
Abstract
Background:
The mental burden faced by university students in their early years is not frequently reported in the literature.
Objectives:
The aim of this study is to investigate the prevalence and predictors of depression among preparatory (first) year university students using a predictive test developed from general health and well-being questionnaires.
Methods:
A cross-sectional study was conducted among university students in the eastern region of Saudi Arabia from March 2023 to June 2023. A self-administered electronic general health and well-being questionnaire was implemented. Written informed consent was obtained from the participants after explaining the study’s purposes. The questionnaire consisted of three parts. Part I described the objective of the study and maintained the confidentiality of the data, part II contained questions about demographic data, and part III contained the scales of the items to assess the physical and psychological health.
Results:
The findings demonstrated a significant positive correlation between depressive symptoms and both perceived stress (r = 0.444, p < 0.01) and perceived burdens (r = 0.735, p < 0.01). In addition, there were significant negative correlations between the depressive symptoms and gender (r = −0.144, p < 0.05), economic level (r = −0.178, p < 0.05), and social support (r = −0.312, p < 0.01). Furthermore, the results revealed that body mass index (b = 0.272, t(146) = 4.636, p < .001), perceived stress (b = 0.182, t(146) = 2.910, p < 0.01), and perceived burdens (b = 0.593, t(146) = 9.507, p < .001) were significant predictors of depressive symptoms among Saudi university junior students.
Conclusion:
Our findings emphasize the need for tailored mental health support services to address depression and its predictors, especially during critical transition periods like the early stages of university life, as early detection and intervention can lead to improved management and better control of the depression.
Introduction
The mental challenges faced by university students, particularly during critical transitions like the early stages of university life, are rarely reported in the literature. 1 Aside from education, other important parts of being a student might include moving away from parents, dealing with money issues, housing, and interacting socially with students. Students’ coping strategies, social support, and adaptability may determine how much of an impact these changes have on them. 2 These perceived burdens have an effect on mental health. There is typically a correlation between perceived burden and depressive symptoms. 3 But it is still unclear if perceived burden completely explains its impact on depression.
University education requires time and effort, and it is not always easy. University students are expected to be skillful and competent in order to work safely with patients after graduation. As a result, many students may find university a difficult, demanding, and stressful learning process. 4 According to the available evidence, university-age students are more likely to experience mental health issues, such as depression and anxiety, due to the perceived overwhelming and stressful nature of the university environment. 5
An increasing number of studies highlight depression as a significant health concern for university students, with research suggesting that around one-third of students show symptoms of depression. Additionally, depression rates among university students can be as high as 85%, varying based on the specific population and the assessment methods applied. 6
Several factors have been identified as potential predictors of depression among university students, including academic stress, social support, financial difficulties, and personal history of mental health issues. 7 Understanding these predictors is crucial for developing effective prevention and intervention strategies.
Physical health has been shown to affect mental health and vice versa. 8 A prior reports at Imam Abdulrahman Bin Faisal University, Saudi Arabia found low engagement in extracurricular activities among college students.9,10 This low participation rate could potentially be a significant risk factor for students’ mental well-being.
Prior studies have reported high levels of overweight among Saudi university students,11,12 which may exacerbate the problem of depression. Research has established a significant link between body weight and mood disorders. A meta-analysis and systematic review have demonstrated that being overweight increases the risk of developing depression. 13
While depression has been studied among Saudi university students, previous research has primarily focused on specific cohorts, such as medical 14 or nursing 15 students, particular genders, 16 postgraduate students, 17 or during the COVID-19 pandemic. 18 However, little attention has been paid to depression risk factors, especially among students in their early stages of university education, particularly at our institution. This gap in knowledge underscores the need for further investigation to predict the most likely risk factors for depression in early university life in this local setting.
This study hypothesizes that elevated levels of perceived stress are correlated with a higher prevalence of depressive symptoms among university students. Additionally, it posits that greater social support is associated with reduced levels of depressive symptoms. Furthermore, it is anticipated that students from lower economic backgrounds will exhibit higher levels of depressive symptoms compared to their peers from more affluent backgrounds. Thus, the aim of the current study was to investigate the prevalence and predictors of depression among university students in preparatory (first) year, Saudi Arabia, eastern region, using a predictive test developed from general health and well-being questionnaires.
