
Abstract
Background:
Needlesticks and sharp injuries are occupational hazards for healthcare workers that result from the accidental piercing of the skin. Needlestick injuries expose healthcare workers to blood and body fluids that may be infected and can be transmitted to them. Healthcare workers have been exposed to blood-borne pathogens through contaminated needles and other sharp materials every day. Around 20 blood-borne diseases can be transmitted through casual needlesticks and sharp injuries.
Objective:
To assess needlestick and sharp injuries and its associated factors among healthcare workers in Southern Ethiopia, 2021.
Methods:
The hospital-based cross-sectional study design was conducted among 341 healthcare workers in Worabe Comprehensive Specialized Hospital from June 10 to July 6, 2021. A stratified sampling technique was used and data were collected using standardized structural questionnaires by BSc nursing professionals. The collected data were checked for completeness and consistency by the investigator. The completed questionnaire was given an identification number and entered into EpiData version 3.5.1. The data were coded and analyzed using SPSS version 26 using a binary logistic regression model and presented with texts, tables, and graphs.
Results:
The finding revealed that 30.6% of healthcare workers had experienced needlestick and sharp injuries within their working area. Healthcare workers not trained on safety measures of needlestick and sharp injury (adjusted odds ratio: 7.179 (3.494–14.749)), working in the delivery unit (adjusted odds ratio: 6.528 (3.171–11.834)), being older age (adjusted odds ratio: 3.394 (1.775–7.126)), working in inpatient unit (3.278 (1.804–5.231)), working in an emergency unit (adjusted odds ratio: 5.718 (4.326–6.398)), working in an operation room theater (adjusted odds ratio: 2.359 (1.781–4.430)), working as a medical laboratory technician (adjusted odds ratio: 1.070 (1.432–3.304)), working in pediatrics unit (adjusted odds ratio: 1.063 (1.431–2.843)), working as cleaners (adjusted odds ratio: 0.018 (0.002–0.195)), working <40 h per week (adjusted odds ratio: 0.036 (0.004–0.345)), and seldom needle recapping (adjusted odds ratio: 0.043 (0.015–0.125)) were statistically associated with needlestick and sharp injury.
Conclusions:
In this study, there is a high magnitude of needlestick or sharp injuries among healthcare workers. Lack of training on work-related safety measures; working in delivery; being older age; working in the inpatient unit, emergency, operation room, and pediatrics units; being laboratory technicians, and cleaners; working hours per week; and seldom needle recapping were significant predictors of needlestick and sharp injury.
Introduction
Needlestick and sharp injuries (NSSIs) are caused by sharp materials that accidentally puncture the skin with medical equipment that was used to screen, diagnose, treat, or follow a patient’s disease condition. 1 Needlesticks and sharps include hypodermic needles, blood collection needles, and IV (intravenous) cannulas or needles as well as items such as scalpels, blades, lancets, retractors, scissors, pins, clamps, cutters, staples, and glass items. 2
Healthcare facilities can provide diagnostic, preventive, curative, and prognostic services for the community. However, while they are providing services, healthcare workers (HCWs) are exposed to blood and body fluids through occupational sharps, splashes, and needlestick injuries. 3 Particularly, there is a potential exposure among doctors, nurses, laboratory professionals, and biomedical waste management staff to blood-borne pathogens worldwide. 4
NSSIs are the most common workplace-related health hazards responsible for the transmission of blood-borne pathogens among HCWs. 5 Occupational exposures to percutaneous injuries are a substantial source of infections with blood-borne pathogens among HCWs and can cause substantial health consequences and psychological stress for HCWs. 6
Needles and sharp objects cause accidental puncture of the skin. 3 The majority of injuries occur during surgical operations, blood sample collection, intravenous line administration, and negligent waste disposal practices. 7 More than 20 blood-borne infections can be transmitted through body fluids by NSSI. 8
