
Abstract
Objectives:
Effective adherence to infection prevention and control practices is needed to reduce the rate of healthcare-acquired infections among healthcare workers. Policies to control healthcare-acquired infections among healthcare workers can be designed and implemented using information on adherence to infection prevention and control practices adherence and its determinants. This study, therefore, sought to assess the adherence to infection prevention and control practices among healthcare workers during the 2019 Coronavirus disease pandemic.
Methods:
A multicentre cross-sectional study was conducted among 323 randomly selected healthcare workers in four health facilities in the Suame Municipality, Ghana. Data on participants’ socio-demographics, knowledge of infection prevention and control practices and adherence to infection prevention and control practices were collected using a pre-tested structured questionnaire. Multivariate logistic regression analysis was used to examine the effect of demographic characteristics and knowledge of infection prevention and control on adherence to infection prevention and control practices among study participants.
Results:
Over three-quarters (75.9%) of the study participants had adequate knowledge of infection prevention and control practices with a significant knowledge gap in the colour coding of bin liners for waste segregation (35.6%). The proportion of study participants who reported good adherence to infection prevention and control practices was 86.7%. Healthcare workers who were 33 years and above (Adjusted odds ratio (AOR): 0.27; 95% Confidence interval (CI): 0.08–0.92) and absence of an infection prevention and control committee at the facility AOR: 0.25; 95% CI: 0.08–0.73) had reduced odds of good adherence to infection prevention and control practices. Nursing staff (AOR: 9.49, 95% CI: 2.51–35.87) and having adequate knowledge of infection prevention and control practices (AOR: 2.66; 95% CI: 1.19–5.97) were associated with increased odds of good adherence to infection prevention and control practices.
Conclusion:
Adherence to infection prevention and control practices was high among this sample of Ghanaian healthcare workers. Interventions and strategies to improve adherence should include the setting up of infection prevention and control committees, education and strict observance of colour coding of bin liners for waste segregation and intensification of training of healthcare workers in infection prevention and control practices.
Introduction
The 2019 Coronavirus disease (COVID-19) is a recent addition to the trail of viral infections of global epidemic proportions to have hit the world over the last 2 decades. 1 Severe Acute Respiratory Syndrome, Middle East Respiratory Syndrome, Bird flu and Swine flu, among others, have hit the world during this period. The COVID-19 pandemic brought in its wake a huge burden on public health and the global economy.2,3 As of 13th December 2023, over 772.39 million cases and over 6.99 million mortalities were reported across the globe. 3 In China, some studies that were conducted at the early stages of the pandemic reported that the rate of infection was very high and the condition was reported to be very severe among the aged population and people with underlying comorbidities.4,5
Healthcare workers (HCWs) were key actors in the fight against COVID-19 and other healthcare-associated infections (HAIs). They are susceptible to infections and may serve as agents for the transmission of pathogens.6,7 The COVID-19 pandemic resulted in an increased workload on HCWs and exposed lapses in the healthcare systems in both developed and developing countries. 8 Globally, HCWs were not spared from contracting COVID-19 despite the adoption of the WHO’s infection prevention and control (IPC) recommendations including hand washing before and after attending to patients, usage of recommended personal protective equipment (PPE) and capacity building in IPC.9–11 The WHO confirmed over 115,000 global COVID-19-associated mortalities among HCWs after 18 months of the pandemic. 9 In the USA, Kiang et al. 12 reported an excess mortality of 43 per 100,000 person-years among physicians during the COVID-19 pandemic. In an umbrella review involving 13 systematic reviews, a case fatality of 9 deaths per 1000 infections among HCWs across the globe was reported. 13 A study reported 293 COVID-19-associated mortalities among Physicians in Italy between March 2020 and October 2021. 14 In sub-Saharan Africa, a study in South Africa reported that out of a total of 169,678 COVID-19 hospital admissions from March 2020 to April 2021, about 3.8% (6364) were HCWs. 15 In Ghana, as of July 2021, over 2000 HCWs had been infected with COVID-19. 16
Formulating policies and guidelines at the workplace to prevent and control infections is critical to reducing occupational exposures and HAIs. 17 Strict adherence to IPC practices at the workplace is a vital measure in reducing COVID-19 and other HAIs among HCWs.18,19 In a case-control study among HCWs in Ghana, COVID-19-positive cases were about 71% more likely to be poorly adherent to hand hygiene or PPE usage. 20 Good adherence to IPC practices can be facilitated by effective training and the provision of PPE as well as routinely auditing safety measures. 21 A study reported that HCWs who did not receive training on PPE had two times increased odds of non-compliance to IPC practices. 22
Few studies in Ghana have assessed IPC practices among HCWs amidst the COVID-19 pandemic.20,23–25 About 9.1–80.8% adherence to IPC practices during the COVID-19 pandemic was reported among HCWs in Ghana.20,23,25 Ashinyo et al. 23 reported that non-clinical staff had 57.0% reduced risks of adherence to hand hygiene compared to clinical staff. Abatanie et al. 25 in their study found that about 60.2% of HCWs had adequate knowledge of COVID-19 safety protocols. However, no study in Ghana has assessed the relationship between HCWs’ knowledge of IPC measures and adherence to IPC practices. This study, therefore, sought to assess adherence to IPC practices and their predictors among HCWs in the Suame Municipality, Ghana. It also assessed HCWs’ knowledge of IPC practices and their relationship with IPC adherence.