Methodology
Study design and data collection
A cross-sectional study was conducted among university students in the eastern region of Saudi Arabia during the period March 2023 to June 2023. A self-administered electronic questionnaire in preparatory year at Imam Abdulrahman Bin Faisal University was issued to students with courses that were randomly selected.
The study utilized a convenience sampling method to recruit participants. The survey instrument was distributed to a pool of 1000 students currently enrolled in the preparatory health path program at Imam Abdulrahman Bin Faisal University. This sampling approach was chosen due to the accessibility and proximity of the target population to the researchers, as well as the relevance of these students to the study’s objectives.
Inclusion criteria were the following: being a university junior student, aged ⩾ 18 years old, and enrolled full-time at the university. Students were excluded from the study if they were currently receiving mental health treatment, had a diagnosis of any psychological conditions, were not first-year students, and had severe medical conditions.
This research will uphold the rights and welfare of all participants, in line with the principles outlined in the Declaration of Helsinki. An ethical approval was obtained prior to the study (IRB-2023-19-108) by the institutional review board at Imam Abdulrahman Bin Faisal University.
The current research utilized a predictive test that was developed from general health and well-being questionnaires. However, the research utilized the questionnaire that had been previously validated in Arabic language. 19
The questionnaire consisted of three parts. Part I described the objective of the study and maintained the confidentiality of the data in addition to indicating that the participation in the questionnaire was voluntary, and the answers to the questions were anonymous. Participants were required to acknowledge this information by clicking “next,” before proceeding to the subsequent parts of the questionnaire. Part II contained questions about demographic data, such as gender, age, social status, economic level, residence, and year of study. Part III contained the scales of the items.
Two items in the body mass index (BMI)
BMI was calculated using the reported data through applying a metric formula (BMI = (weight in kilogram (kg)/height in meter m2)). The calculated BMI categorized into underweight (BMI < 18.5), normal (18.5 ⩽ BMI ⩽ 24.9), and overweight (BMI ⩾ 25.0). 20
22 Items in the health problems, strains, and psychosomatic symptoms
The study evaluated 22 symptoms that assessed various student health issues, based on previous research. The symptoms included sleep insomnia/disorder, concentration difficulties, dizziness, stomach heartburn/trouble, depressive mood, rapid heartbeats, headaches, concentration issues, neck, and shoulder pain. Participants were asked to rate their experiences over the past year using a four-point scale (1 = never; 4 = very often). Responses categorized as “sometimes” and “very often” were combined into a single group for analysis purposes. 21
19 Items in the depressive symptoms
Depression was assessed through a modification of the Beck Depression Inventory (M-BDI 20 items). 22 We adapted the M-BDI version as it has been shown to effectively capture depression symptoms in similar cohorts and validated in similar contexts. 23 Importantly, the internal consistency of the 20-item M-BDI was found to be high across four different countries (Denmark, Germany, Bulgaria, and Poland), with Cronbach’s alpha values ranging from 0.87 to 0.92. Overall, the translated versions of the M-BDI exhibited good configural and metric measurement invariance for the samples studied, supporting the validity of cross-national comparisons. 23
In the present study, the authors of the M-BDI excluded the item “I lost interest in sex” in their survey due to cultural sensitivities in a Muslim-majority country. They have established the validity of the M-BDI's construct and its measurement equivalence to the original BDI. This indicates that the M-BDI can accurately measure depression in a culturally sensitive manner, ensuring that the results are comparable to those obtained using the original BDI. The sum of the 19 items of the M-BDI was 7–35 points. All depressive symptoms were divided into two binary categories (low ⩽ 4th quintile and high > 5th quintile).