Human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV) are the most prevalent illnesses that might possibly be transmitted through bodily fluids. 9 Following unintentional sharps injuries, there was a potential of contracting 30% HBV, 3% HCV, and 0.3% HIV. 10
Due to the high prevalence of blood-borne pathogens, the lack of basic personal protective equipment (PPE), poor adherence to safety procedures, and a decreased propensity to report and use postexposure prophylaxis HCWs are at risk of blood-borne pathogen infections through occupational exposure in developing countries.11,12
After exposure, the HCWs are affected in various ways including direct costs for laboratory tests, including tests for HBV serology, HIV antibodies, anti-HCV, and treatment for any conditions. There is also the burden associated with postexposure prophylaxis and its working units. 13
Generally, NSSI causes only minor bleeding or visible trauma on the surface of the skin and subcutaneous tissue. However, even in the absence of bleeding, the risk of developing viral infection remains positive. 14 It is important to study about NSSIs to prevent their occurrence and take adequate measures to avoid transmission of blood-borne pathogens related to it so that it can no longer pose a risk for HCWs. In settings with inadequate resources, there is a considerable risk of occupational transmission of blood-borne pathogens, and an increased risk of contracting a serious illness, which can be caused by bleeding, minor surface scrapes, and apparent skin injuries. 15
A review study conducted in the overall African region and Ethiopia revealed that 51% and 43.6%, respectively, of HCWs were exposed to NSSIs in the course of their careers.16,17 Also, studies revealed that the contributing factors for NSSI were job satisfaction, being cleaner, working in maternity, emergency unit, and lack of work experience and training.18,19 While in search of factors like the number of working hours per week, the type of instrument used, the shift time, the activity that caused the accident, the beginning of postexposure prophylaxis, and the application of postexposure antiseptic agent were neither statistically tested nor discovered in prior studies. But identifying these contributing factors is important for effective prevention of NSSI in HCWs.
So, this study was designed to fill these gaps and the finding of this result was used as an evidence-based practice for the healthcare community, and healthcare safety measures standards, policies, and guidelines at the national and international levels. Therefore, the study aimed to assess NSSIs among HCWs in Southern Ethiopia.
Methods and materials
Study design and setting
A cross-sectional study was carried out in Worebe Comprehensive Specialized Hospital (WCSH), Southern Ethiopia, which is located 172 km southwest of Addis Ababa, the capital city of Ethiopia. It is the primary hospital serving the Southern region, offering general and specialty care in the intensive care unit (ICU), medical specialty, surgery, gynecology, obstetrics, ENT (ear, nose, and throat), maxillofacial, plastic, and orthopedic healthcare service to around 10 million people from the surrounding region. The study was conducted from June 10 to July 6, 2021.
Sample size determination
The required sample size was calculated using single population proportion formula with the assumption of a 95% of confidence interval (CI) and a 5% of margin of error and the prevalence of NSSIs (28.3%) among HCWs in Dessie City Hospital, Northeast Ethiopia. 19

Where n = Sample size
(Z α/2)2 = Value corresponding to a 95% level of significance = 1.96
p = prevalence (28.3%) = 0.28
q = (1 − p) = (1 − 0.28) = 0.72
d = Margin of error assumed to be 5%

Considering a 10% nonresponse rate, the final sample size became 341.
Study participants and sampling procedures
All HCWs working in Worabe Comprehensive Specialized Hospital were the source of the population. Randomly selected HCWs working at the hospital who fulfilled the inclusion criteria were the study sample. All HCWs in WCSH who had needlestick injuries and were present at the time of data collection were included. Critically ill participants and those on annual leave were excluded from the study. In the sampling procedure, a stratified random sampling method was used. The study population (HCWs) was divided into subgroups or strata based on their professional characteristics and then from each subgroup participants were selected randomly using a lottery sampling technique (Figure 1).