Methods
Study design, setting and population
This was a multicentre cross-sectional study that was conducted among HCWs in four health facilities, namely Bremang SDA Hospital, God’s Glory Hospital, Jomo Medical Centre and Wisdom Specialist Hospital in the Suame Municipality of the Ashanti Region of Ghana. The first two are quasi-government facilities, while the other two are privately owned. The study was conducted from 4th October 2021 to 29th December 2021.
The Suame Municipality is one of the 38 newly created districts in the country with an estimated population of over 250,000 people. There are 26 health facilities in the municipality, the majority of which are private. The four facilities used in this study, each from one of the four towns in the municipality, were purposively selected as they were actively involved in the case detection, management and contact tracing of suspected COVID-19 patients in the municipality.
The target population was both clinical (nursing staff, doctors, laboratory technicians, pharmacists and physician assistants) and non-clinical staff (records personnel and administrative staff). We included all HCWs in the four facilities who had their permanent license and were fully engaged. However, all students on clinical attachments and national service personnel undergoing their 1-year mandatory service in the four health facilities were excluded from the study.
Sample size calculation and sampling technique
The sample size was estimated using the Charan and Biswas 26 formula by assuming a 30.7% prevalence of adherence to IPC practices from a previous study, 27 at a 95% confidence interval and an allowable margin of error of 5%. Accounting for a 10.0% non-response rate, a total of 360 participants were estimated for the study.
A simple random sampling technique was used to select the study participants from all the health facilities. The number of HCWs that were recruited in each facility was determined using proportional allocation of sample size to the size of the target population. This was calculated by dividing the number of HCWs in each facility by the total number of HCWs in all the facilities and multiplied by the estimated sample size of 360 participants. At each facility, the staff list was drawn from the human resource department and entered into balloting using the lottery method. In all, we recruited 132 HCWs from Bremang SDA Hospital, 85 from God’s Glory Hospital, 76 from Wisdom Specialist Hospital and 30 from Jomo Medical Centre.
Data collection tools and procedure
A structured questionnaire (see Supplemental File) was used to collect study data using a pen-to-paper approach. The questionnaire was developed by the researchers through a review of questions posed in previous studies.11,19,21,28,29 The questionnaire was not validated. However, to improve its internal validity and reliability, we adopted robust methods including the involvement of experts such as an epidemiologist, IPC consultant, biostatisticians, and public health physician to review the content of the questionnaire as well as pretesting. The questionnaire was pretested among HCWs in the Asokwa Municipality with all the important corrections being made before using it to collect the final study data. Adherence to IPC practices by HCWs can be influenced by several interwoven factors including individual and environmental factors. Hence, the development of the questionnaire for this study was guided by a conceptual and theoretical framework. Considering the main focus of this study of adherence to IPC practices amidst the COVID-19 pandemic in Ghana, the ecological model and theory of planned behaviour guided this study.30,31 These theories explain that an individual will take a particular action based on some enabling factors such as environmental and individual factors of health. It was anticipated in this study that HCWs’ adherence to IPC practices shall be determined by individual factors including age, knowledge of IPC practices and cadre of HCWs and environmental/organisational factors such as IPC committee at the facility, provision of PPE etc.
The questionnaire was used to collect data on socio-demographic characteristics (which included cadre of HCW, age, sex, relationship status, working experience etc.), knowledge about IPC (use of gloves, hand washing, infection transmission etc.) and adherence to IPC practices.