Eight items in the body image concern
This part gauges the degree of concern regarding body shape over the last 4 weeks on a six-point Likert scale ranging from 1 (“Never”) to 6 (“Always”). Scores on this scale range from 8 to 48 points. 24
One item in the general health
The survey investigated students’ general health, which was based on a question from The American College Health Association. Participants were asked to rate their current general health by answering the question “How would you describe your general health?” with a five-point response scale ranging from “1 = excellent” to “5 = poor.” The responses were then recategorized into three categories for analysis purposes. This allowed for a more straightforward interpretation of the results and provided a broader understanding of the students’ general health. 25
Four items in the perceived stress
Perceived stress was assessed using the four items Perceived Stress Scale (PSS-4) with each item rated on a five-point Likert scale. The PSS-4 was selected for its brevity and suitability for measuring perceived stress and mental health in a variety of populations, including those similar to our study sample. While the original PSS is longer, the PSS-4 has been shown to retain strong psychometric properties while minimizing respondent burden. The total PSS score was computed and subsequently reclassified for the present study by splitting it at the median into two subgroups: “low” (⩽median) and “high” (>median). 26
One item in the self-assessed health
Self-assessed health involved the query “How do you assess your overall health?” with responses on a five-point scale. In this study, we recategorized it into two subgroups: “Higher” perceived health (“Excellent” and “Very good”); and “Lower” perceived health (“Good”, “Fair”, and “Poor”). 27
Two items in the social support and satisfaction
Social aspect was assessed using a modified version of Sarason’s Social Support Questionnaire. Participants were asked two questions: “How many people do you know including your family and friends support you whenever you feel down?” The numerical responses were categorized into “low” (1 person), “medium” (2–3 persons), or “high” (>3 persons) social support. Satisfaction with social support was evaluated with the question: “Are you on the whole satisfied with the support you get in such situations?” Responses were recorded on a five-point Likert scale ranging from “very satisfied” (1) to “very dissatisfied” (5), which were later grouped into three categories. 28
One item in the economic-related stress
Economic-related stress was evaluated through a question asking participants on a six-point Likert scale ranging from “not at all” (1 point) to “very strongly” (6 points) about the extent of the burden they felt in the area of finance. A binary variable was created by grouping the lower rating into “lower” and the higher rating categories into “higher.” 29
18 items in the perceived burdens/life stressors
The evaluation of perceived burdens and life stressors involves the examination of various stressors that students experience, such as academic demands, exams, relationships with peers and parents, feelings of isolation, financial concerns, and future expectations. Participants were asked to rate their level of agreement with each statement on a six-point scale, ranging from “not at all” to “very strongly.” The responses were then recategorized into two categories for further analysis. This approach allowed for a more straightforward interpretation of the results and provided a broader understanding of the stressors that students face. 30
The statistical analysis
We employed SPSS version 28 (IBM Corp., Armonk, NY, USA) to estimate descriptive statistics, examine the normality of variable distributions, and conduct Pearson correlation analysis. We cleaned the data and excluded uncompleted responses. In addition, multiple regression was applied to study the effect of predictor variables on depressive symptoms, and the results were presented as standardized coefficient β, and adjusted R2 with p set at less than 0.05.
Results
Baseline characteristics of the participants are summarized in Table 1. A sample size of 146 (14.6%) participants was obtained from a university preparatory student of 1000. A post hoc power analysis was conducted using G*Power to assess the adequacy of this sample Assuming a medium effect size (0.3) and an alpha level of 0.05, the achieved power was 0.99 for a one-sample proportion test. This indicates that the study had a 99% chance of detecting a medium-sized effect if one existed in the population, which exceeds the conventional threshold of 80% power. The margin of error for this sample size was calculated to be approximately 7.1% at a 95% confidence level. 31
Demographic data of the sample.

SR: Saudi riyal; SD: standard deviation.
Most of the participants were females (81), single (137) on average (18.2.8 ± 2.1 years old), and overly good economic level (1067.4 ± 25 Saudi Riyal).
We computed the descriptive statistics for the depressive symptoms to ensure their normality as one of the prerequisites for using regression analysis. Furthermore, we estimated the Pearson correlation coefficient between the variables as a prerequisite to regression analysis and to investigate the multicollinearity. Table 2 shows the variables correlation matrix of the variables. Our results revealed a significant positive correlation between depressive symptoms and both perceived stress (r = 0.444, p < 0.01) and perceived burdens (r = 0.735, p < 0.01). The study also detected significant negative correlations between the depressive symptoms and gender (r = −0.144, p < 0.05), economic level (r = −0.178, p < 0.05), and social support (r = −0.312, p < 0.01). However, there were few significant correlations between the independent variables, which ranged from weak to medium correlations.