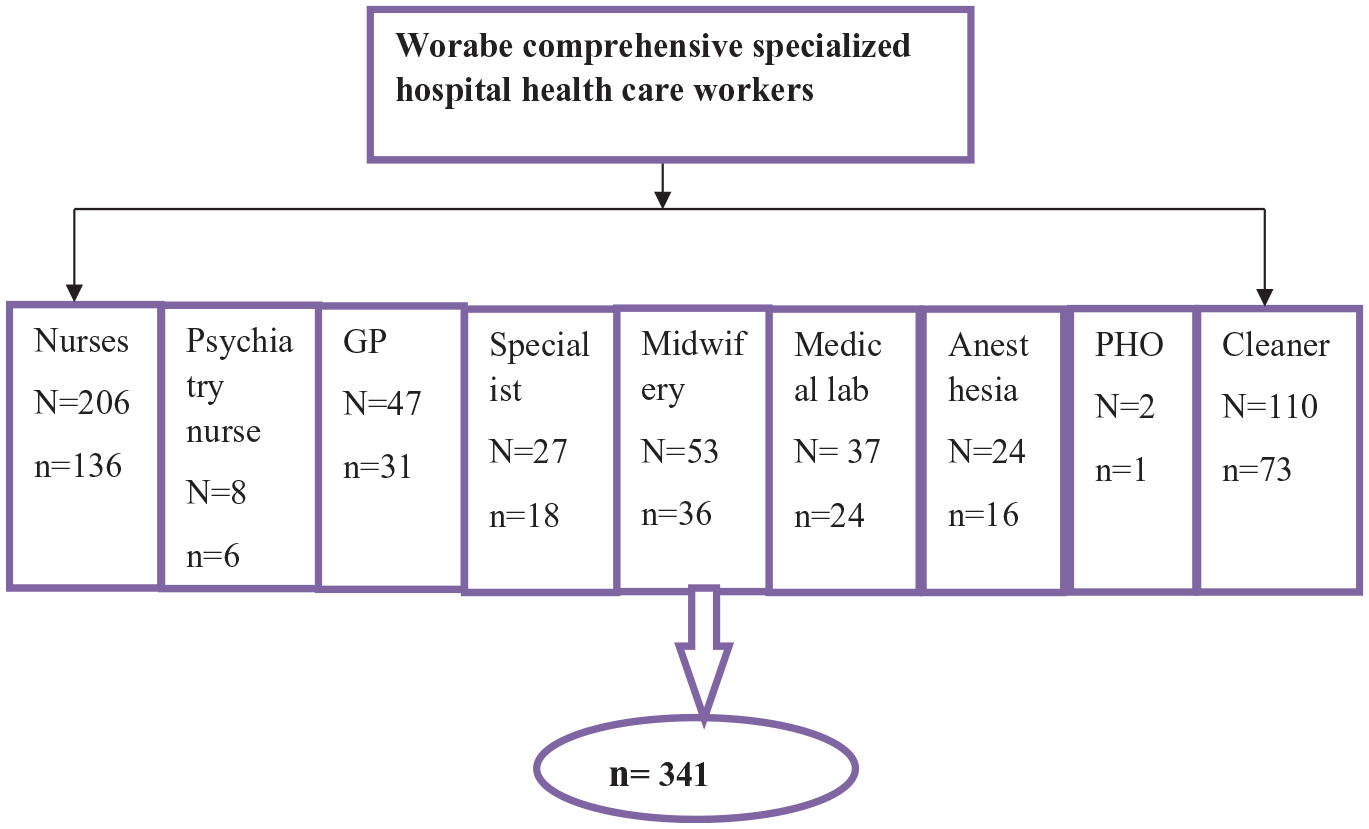
Schematic representation of sampling procure.
Study variables
The dependent variable was sharp and needlestick injury. The independent variables included sociodemographic (age, sex, educational level, job category, work experience), organizational (working hours, working department, training on safety measures and precaution, working unit), and behavioral factors (needle recapping, use of PPE, follow universal safety guidelines).
Operational definition
Needles stick sharp injuries
Injury caused by needles or any sharp materials that accidentally puncture the skin of HCWs in their working area during their entire career.
Healthcare workers
Participants working in the hospital have contact with syringes, needles, and other sharp materials due to their job.
Data collection instrument and quality control
A standardized structural questionnaire was used and the questionnaire was prepared in English language and translated into the national language, Amharic. The dependent variable component of the questionnaire contained NSSIs, which were defined as injuries caused by needles or other sharp objects accidentally puncturing the skin of healthcare personnel in their workplace over the course of their careers. The independent variables included sociodemographic characteristics, NSSI exposure-related factors, and knowledge of safety measure-related factors, They were adapted from similar studies conducted in Desse hospital 19 and Tikur Anbessa Specialized Hospitals. 1 Data were collected by three BSc graduating nurses and two supervisors following the overall data collection process from June 10 to July 6, 2021. The training was given to data collectors and supervisors for one day. A pretest was done on 5% of the study population in Butajira Hospital 1 week before starting data collection. Appropriate corrections and modifications in the area such as sentence context, grammar, and punctuation were made. The collected data were submitted to the principal investigators on time and were checked for completeness, consistency, and clarity.
