
Abstract
Introduction:
An increasing amount of research has shown a link between psychopathological behaviors such as smartphone addiction, depression, anxiety, and stress. The aim of this study was to assess the association of smartphone addiction with depression, anxiety, and stress.
Methods:
A cross-sectional study was conducted between 26th January and 3rd March 2021. The sample was chosen using a convenient sampling technique and Raosoft tool. The survey assessed smartphone addiction using abbreviated versions of the Addiction Scale Short Version, a self-administered questionnaire that has been validated in the English and Arabic languages. Also, Depression and Anxiety Stress Scale was used to measure the level of depression, anxiety, and stress among the university students.
Results:
A total of 367 university students from the Medical and Health Sciences College participated. Our findings showed that smartphone addiction exhibited positive correlations with depression (r = 0.375, p < 0.01), anxiety (r = 0.253, p < 0.01), and stress (r = 0.328, p < 0.05). In addition, there was a strong positive correlation between depression and both anxiety and stress (r = 0.731, p < 0.01) (r = 0.778, p < 0.01), respectively. Finally, stress and anxiety showed a positive correlation (r = 0.708, p < 0.01).
Conclusion:
When combined, our data offer strong support for a bidirectional hybrid theory that takes into account the link between smartphone addiction and depression, anxiety, and stress. The current study’s findings might assist national health authorities in strengthening their efforts to prevent depression, anxiety, and stress associated with the use of modern technology.
Introduction
Smartphone addiction (SPA) is conceptualized as excessive smartphone use, which is associated with impairments in social, occupational, and academic functioning. 1 Despite the extensive literature on SPA, few studies have looked at the effect of mental health factors on different forms of smartphone use and how such use may lead to SPA. SPA has been linked to psychological disturbances in people and disruptions in daily work, according to a study done among university students. 2
Many previous studies examined the usage time of smartphones. In 2012, 1.5 h a day were spent on social media with a smartphone in the United States, compared to 3.5 h in 2017. However, according to data from the Organization for Economic Co-operation and Development, people aged 14–24 spend an average of 4.5 h each day using smartphones. 3
The prevalence of SPA varies from one country to another. For example, a survey of students from Switzerland was conducted as part of a study to determine smartphone usage and addiction. Of the 1519 students, 16.9% had a SPA. 4 On the other hand, a meta-analysis of research conducted on medical students in seven different Asian nations. The study found that among Asian medical students, SPA was common (41.93%). 5 In Palestine, we did not find any published studies on SPA.
Regarding the mental health outcomes and their relation to SPA, the first important mental disorder is depression, which may impact SPA in the world. It has a significant impact on workers’ quality of life and productivity and may have a direct financial cost.6,7 A study found that 28.0% of medical students worldwide have depression. 8 Also, one study found that reducing excessive smartphone usage can help relieve depression. 9 Depression has a global impact on individuals’ public health. According to the World Health Organization, depression is the primary cause of disability for more than 300 million people worldwide. 10 In Palestine, the Palestinian Ministry of Health’s Annual Report for 2016 presented that the incidence rate of mood (affective) disorders in the West Bank was 11.1 per 100,000 people. 11 Regarding college students, widespread public concern has been sparked by the high prevalence of depression among them. According to a review of studies, 34% of people reported having depressed symptoms. 12 A recent study of college students in the United States found that 48.14% of them had moderate to severe depression. 13 The coronavirus disease outbreak during the time of data collection in 2021 has made depression among college students more severe globally and presents significant difficulties for its prevention and treatment. 14
The second mental disorder that may have a relation with SPA is anxiety. The prevalence of anxiety worldwide has reached significant levels. A study on the prevalence of anxiety among medical students worldwide discovered that 33.8% of them reported experiencing anxiety. 15 Epidemiological surveys have estimated the lifetime prevalence of anxiety disorders to be 14.5%–33.7%, which means that up to about one-third of people will have any type of anxiety illness at some point in their lives. 16 In the same vein, one study found that confusion and instability in today’s world are sources of anxiety. 17 Also, numerous studies have explored the association between SPA and anxiety. One study found that SPA scale scores were positively correlated with anxiety among university students. 18 In the same line, a study from China found that anxiety among college students can impact self-esteem. 19 For starters, some researchers hypothesized that SPA could be a predictor of anxiety.20,21 In addition, another study discovered that SPA severity is mildly to moderately correlated with anxiety severity in participants from the United States, 22 Korea, 23 China, 22 and Turkey. 24 Also, previous studies have found that SPA has the potential to create psychopathology.25,26 In addition, other studies have discovered links between smartphone use and anxiety, 27 as well as between smartphone use and sleep quality.28–30 An increasing body of data suggests that SPA is linked to stress, anxiety, and depression.31–34 An international issue is the high frequency of anxiety disorders among college students.35,36 According to a cross-sectional survey of college students in India, anxiety disorders were 30% more common than depression, which was 18% in Asia. 37 A study on depression, anxiety, and stress symptoms in Spanish college students revealed that anxiety disorders were more common in this population, with 23.6% than depression. 38 In the same line, one previous finding revealed that the sub-scores for depression, anxiety, and stress were all substantially and positively linked with higher SPA scores. 39
During the time of data collection for the current study at the beginning of 2021, Coronavirus disease 2019 (COVID-19) continued to spread around the world, quickly developing into a worldwide health emergency. 40 As a psychological consequence of COVID-19, one study found that COVID-19 anxiety was found to be associated with SPA severity. 34 This link of coronavirus outbreak and an increase in the prevalence of SPA and anxiety can be added to the associated risk factors that increase the likelihood of anxiety prevalence.