Participants’ knowledge of IPC was measured using a cumulative score of 10 questions. A correct answer was given a score of ‘1’ and an incorrect answer was given a score of ‘0’. The overall score was calculated and expressed as a percentage. The participant’s knowledge was graded based on the overall score (inadequate: ⩽30%, moderate: 40%–60% and adequate: ⩾70.0%). The assessment of participants’ knowledge of IPC was subjective and may affect direct comparison to previous studies. However, these arbitrary categorisation methods have been documented in the literature.32,33
Study participants’ adherence to IPC was assessed using 12 adherence questions (unstandardised) to determine their practices on available IPC measures. A participant who indicated following the right practice was given a score of ‘1’ and those who did not follow the recommended practice were given a score of ‘0’. The overall score was computed and expressed as a percentage. Participants who scored 70.0% and above on the adherence questions were categorised as ‘good adherence’, while those who had below 70.0% were categorised as ‘poor adherence. The investigators’ preference for HCWs to strictly adhere to IPC practices, given their importance in lowering COVID-19 infections and HAIs, led to the adoption of the 70% cut-off for good adherence.
Data quality control
Data entry was done by two research assistants independently using Epi Info version 7.2.4.0 (Centers for Disease Control and Prevention (CDC) USA). The data were exported to Stata version 16 for quality improvement and analysis. Data quality control was conducted by checking for completeness, duplication and wrong entries by the data validation team.
Statistical analysis
For all categorical variables, frequencies and percentages were determined in addition to means and standard deviations and medians and interquartile ranges for continuous variables. Measures of association were calculated to assess the relationship between demographic characteristics, knowledge of IPC and adherence to IPC practices among study participants. Multivariate logistic regression analysis was used to model the effect of demographic characteristics, and knowledge of IPC on adherence to IPC practices among study participants. Both crude odds ratio and adjusted odds ratio were presented along with a 95% confidence interval using a statistical significance of p < 0.05.
Ethics approval and consent to participate
Ethical approval for the study was obtained from the Committee on Human Research, Publications and Ethics, School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi (Reference number: CHRPE/AP/459/21). This was done after obtaining written permission from the Suame Municipal Health Directorate. All the study participants provided written informed consent before recruitment. The participants either signed or thumb printed an informed consent.
Results
Socio-demographic characteristics of study participants
Of the estimated 360 participants, 323 were recruited, yielding a response rate of 89.7%. The mean age of study participants was 26.2 (±6.3) years, with a minimum age of 18 years and a maximum age of 59 years. Approximately 58.5% of the study participants were females and over two-thirds (64.1%) of them were nursing staff. Two hundred and eighty-six of the participants (88.5%) had practised as HCWs for 1–5 years with a median working experience of 2 Interquartile range (IQR): 2) years (Table 1).
Demographic characteristics of study participants (N = 323).

SD: standard deviation; HCW: healthcare workers; IQR: Interquartile range.
Includes medical doctors and physician assistants.
Health workers’ knowledge of infection prevention control
Of the 323 participants, 75.9% had adequate knowledge of IPC practices. Majority (93.5%) indicated that HAIs can be prevented. Approximately 35.6% of the study participants indicated that a waste bin with a yellow liner is not for general waste (Table 2).
Knowledge of infection prevention and control practices among study participants (N = 323).

IPC: infection prevention and control.
Adherence to IPC practices among study participants
The proportion of study participants who reported good adherence to IPC practices was 86.7%. Over 97.8% of them washed their hands after attending to a patient. More than half (56.0%) of the recruited HCWs had received COVID-19 vaccination, and majority (96.3%) of them indicated that they had a policy on IPC practices at their facility (Table 3).
Adherence to infection prevention and control measures among study participants.