Statistical analysis
Each questionnaire was carefully validated for its completeness after data were collected, coded, entered into EpiData version 3.1, and exported to SPSS version 26 for statistical analysis. A binary logistic regression analysis was used to determine associated factors with the dependent variable, sharp and needlestick injuries. The relationship was determined by odds ratio and p-value with a 95% CI. An explanatory variable with a p-value ⩽0.2 in the bi-variable logistic regression analysis was entered into a multivariable logistic regression analysis to control possible confounders, which is a third variable that influences both the independent and dependent variables. p-Value < 0.05 was used to declare the level of statistical significance and an adjusted odds ratio (AOR) with 95% CI was used to estimate the significant level of variables. Finally, the results were presented in texts, tables, and graphs based on the types of data.
Ethics consideration
Ethical approval for the study was obtained from Wolkite University, College of Medicine and Health Science, Institutional Review Board (IRB) with ethical approval number RCSUILC/14/2021. Verbal informed consent was obtained from each study participant; however, trial registration is not applicable and it is not necessary to get written informed consent. The IRB waived this requirement for this investigation.
Results
Sociodemographic characteristics
From the total sample size, 340 respondents participated with a response rate of 99.7%. Of those participants, 174 (51.2%) were females. Regarding the age of the participants, the mean age was 29.8 years with a ±5 standard deviation. In marital status, 207 (60.9%) study participants were married, concerning educational status, 213 (62.6%) were degree holders, and 136 (40.0%) of participants were nurses. And one-third of the study participants had >40 working hours per week, 198 (58.2%). Regarding working experience, 298 (87.6%) participants had work experience of lesser than 5 years, and 42 (12.4%) had work experience of 5–10 years (Table 1).
Sociodemographic characteristics of a study on NSSI among HCWs working in Southern Ethiopia, 2021.