In spite the fact that many studies have discovered the negative impact of smartphone usage, very few studies have explored the positive impact of smartphones. Likewise, one study found a significant correlation between SPA and the frequency of positive health-related issues. 41 In the same vein, one study found that people who are depressed use smartphones more frequently to cope with their unpleasant feelings. 18
The third and final mental health problem that might have a relation with smartphone use is stress. People who endure stress have a specific psychological condition that they deal with on a daily basis. 42 The stress that is a component of modern existence has ingrained itself into the experience of the person living in this time. The numerous environmental circumstances endangering his or her welfare are the cause of this. A response to these dangerous environmental conditions is what is known as stress.43–46 Two types of stress are typically described in the literature: helpful eustress and distress. 47 Distress has been the subject of more concentrated focus in the majority of these investigations.
Young adults may also display stress symptoms linked to smartphone use. 24 Additionally, further studies have examined how concerning and alarming the stress levels of university students can be.48,49 One study revealed a link between stress and SPA. 50 Also, another study found that improper and excessive use of technology causes stress and suffering. 51 Finally, one study among teenagers found that stress was positively correlated with the severity of SPA. 52
The current study aimed to investigate the relationship between SPA and depression, anxiety, and stress among Palestinian medical college students at An-Najah National University.
This relationship between SPA and depression, anxiety, and stress was not investigated before using Palestinian samples. We used a smartphone because all students have this device and are preoccupied with using it. Our research contributes by proposing and testing a model for SPA and its consequences. To begin, we looked into the fundamental mechanisms that link SPA to depression, anxiety, and stress. It is critical to explore the impact of SPA among university students. The impact can extend to cause anxiety, depression, and stress for university students.
Methods
Study design, population, and setting
A cross-sectional study has been conducted. The cross-sectional investigations are conducted over a brief period of time or at a single moment in time. Usually for the aim of public health planning. They are carried out to determine the prevalence of the result of interest for a particular group. 53 The study was carried out between January and March 2021 among 367 university students who were selected from various branches of the Medical and Health Sciences College. The sample was chosen using a convenient sampling technique, and Raosoft software tool for sample size calculation. The sample size was determined with a 50% response rate, a 5% margin of error, and a 95% confidence level. The response rate of the questionnaire was 100% among the participants due to that the sample was collected through convenient techniques and face-to-face interviews, which enabled us to exclude any participant who refused to participate from the beginning of the data collection process. The current study enrolled students from Medicine, Nursing, Pharmacy, Medical Imaging, Audiology and Speech Therapy, and Optics. Those who refused were disqualified.
Inclusion and exclusion criteria
All undergraduate students enrolled in An-Najah National University’s Medical College for the spring semester of 2020–2021 were eligible to participate and were included in the study upon their acceptance to participate. However, the students who claimed that they never used smartphones and those who claimed that they were unable to engage in the questionnaire answering session were excluded.
The data collection process
After obtaining approval from the Institutional Review Board of An-Najah National University, a face-to-face interview in the lecture classes was conducted with the respondents to collect research data. The questionnaire took approximately 30–40 min to complete.
