its financial instability. Furthermore, HCWs in both LGAs reported insufficient SDD refrigerators and freezers. Both LGAs’ cold chain management constraints hindered repairing or replacing malfunctioning equipment, exacerbating vaccine storage challenges. These interconnected systemic inadequacies negatively impacted workflow efficiency and service quality, underscoring the interdependence of financial, infrastructural, and human resources in effective immunization programs.
Human resource challenges: Training, retention, and workforce vulnerability
Quantitative data indicated a seemingly well-trained workforce in both LGAs, with over 85% of HCWs reporting pre-service and on-site immunization training. However, qualitative interviews revealed a significant discrepancy, with many facilities relying on temporary or volunteer staff with limited qualifications. Across both LGAs, immunization tasks were performed by ad hoc personnel who often lacked formal training in cold chain management and caregiver communication, resulting in inconsistent service delivery. In Lagelu, the BHCPF allocation enabled temporary hiring of supplementary staff, though long-term workforce sustainability remained a concern.
This reliance on transient staff highlights a systemic vulnerability. Experienced HCWs were often nearing retirement, and younger professionals tended to seek employment in urban centers or tertiary facilities, leading to understaffing in rural PHC centers. This pattern aligns with findings from Ekiti State, where high turnover and burnout among HCWs negatively impacted immunization consistency. 38
Notably, HCWs who received training in cold chain management demonstrated significantly better practices. In Akinyele, targeted training was strongly associated with effective practices, while in Lagelu, enhanced knowledge of vaccine cold chain management significantly correlated with improved practice. These findings align with similar studies from Ethiopia. 22 Although temporary workers were trained during SIAs, the absence of retention incentives led to a decline in knowledge between campaigns. Consequently, cold chain management practices deteriorate during non-SIA periods when volunteers return to other roles. This underscores the urgent need for policies prioritizing permanent recruitment, establishing clear career development pathways, and providing competitive compensation to stabilize the PHC workforce.42,43
Cold chain logistics: Infrastructure deficits and operational strain
Suboptimal cold chain infrastructure posed a major challenge. Fewer than half of the facilities in both LGAs had a functional cold chain management system. In facilities without adequate storage equipment, HCWs were forced to undertake lengthy vaccine collection routines, sometimes traveling up to 50 km. These trips depleted limited fuel supplies and took a toll on staff morale, with HCWs in Akinyele describing the process as exhausting and unsustainable. In Lagelu, although BHCPF funds occasionally covered transportation costs, equipment shortages persisted. These findings are consistent with research from Ile-Ife, where only 11.7% of facilities had adequate cold chain infrastructure, contributing to frequent vaccine wastage. 25
The lack of necessary equipment fosters a cycle of inefficiency, resulting in inadequate storage and vaccine stockouts. This challenging situation contributes to lower caregiver attendance and places excessive demands on the remaining, strained resources. 44
Caregiver engagement: Communication and community trust
Effective communication with caregivers was crucial for immunization adherence, with HCWs emphasizing vaccine schedules, side effect management, contraindications, follow-up dates, nutritional advice, and misinformation correction. In Lagelu, consistent outreach fostered repeated interactions, enhancing caregiver trust. Akinyele’s intermittent outreach hindered message reinforcement, which might lead to caregiver confusion regarding schedules. This finding is consistent with studies in Bauchi and Cross River, where consistent HCW-caregiver dialogue significantly improved immunization uptake.16,41
However, staffing instability negatively impacted communication effectiveness. Temporary workers often lacked familiarity with local dialects and cultural nuances, impeding rapport-building. This highlights the necessity of a permanent, culturally competent workforce to maintain caregiver trust and ensure effective communication.
Outreach and equity: Funding’s role in service accessibility
Although the EPI guarantees free services, Akinyele’s reliance on out-of-pocket payments resulted in indirect costs such as transportation expenses incurred by HCWs, thereby diminishing the frequency of outreach services. In contrast, Lagelu’s BHCPF actively supported outreach initiatives by deploying dedicated teams to underserved communities, a strategy that echoes successful interventions in southwest Nigeria, where mobile units contributed to a 30% increase in measles vaccination coverage. 38
Moreover, enhanced financial stability had a positive impact on HCWs’ morale. HCWs in Lagelu expressed satisfaction and pride in their capacity to reach every child, whereas their counterparts in Akinyele reported frustration over preventable service delivery gaps. These contrasting experiences underscore the dual role of financial resources in optimizing logistical operations and bolstering the motivation of frontline healthcare providers.