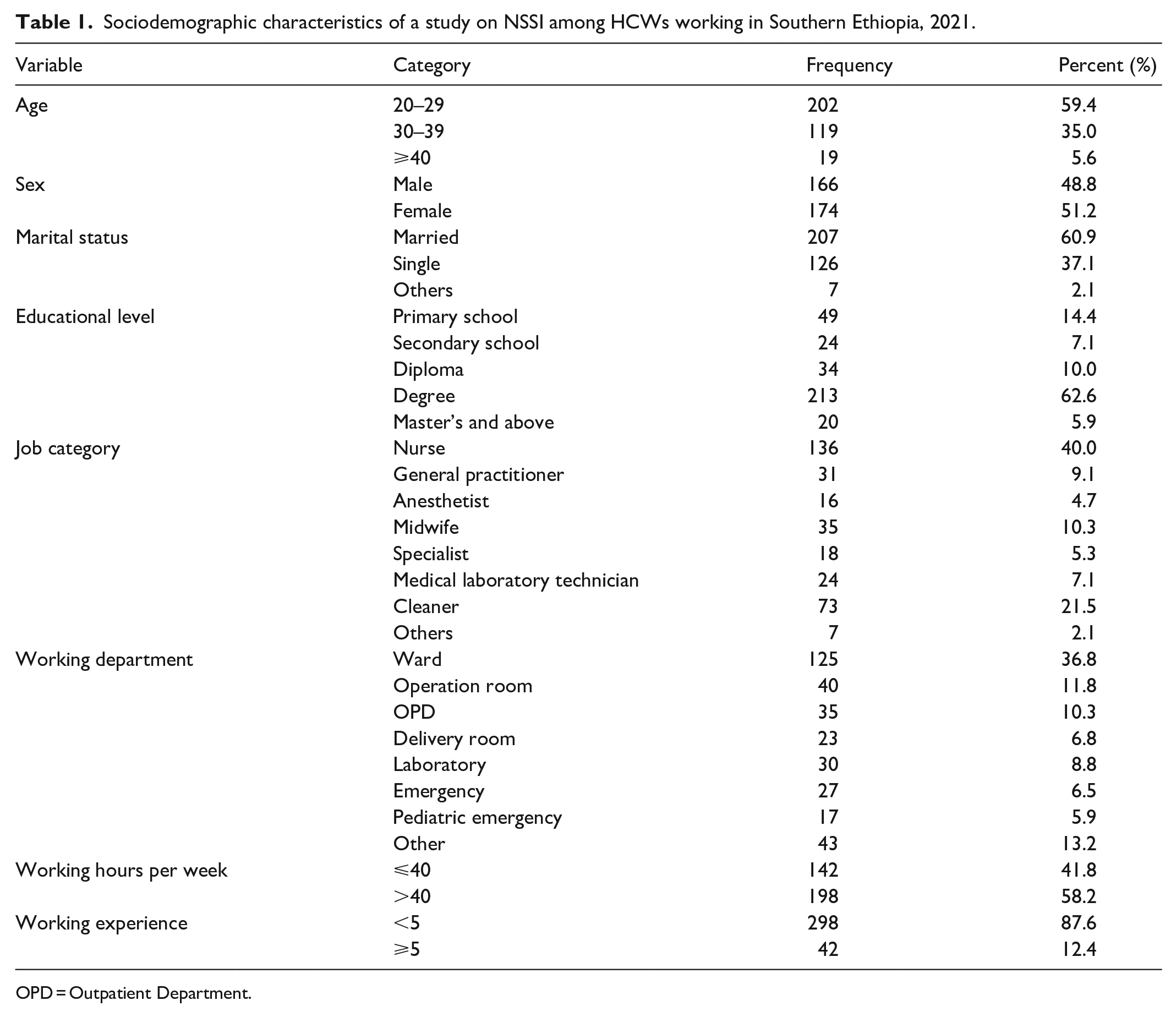
OPD = Outpatient Department.
Needlestick and sharp injuries
Of a total of 340 HCWs, 104 (30.6%) faced NSSIs in their working area (95% CI (25.67–35.51)). Around 87 (25.6%) of the HCWs experienced injury 2 to 4 times in their working environment. Regarding the depth of the injury, 61 (17.9%) were superficial and 39 (11.5%) were moderate. Needle hollow bore was the major cause of injury in 65 (19.1%) and 29 (8.5%) injuries occurred during recapping, 72 (21.2%) of the instruments were used and 15 (4.4%) of the instruments had blood on it. Ninety-three (27.4%) injuries occurred during daytime and 125 (36.7%) of the injury occurred inwards. Of the injured participants, 95 (27.9%) washed the injury site with soap and water. Of 104 (30.6%) HCWs who experienced the injury, only 29 (8.5%) of them reported their injury (Table 2).
The magnitude of NSSI exposure of health workers working in WCSH, Worabe, Ethiopia, 2021.

OPD = Outpatient Department.
Safety measures taken by HCWs
Among the study participants, 41.8% recap the needle, 16.8% always recap needles, and 25.0% of the participants seldom recap needles. From the study participants, 177 (52.1%) did not receive the full dose of the hepatitis vaccine and 230 (67.6%)were trained on the safe practice of NSSI (Table 3).
Awareness of safety measures among HCWs working in Southern Ethiopia, 2021.

NSSI = Needlestick and sharp injury.
Factors associated with NSSI
In bi-variable analysis, the variables were age, sex, marital status, educational status, job category, working department, shifting time, the reason for the accident report, time of accident happening, receiving a full dose of hepatitis vaccine, working hours, needle recapping, visible blood before the accident, and HCWs not trained on needlestick injury and safety measure were statistically significant variables. In multivariable analysis, variables being aged, medical laboratory, cleaner, working environment in a ward, emergency and operation room, long contact working hours, needle recapping, and HCWs not trained on needlestick injury and safety measures were significantly associated with NSSI.