Correlation matrix of all the study variables with depressive symptoms.
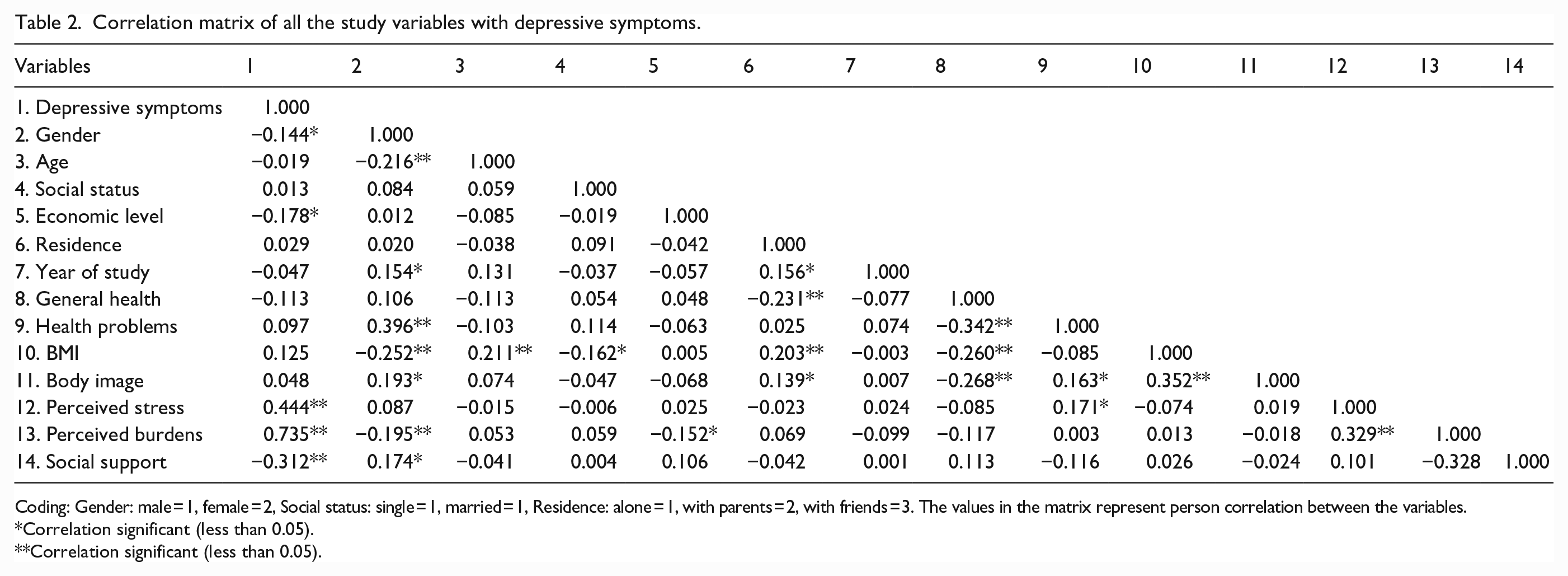
Coding: Gender: male = 1, female = 2, Social status: single = 1, married = 1, Residence: alone = 1, with parents = 2, with friends = 3. The values in the matrix represent person correlation between the variables.
Correlation significant (less than 0.05).
Correlation significant (less than 0.05).
A multiple regression test was conducted to examine the effect of gender, age, social status, economic level, residence, general health, health problems, BMI, body image, perceived stress, perceived burdens, and social support on the depressive symptoms. The overall model was significant (F (13, 132) = 18.350, p < 0.001) and accounted for 60.9% of the variance in the depressive symptoms (adjusted R2 = 0.609). The results revealed that both perceived stress and BMI were a significant predictor of the depressive symptoms, (b = 0.182, t(146) = 2.910, p < .01 and b = 0.272, t(146) = 4.636, p < 0.001 respectively). This suggests that individuals who report higher levels of stress are more likely to experience depressive symptoms.