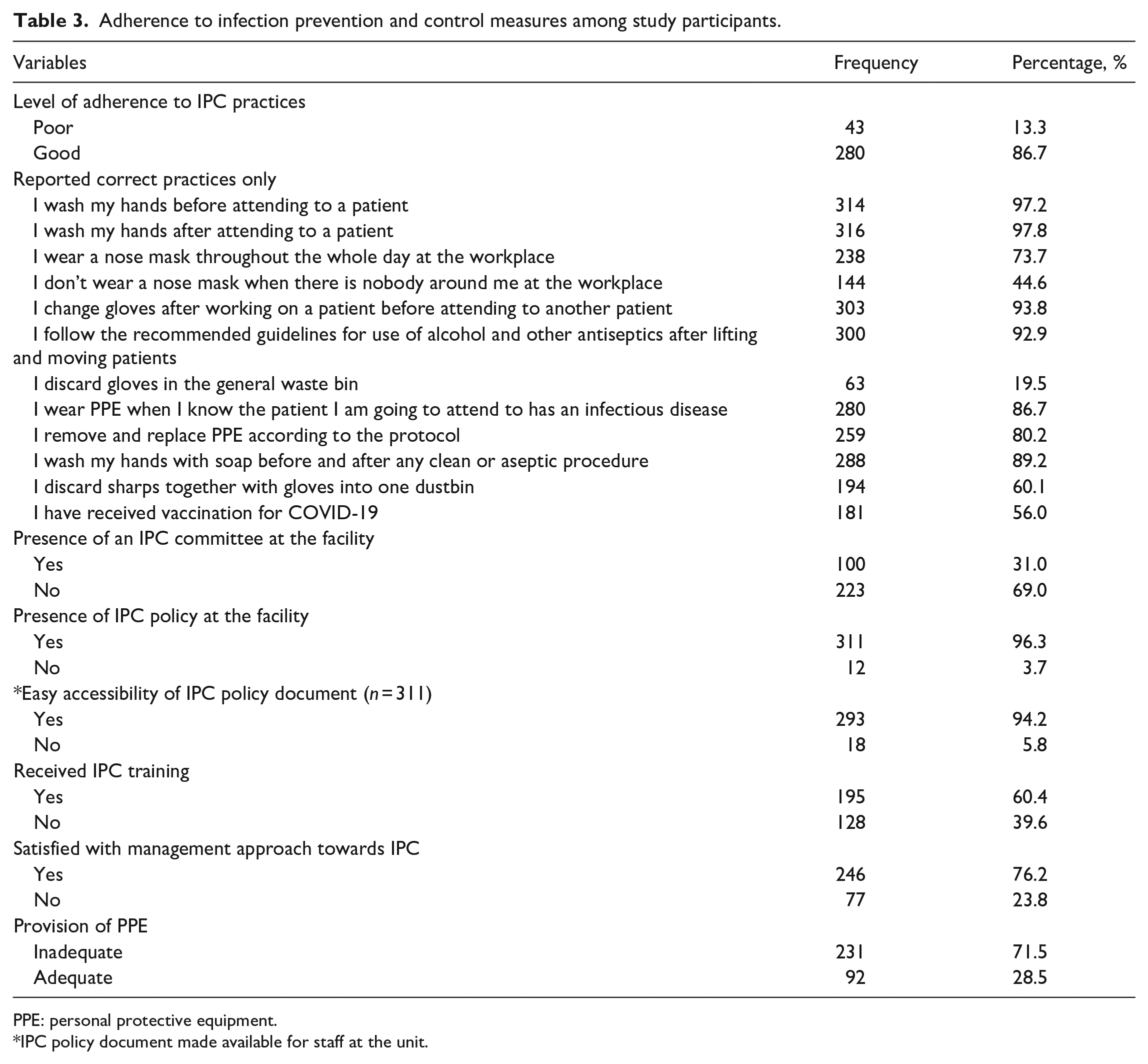
PPE: personal protective equipment.
IPC policy document made available for staff at the unit.
Predictors of adherence to IPC measures
After adjusting for significant covariates in the multivariate logistic regression analysis, HCWs who were 33 years and above (AOR: 0.27; 95% CI: 0.08–0.92) and absence of IPC committee at the facility (AOR: 0.25; 95% CI: 0.08–0.73) were associated with reduced odds of good adherence to IPC practices among the study participants. Nursing staff (AOR: 9.49, 95% CI: 2.51–35.87), prescribers (AOR: 69.76; 95% CI: 6.8–715.39) and having adequate knowledge of IPC practices (AOR: 2.66; 95% CI: 1.19–5.97) were associated with increased odds of good adherence to IPC practices among study participants (Table 4).
Multivariate logistic regression analysis of the factors associated with adherence to infection prevention and control practices.

OR: odds ratio.
Discussion
The emergence of the COVID-19 pandemic led to the significant recognition of IPC and public health worldwide. There was an increased burden on the healthcare system across the globe due to unpreparedness of the healthcare system including inadequate HCWs, health infrastructure for isolation centres and lack of education and training on IPC.34,35 The health and safety of HCWs could be enhanced through IPC practices.