Older HCWs were three times more likely to have NSSIs than those who were young (AOR: 3.394 (1.775–7.126)). A medical laboratory technician was more likely (AOR: 1.070 (1.432–3.304)) to have NSSI than a cleaner (AOR: 0.018 (0.002–0.195)). Healthcare providers working in a ward (3.278 (1.804–5.231)) three times, working in the operation room (AOR: 2.359 (1.781–4.430)) 2.4 times, and working in the delivery unit. Working in the emergency unit (AOR: 5.718 (4.326–6.398)) and in the pediatrics unit (AOR: 1.063 (1.431–2.843)) were likely to have 5.7 times and 1.1 times more NSSI, respectively. But working in the laboratory unit (AOR: 0.897 (0.020–0.238)) was less likely to have NSSI. HCWs working more than 40 h per week were less likely to have NSSI than those working less than 40 h per week (AOR: 0.036 (0.004–0.345)). Seldom needle recapping (AOR: 0.043 (0.015–0.125)) and always needle recapping (AOR: 0.273 (0.108–0.687)) were less likely to have needlestick injury compared to the HCWs who never recapped needle. HCWs not trained on safety measures for sharp and needlestick injury (AOR: 7.179 (3.494–14.749)) were seven times more likely to have sharp and needlestick injuries than those who have been trained (Table 4).
Shows bivariate and multivariate logistic regression analysis of sharp and needlestick injury among HCWs working in Southern Ethiopia, 2021.

Indicates significant variables in multivariable analysis.
NSSI = Needlestick and Sharp Injury; COR = Crude Odds Ratio; AOR = Adjusted Odds Ratio; OPD = Outpatient Department.
Discussion
NSSIs are the most common workplace-related health hazards responsible for the transmission of bloodborne pathogens in HCWs. 5 This study aimed to assess NSSI among HCWs working in Southern Ethiopia. This study’s result showed that about 104 (30.6%) HCWs encountered sharp and needlestick injuries, which is in line with (95% CI; 26.8–34.4). This study’s result is higher than the incidence reported in Saudi Arabia (22.2%), 20 percutaneous injuries in Kenya (19%), 2 and Awi Zone (18.7%). 21 The difference might be due to the design of the study as their study includes a 1-year magnitude whereas this study includes a month of working time magnitude. This finding is lower than the ones reported from Iran (45.5%), 22 a systematic review and meta-analysis at the global, regional, and national levels (43%), 16 Dessie (60.2%), 19 Dire Dawa (52.8%), 23 Tigray (38.5%), 24 Bale Zone (37.1%), 25 and Hawassa city (35.8%) 23 in their working area. The variation might be due to Sociodemographic characteristic of the study participants, their work experience, or the study period now advanced health facilities are available compared to the past few years.
Being an older age HCW was three times significantly associated with NSSI. This result was consistent with the study conducted in, 20 Tanzania, 8 and Kenya. 2 The reason might be increasing chronological age-related structural and functional change in the loss of muscle strength and sensory nerve ending, loss of concentration, attention, and other body organ changes in older care providers. Being a laboratory technician was positively associated with NSSI. This is consistent with the report from Saudi Arabia 26 and Dire Dawa, Eastern Ethiopia. 23 This may be due to the fact that those workers were exposed to sharp materials in their working environment. While being a cleaner is negatively associated with having a NSSI relative to being a nurse. There were no similar studies related to this result. The cleaners use hard and strong PPE such as rubber gloves and boots shoes. It could be the reason for this negative association.
Healthcare providers working in the inpatient unit were three times significantly associated with NSSI; there were no similar studies reported as such. This is because care providers stayed for a prolonged time in the ward, which may increase the chance of frequent exposure of needles and sharp materials. Care providers working in the operation room were more than two times statistically associated with NSSI, which is the same as reported in South Africa. 27 The reason might be the presence of various sharp materials in the operation room. Working in the delivery unit six times, working in the emergency unit almost six times, and pediatrics unit more than one time more likely to have NSSI, while working in the laboratory unit was less likely to have NSSI. This mimicked the study finding from Bahir Dar, Northwest Ethiopia. 18 This might be because the working units were in a risk environment for NSSI, the station was overcrowded with patients, and there were poor equipment and material station in the unit may.
HCWs working more than 40 h per week were less likely to have NSSIs than those working less than 40 h per week. This was consistent with the study done in Iran 28 ; Tigray, Northern Ethiopia 24 ; and Dire Dawa, Eastern Ethiopia. 23 This might be due to the fact that direct increasing working hours might have increased their work experience and awareness of safety measures, which in turn reduced the incidences of sharp and needlestick injury.