In addition, perceived burdens were a significant predictor of depressive symptoms, b = 0.593, t(146) = 9.507, p < 0.001. Furthermore, social support was also a significant predictor of the depressive symptoms, b = −0.139, t(146) = 2.357, p < 0.05. On the other hand, age, social status, economic level, residence, year of study, general health, health problems, or body image were a nonsignificant predictor of the depressive symptoms, as presented in Table 3.
Key predictors of depressive symptoms in the study sample.

Discussion
The main finding of the present study demonstrated a significant positive correlation between depressive symptoms and both perceived stress and perceived burdens. In addition, there were significant negative correlations between the depressive symptoms with female (coded 2) gender, economic level, and social support. Furthermore, the results revealed that BMI, perceived stress, and perceived burdens were significant predictors of depressive symptoms among Saudi university students.
The significant occurrence of depression noted in this research might be attributed to numerous stressors associated with education, along with the regular stressors of daily academic life including academic pressure, career concerns, and financial struggles, or even health issues affect students. 32
Our findings on the significant positive correlation between depressive symptoms with both perceived stress and burdens among students in Saudi Arabia align with existing research in the field of mental health. Numerous studies have highlighted the complex relationship between depressive symptoms, stress, and burdens, emphasizing their impact on mental well-being. 11
By identifying specific stress domains that are significantly associated with depression, this research complements the study’s focus on perceived stress and perceived burdens, providing a more nuanced understanding of the factors contributing to depressive symptoms.
The research findings demonstrated a significant negative correlation between depression with female gender, economic level, and social support align with existing research in the field of mental health. 33 Several studies have explored the complex interplay between these variables, shedding light on how gender, economic factors, and social support can influence depressive symptoms. 19
In Saudi Arabia, the prevalence of depression in university age students based on gender is controversial. 20 A prior report documented a very high prevalence rate of depressive symptoms among male students range from 30.95% to 44.4%. 21
Male gender in Saudi Arabia is more prone to depression due to various factors highlighted in the research studies. While depression is generally more prevalent among females worldwide, the situation in Saudi Arabia shows a different trend. Research indicates that females in Saudi Arabia are more likely to experience anxiety and stress, but males are more prone to depression. Factors contributing to this include sociodemographic characteristics such as employment status, marital status, physical activity, and education level. 34 For example, males with lower education levels and unemployment are at higher risk of depression.
Additionally, the study findings suggest that depression levels increase with age, with older males showing higher mean depression scores. These factors collectively contribute to the increased vulnerability of males in Saudi Arabia to depression compared to females. 22 Moreover, the study delves into the gender differences in social support, noting that female students more likely to receiving higher levels of social support compared to male students. This gender variation in social support levels may influence how female individuals cope with stressors and utilize support networks, ultimately affecting their mental health outcomes. 21
The research findings suggest that social support can serve as a strong indicator of the psychological domain, indicating a negative correlation between depression and social support. Consistent with the present results, a prior report demonstrated that social support is important for university students against depressive symptoms. 23
While the specific mechanisms by which positive social support influences mental health outcomes are not fully understood, 24 it is generally believed to operate through two distinct mechanisms. First, it may mitigate the negative impacts of financial or emotional stress, known as the “buffering effect model,” by providing a protective layer against adverse effects. Alternatively, social support can directly influence mental health by meeting an individual’s fundamental needs for affection, social recognition, respect, or nurturance, regardless of their stress levels. 25
In the line of our findings, a high level of economic level is correlated with lower prevalence of the depression in previous studies. 24 In contrast, low economic resources can correlate with social stigma, stress, and feelings of hopelessness and helplessness, increasing the likelihood of social exclusion and marginalization. Nevertheless, these negative effects can be offset by the presence of positive social support. 26
Our results ran counter to existing evidence suggesting the association between body image concerns and depressive symptoms. 27 Previous research, however, emphasized the role of gender differences in this association. For instance, several studies reported that young females have more negative body image, higher susceptibility to eating disorders, and are more vulnerable to depression. 28 Accordingly, future replications should examine whether the relationship between body image and depression is contingent upon students’ gender through moderation analysis.