The high good adherence to IPC practices (86.7%) observed in the present study is similar to the 80.8% good adherence recorded in an earlier study in Ghana 23 and the United States. 36 Consistent with this study, in China, HCWs’ adherence to IPC practices increased in the wake of the COVID-19 pandemic. 37 This is particularly pertinent to the fight against COVID-19 and a reduction in the rate of infection transmission among HCWs. Strict adherence to IPC practices at the workplace is one of the most effective measures to mitigate the spread of HAIs. 38 The high adherence to IPC measures in this study could be explained by the increased awareness of IPC practices as well as the fear of contracting the disease by the HCWs.
Knowledge of IPC practices among HCWs is key to the implementation of IPC practices at the workplace. 39 It was observed in the present study that over three-fourths (75.9%) of HCWs had adequate knowledge of IPC practices. This is comparable to earlier studies conducted in Nigeria (70.0%) and Ethiopia (84.7%), which reported adequate knowledge of IPC practices among HCWs.40,41 However, the knowledge of IPC practices among HCWs in the present study is at variance with the 50.6% that was reported among HCWs in Tamale, Ghana. 28 The high knowledge of IPC practices among HCWs in the present study may be attributed to the existence of an IPC policy in the health facilities and its easy accessibility by most of the HCWs. Again, the increased awareness creation and training of HCWs in IPC practices amidst the COVID-19 pandemic may have contributed to the adequate knowledge among the study participants unlike the study in Tamale, 28 which was conducted prior to the COVID-19 outbreak in Ghana. Despite participants’ high knowledge of IPC practices, there was a gap in participants’ knowledge of colour coding for waste segregation. Only 35.6% of HCWs had the correct response for the implication of yellow bin liners not being used for general waste. This calls for further training of HCWs on the colour coding of waste segregation.
It was observed in the present study that HCWs who had adequate knowledge of IPC practices had about three (AOR: 2.66, 95% CI: 1.19–5.97) times increased odds of good adherence to IPC practices compared to those who had moderate knowledge. Knowledge of IPC practices can influence a person’s attitude towards adherence. This is in line with other studies which reported that adequate knowledge of IPC practices among HCWs is significantly associated with good adherence.42–44 This implies that HCWs with adequate knowledge of IPC practices are likely to apply it at the workplace to improve their health and safety. It may not always be the case that adequate knowledge translates into application. However, having adequate knowledge can guide one to make a good decision or take an action that will positively benefit him/her. This highlights the need for interventions to increase IPC practices among HCWs to target increasing awareness of IPC, regular training and enhanced accessibility to IPC policies, guidelines and tools at the workplace.
Furthermore, it was observed in the present study that HCWs who worked in facilities without an IPC committee at the workplace had about 75.0% (AOR: 0.25, 95% CI: 0.08–0.73) reduced odds of good adherence to IPC practices compared to those with an IPC committee in their facilities. This finding resonates with studies conducted in Kenya 45 and Ethiopia. 46 This underscores the significance of the presence of an IPC committee on the adherence to IPC practices by HCWs. The responsibilities of an IPC committee may involve the formulation of policies/guidelines and effective implementation, coordination, monitoring and supervision of IPC practices among HCWs in the workplace. We therefore recommend that potential strategies to increase adherence to IPC practices among HCWs should include setting up an IPC committee in all health facilities.
We also observed in the current study that the age groups of study participants were significantly associated with adherence to IPC practices, and this is in agreement with earlier reports.36,47 HCWs who were 33 years and above had about 73.0% (AOR: 0.27, 95% CI: 0.08–0.92) reduced odds of good adherence to IPC practices compared to those between the ages of 18 and 22 years. A possible reason could be inadequate knowledge of IPC practices among those who were 33 years and older. Also, those who were 33 years and older may have gathered some experience over the years and were very confident in their ability by not adhering to IPC measures and still not getting infected. In Ghana, younger (20–29 years) surgical healthcare providers in a teaching hospital were found to adhere more to facemask use compared to older (40–59 years) ones. 28 A qualitative study design may be useful in identifying possible reasons why older HCWs adhere poorly to IPC measures.