Needle recapping was less likely to have needlestick injury relative to the HCWs who never recapped needles. A similar finding was reported from Dessie City Hospitals, North Ethiopia 19 ; Tigray Region, Ethiopia 24 ; Dire Dawa, Eastern Ethiopia 23 ; and Nekemte, Western Ethiopia. 25 Also in this study, 36.8% of healthcare professionals never recapped needles after use, which is lower than a study reported from Taiwan increasing from 47% to 85% of participants who never recapped needles after use in their working environment. 29 The reason may be a direct shuffling of the dry needlestick by needle cap and properly disposing of the safety box.
HCWs not trained on safety measures for NSSI were seven times more likely to have sharp and needlestick injuries than those who have been trained. The report was similar to the study reported from Kenya 2 ; Dessie City Hospitals, Northern Ethiopia 19 ; Tigray, Northern Ethiopia 24 ; and Nekemte, Western Ethiopia 25 The reason may be that those who had taken the training had a better awareness of standard precautions to be taken on the prevention of needlestick injury and its safety measure.
Strength and limitation
Strength
The report had a high response rate and the inclusive nature of this research incorporate all HCWs who have direct contact with NSSIs and was not specific to one or two professionals’ occupational exposures.
Limitation
The study did not address the qualitative section using observational checklists. The study was a cross-sectional study design that cannot establish cause and effect relationships and recall bias due to the retrospective nature of questions concerning the risks or accuracy of the experience of the respondents concerning the occurrence of the NSSI might have been affected by recall bias.
Conclusion and recommendation
Conclusion
There is a high magnitude of NSSIs among HCWs in their working area and a lack of training on work-related safety measures, working in delivery, being older age, working in inpatient units, emergency, operation room, and pediatrics units, being laboratory technicians, cleaners, contact working hours and seldom needle recapping were significant predictors of NSSI.
Recommendation
Policymakers should provide formal continuous professional development training on the safe practice of needlesticks and sharps and continuous monitoring of workplace safety should be ensured to reduce the NSSIs.
The ministry of health should ensure the presence of the required manpower available in their working area. It can reduce working hours or staff work overload and also reduce occupational exposure to NSSI.
The institution should also have access to an adequate supply of PPE for high-risk working environments such as delivery units, emergency, operation room theater (ORT), and ICU rooms and should also ensure the availability of postexposure prophylaxis medicines in the organizations.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221149536 – Supplemental material for Needlestick and sharp injuries and its associated factors among healthcare workers in Southern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221149536 for Needlestick and sharp injuries and its associated factors among healthcare workers in Southern Ethiopia by Baye Tsegaye Amlak, Shegaw Tesfa, Betelhem Tesfamichael, Haimanot Abebe, Bitew Tefera Zewudie, Agerie Aynalem Mewahegn, Bogale Chekole Temere, Tamene Fetene Terefe, Fisha Alebel GebreEyesus, Tadesse Tsehay and Mamo Solomon in SAGE Open Medicine
Footnotes
Acknowledgements
Firstly, we would like to thank Wolkite University, the College of Medicine and Health Science, and the Department of Nursing for providing the opportunity to learn and develop this research article. Next, we would like to express our sincere gratitude to the hospital managers for allowing us to conduct this study in their respective health institutions and to study participants for their willingness to participate.
Author contributions
ST, BTA, and TT: Draft the proposal, lead the data collection, and analysis process, wrote the final thesis, and prepare the manuscript, HA, BC, AA, and BT: Revise and edit proposal and thesis, support data collection and analysis, revise thesis manuscript, MS, TF, FA, and BTZ: reviewed different works of literature, revised proposal, and thesis manuscript. All authors revised, consented, and approved the final version of the thesis and manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for the study was obtained from Wolkite University, College of Medicine and Health Science, Institutional Review Board (IRB) with ethical approval number RCSUILC/14/2021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from each study participant, however, trial registration is not applicable and it is not necessary to get written informed consent, and the Institutional Review Board waived this requirement for this investigation.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.