Instruments
The first section of the questionnaire collected sociodemographic and behavioral data, including age (years), gender, university major, study year (1st, 2nd, 3rd, 4th, and 5th year), daily duration of smartphone use in hours, smoking, and history of chronic diseases. The second component of the survey assessed SPA using abbreviated versions of the Arabic and English Smartphone Addiction Scale Short Version (SAS-SV), a self-administered questionnaire that has been validated in both languages. Ten items make up the scale, such as “Missing planned work due to smartphone use.” The internal consistency and concurrent validity of SAS-SV were verified (Cronbach’s alpha = 0.967) to explore the prevalence of SPA.54,55 Furthermore, the scale’s validity in numerous recent cross-cultural studies, such as those conducted by Lopez-Fernandez, provides evidence for its validity. 56 There are no reverse scores involved, and the scale is incredibly quick and simple to use. Participants were asked to rate how much they disagreed or agreed with ten statements concerning their current smartphone usage in the SAS survey. A 6-point Likert scale is used in the SAS questionnaire (strongly disagree, disagree, weakly disagree, weakly agree, agree, strongly agree). The total number of answers was tallied and compared to male and female cutoff criteria of 31 and 33, respectively. Students who received a higher score than the cutoff were labeled as addicted.
The third part of the questionnaire measured depression, anxiety, and stress using the Depression Anxiety Stress Scale (DASS-42). The scale consisting of 42 items was founded by Lovibond and Lovibond 57 is available in a variety of languages, including Arabic. The Arabic DASS discriminates between depression, anxiety, and stress to a smaller extent than the English DASS, according to confirmatory factor analysis. The factor loadings for all 42 items were equivalent to the English DASS, demonstrating that the items had been translated and adapted correctly. Cronbach’s alpha was used to evaluate the internal reliability of the DASS-42 subscales for anxiety, depression, and stress. The depression scale’s alpha was 0.888, the stress scale’s alpha was 0.866, and the anxiety subscale’s alpha was 0.833. The item-internal consistency of subscales is good (Cronbach’s alpha values were more than 0.70). 58 The DASS uses a 4-point Likert scale ranging from 0 to 3 to assess negative emotional symptoms and comprises three subscales (depression, anxiety, and stress), each with 14 items. The total item scores, which can range from 0 to 42, are added to score these subscales.
Data analysis
The statistical software utilized for data analysis was IBM SPSS version 26 (SPSS Inc., Chicago, IL, USA). Age, gender, university major, study year, daily smartphone usage per hour, smoking, and history of chronic disease as demographic variables that were analyzed using descriptive statistics of percentages and frequencies. There was no missing data from the respondents’ responses as filling out the questionnaire was done among a convenient sample under the author’s supervision. Therefore, any respondent not complete the questions was omitted before arranging the dataset in SPSS. In order to examine the key traits of the sample, we also employed descriptive statistics, means, standard deviations, range, skewness, and kurtosis for all of our measuring variables, including depression, anxiety, stress, and SPA. Pearson correlation to determine whether there is statistical support for a linear relationship among the variables in our study, the coefficient between depression, anxiety, stress, and SPA was calculated. In step one, we used demographic factors (age, gender, university major, study year, daily smartphone usage per hour, smoking, and history of chronic disease) to predict depression, anxiety, and stress. In step two, we employed hierarchical regression analysis to predict depression, anxiety, and stress. In contrast, the SPA was used to predict depression, anxiety, and stress in step 2 using demographic factors (age, gender, university major, study year, daily duration of smartphone usage per hour, smoking, and history of chronic disease).
Ethical considerations
The Arabic invitation letter and consent forms were proposed at the opening pages. The students who accepted to participate proceeded to fill out the questionnaire by face-to-face interview. The study was authorized by An-Najah National University’s Institutional Review Board (Ref. no. 1.201) and conducted according to the standards of the American Psychological Association (APA. 2010) and the 2013 Helsinki Declaration.
Results
Characteristics of participants
As shown in Table 1, the average age was 20.4. Male respondents accounted for 17.2% (n = 63), whereas female respondents accounted for 82.8 % (n = 304). Studying medicine accounted for the highest percentage of the total participating students at 24% (n = 88). According to the participants’ academic year, second-year students had the largest percentage, at 38.7% (n = 142). A significant number of students spent more than 4 h on their smartphones, at 84.2% (n = 309). Additionally, a high percentage of students did not smoke cigarettes, at 88.3% (n = 324). Finally, a high rate of them did not report chronic diseases, at 94.6% (n = 347).