Furthermore, the results indicated that BMI was significantly predicted depressive symptoms when other variables were considered in the regression model. In agreement with the present results, BMI has been recognized as a predictor of depression among individuals in Saudi Arabia. Previous research has shown a positive association between BMI and depression scores, indicating that individuals with higher BMI levels at greater risk of experiencing depression. 29
Several mechanisms and complex factors that are believed to play a role in the development of depression in obese patients include inflammatory signaling, hypothalamic-pituitary-adrenal axis dysregulation, metabolic abnormalities from dysfunctional adipose tissue, alterations in insulin, glucocorticoids, and adipose-derived hormones. 7
Early detection and intervention among students can significantly reduce the progression of depression. By implementing programs like the Penn Resiliency Program, Resourceful Adolescent Program, and Happy Lessons, which focus on cognitive-behavioral skills and well-being promotion, schools can effectively prevent or mitigate the onset of depression in young individuals. These interventions not only equip students with coping mechanisms but also create a supportive environment that fosters mental wellness and resilience.
Conclusion
In conclusion, our study offers novel insights into the complex interplay of factors contributing to depression among university students. By identifying specific predictors and critical time periods for intervention, we extend beyond previous research to provide a more nuanced understanding of mental health challenges in this population. Our findings underscore the urgent need for tailored timely mental health resources and support services that address depression and its predictors, particularly during the pivotal early stages of university life.
Limitations
While this study may offer insights into the predictive factors of depression among preparatory Saudi university junior students, it is not without limitations. First, the generalizability of the findings could be limited due to the sample being small and situated in a single university. Future studies are, therefore, advised to recruit larger samples from an extended range of universities in Saudi Arabia. Second, the findings could be contaminated by response bias due to the use of self-reported tools. Methodological considerations must be made in future research to minimize self-report bias. Finally, given the cross-sectional nature of the data, the temporal precedence of the main variables could not be confirmed. Further, longitudinal studies are needed to track and analyze the development and progression of mental health issues among university students throughout their academic careers.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241310912 – Supplemental material for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students
Supplemental material, sj-docx-1-smo-10.1177_20503121241310912 for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students by Said El-Ashker, Abdulmajeed Alharbi, Somaya Mahmoud, Feras Al-Awad, Ahlam Alghamdi, Nouf Alaqeel and Mohammed Al-Hariri in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241310912 – Supplemental material for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students
Supplemental material, sj-docx-2-smo-10.1177_20503121241310912 for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students by Said El-Ashker, Abdulmajeed Alharbi, Somaya Mahmoud, Feras Al-Awad, Ahlam Alghamdi, Nouf Alaqeel and Mohammed Al-Hariri in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241310912 – Supplemental material for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students
Supplemental material, sj-docx-3-smo-10.1177_20503121241310912 for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students by Said El-Ashker, Abdulmajeed Alharbi, Somaya Mahmoud, Feras Al-Awad, Ahlam Alghamdi, Nouf Alaqeel and Mohammed Al-Hariri in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121241310912 – Supplemental material for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students
Supplemental material, sj-docx-4-smo-10.1177_20503121241310912 for Unraveling the threads of depressive symptoms: Enhancing predictions of depression among university junior students by Said El-Ashker, Abdulmajeed Alharbi, Somaya Mahmoud, Feras Al-Awad, Ahlam Alghamdi, Nouf Alaqeel and Mohammed Al-Hariri in SAGE Open Medicine
Footnotes
Acknowledgements
The authors wish to convey their heartfelt appreciation to the Deanship of Preparatory Year at Imam Abdulrahman Bin Faisal University for their exceptional support. The assistance and encouragement provided have been crucial to the successful completion of this project.
Author contributions
Conceptualization: Said El-Ashker. Resources: Nouf Alaqeel. Data curation and validation: Abdulmajeed Alharbi, Said El-Ashker, and Ahlam Alghamdi. Revising the manuscript: Feras Al-Awad and Nouf Alaqeel. Writing—original draft, review and editing: Mohammed Al-Hariri. Supervision and project administration: Mohammed Al-Hariri. All authors have read and agreed to the published version of the manuscript.
Availability of supporting data
Data are available on request from the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
An ethical approval was obtained prior to the study (IRB-2023-19-108) by the institutional review board at Imam Abdulrahman Bin Faisal University.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.