Overall, this study highlights the importance of consistent and dedicated financial support, exemplified by the BHCPF, in achieving robust immunization service delivery. 37 Such financial backing is crucial for addressing systemic challenges and improving immunization coverage in resource-constrained settings like Oyo State, Nigeria.
Limitations
This study has several limitations. It was confined to government-owned PHC facilities that provide RI within two LGAs in Ibadan, Oyo State, Nigeria, and used Penta 3 coverage exclusively as the immunization indicator. As the findings are specific to the Lagelu and Akinyele LGAs, caution must be exercised when generalizing the results to other settings. Furthermore, the study did not include the end users: mothers and caregivers of children below the age of two. Future research should aim to replicate the study using a larger sample size and incorporate additional immunization indicators to enhance the robustness of the PHC immunization system and broaden applicability to other contexts.
Conclusion
This study highlights the systemic challenges affecting immunization service delivery in Oyo State, Nigeria, particularly in light of the impending phase-out of GAVI funding. The analysis reveals that the BHCPF has proven effective in stabilizing outreach efforts in Lagelu LGA. However, the BHCPF has not adequately addressed issues related to workforce instability, deficiencies in cold chain infrastructure, or equitable community engagement. To ensure the continuity and enhancement of immunization coverage in the post-GAVI era, it is imperative to adopt a comprehensive strategy. Such strategies should include the following:
Sustainable Funding mechanisms: Expand Lagelu’s BHCPF model to all PHCs per ward, integrating state and LGA co-financing. Explore innovative funding through state health insurance and public-private partnerships for vaccines, supporting Universal Health Coverage.
Stable Workforce and Training: Transition temporary staff to permanent, competitively paid positions with clear career paths. Ensure state‑funded training in cold‑chain management, community engagement, and cultural sensitivity for consistent quality.
Modernization of Cold Chain Infrastructure: Invest in climate‑resilient, solar‑powered refrigerators via state–local partnerships. Establish LGA emergency funds for repairs and fuel to prevent stockouts and waste.
Equitable Community Outreach: Reduce service gaps by training staff in local languages and customs. Create community health trusts for mobile clinics and launch local micro-donor programs to build trust and decentralize funding.
Policy for Sustainability: Legislate BHCPF‑style funding with ring‑fenced immunization budgets. Implement strong monitoring of spending and results for accountability and policy improvement.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251352974 – Supplemental material for Evaluation of immunization service delivery in primary healthcare centers in Akinyele and Lagelu local government areas, Oyo State, Nigeria
Supplemental material, sj-docx-1-smo-10.1177_20503121251352974 for Evaluation of immunization service delivery in primary healthcare centers in Akinyele and Lagelu local government areas, Oyo State, Nigeria by Oladosu Timilehin Gbeminiyi and Ajayi IkeOluwapo Oyeneye in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251352974 – Supplemental material for Evaluation of immunization service delivery in primary healthcare centers in Akinyele and Lagelu local government areas, Oyo State, Nigeria
Supplemental material, sj-docx-2-smo-10.1177_20503121251352974 for Evaluation of immunization service delivery in primary healthcare centers in Akinyele and Lagelu local government areas, Oyo State, Nigeria by Oladosu Timilehin Gbeminiyi and Ajayi IkeOluwapo Oyeneye in SAGE Open Medicine
Footnotes
Acknowledgements
The authors appreciate all healthcare workers across the two local government areas who participated in the study.
Ethical considerations
The Oyo State Ministry of Health’s Ethical Review Committee granted ethical approval for the study (NREC number: NHREC/OYOSHRIEC/10/11/22). Participants provided both verbal and written informed consent, were fully briefed on the study’s objectives, and were assured of the confidentiality of their data.
Author contributions
Conception or design of the work: Oladosu Timilehin Gbeminiyi and Ajayi IkeOluwapo Oyeneye. Data collection: Oladosu Timilehin Gbeminiyi. Data analysis and interpretation: Oladosu Timilehin Gbeminiyi and Ajayi IkeOluwapo Oyeneye. Drafting the article: Oladosu Timilehin Gbeminiyi and Ajayi IkeOluwapo Oyeneye. Critical revision of the article: Oladosu Timilehin Gbeminiyi and Ajayi IkeOluwapo Oyeneye. Final approval of the version to be submitted: Oladosu Timilehin Gbeminiyi and Ajayi IkeOluwapo Oyeneye.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.