The cadre of HCWs was significantly associated with good adherence to IPC practices. In the present study, nursing staff (AOR: 9.49, 95% CI: 2.51–35.87), pharmacy staff (AOR: 6.98, 95% CI: 1.01–48.10) and prescribers (AOR: 69.76, 95% CI: 6.80–715.39) had increased odds of good adherence to IPC practices compared to administrative staff. This is in line with an earlier study which reported that being a nurse was associated with a higher compliance score of IPC practices. 29 Nursing staff spend a considerable amount of time with patients and are at higher risk of exposure to HAIs which can influence their adherence to IPC practices. Educational interventions including training and awareness creation to improve IPC practices should involve everyone working in the hospital setting, including administrative staff.
For effective adherence to IPC measures, the adequate provision of the right PPE is very important. It is very worrying as the majority (71.5%) of the study participants indicated inadequate provision of PPE at their workplace. This aligns with reports of a shortage of PPE in most health facilities across the world as their resources were overstretched by the COVID-19 pandemic.48,49 The lack of provision of adequate and appropriate PPEs to HCWs exposes them to a high risk of COVID-19 and other HAIs. 50 It is therefore imperative to provide HCWs with the right and adequate PPE at all times.
This study provides data that can inform the design and implementation of policies on promoting health and safety among HCWs in the workplace. The spread of COVID-19 and other HAIs among HCWs can threaten the health and safety of patients, families and the community as a whole. Adherence to IPC practices among HCWs can reduce exposure to COVID-19 and other HAIs.
Strengths and limitations
The strength of this study is the recruitment of HCWs from four different health facilities (multicentre approach) which enhances the generalizability of study findings among HCWs in the Suame Municipality. Another strength of this study is the high response rate, which improves the representativeness, quality and accuracy of the study data.
Although this study provides significant data that can help to improve HCWs’ adherence to IPC practices, it did have some limitations. The use of a quantitative study approach limited us in exploring the reasons behind non-adherence to IPC measures among the HCWs. Adherence to IPC practices in this study was assessed using self-report, which is likely to introduce bias. A previous study that adopted both self-report and observation found a variation in adherence to IPC practices with the self-report recording higher adherence to IPC practices compared to direct observation. 51 Future studies can include anonymous observation in assessing adherence to IPC practices among HCWs. Again, the large confidence intervals around some of the odds ratio estimates from the regression analysis may point to a reduced precision in the study’s findings. The tools that were used for assessing participants’ knowledge of IPC and adherence to IPC practices were not validated. However, its validity and reliability were enhanced through pretesting.
Conclusion
The majority of HCWs sampled in this study had good adherence to IPC practices amidst the COVID-19 pandemic in Ghana. Participants’ age, absence of an IPC committee at the facility, cadre of HCWs and knowledge of IPC were significant predictors of IPC practices. The HCWs had adequate knowledge of IPC, but their knowledge gap was specifically on the implication of colour coding of bin liners for waste segregation. We recommend the institution of IPC committees in all healthcare facilities in the country. Also, policies and interventions to improve adherence to IPC practices should be context-specific, sustainable and aimed at addressing the knowledge gap including colour coding of bins among HCWs.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231225924 – Supplemental material for Health and safety of health workers in the Suame Municipality of Ghana – Lessons learnt from the COVID-19 outbreak in infection prevention and control for future pandemics
Supplemental material, sj-docx-1-smo-10.1177_20503121231225924 for Health and safety of health workers in the Suame Municipality of Ghana – Lessons learnt from the COVID-19 outbreak in infection prevention and control for future pandemics by David Oppong Darko, Douglas Aninng Opoku, Nana Kwame Ayisi-Boateng, Aliyu Mohammed, Jennifer Ashilevi, Obed Kwabena Offe Amponsah, Ayongo Mate-Kole, Dora Egblewogbe, Bridgetta Addai Darko, Ebenezer Agyemang and Paul Okyere in SAGE Open Medicine
Footnotes
Acknowledgements
We are grateful to the Suame Municipal Health Directorate and all the Management of the four health facilities that approved for this study to be conducted. We express our deepest gratitude to all study participants and research assistants.
Author’s contribution
DOD, DAO and PO conceptualised the study design. DOD, NKAB, AM, JO, BA, JA, AM-K, EA and OKOA collected the study data. DAO, DE, AM, JO and PO contributed to the data analysis and interpretation. DAO, DOD, BAD, AM, PO and JO drafted the manuscript. All the authors were involved in the manuscript revision. The final version of the manuscript was approved by all the authors for publication.
Data availability
The datasets used to analyse the present study will be made available upon request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.