Sociodemographic characteristics of the study participants.
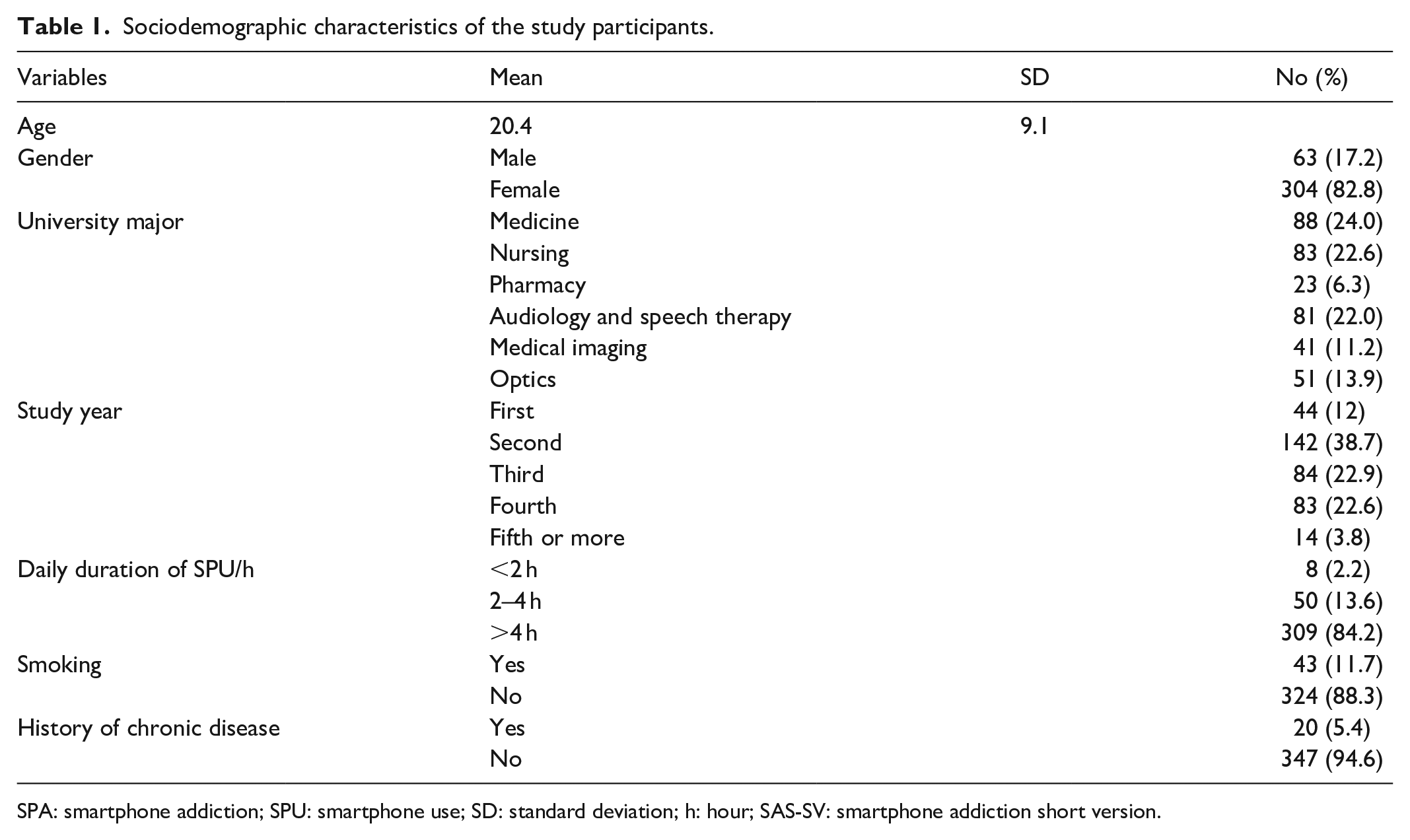
SPA: smartphone addiction; SPU: smartphone use; SD: standard deviation; h: hour; SAS-SV: smartphone addiction short version.
Table 2 presents descriptive statistics of the SPA and depression, anxiety, and stress. Participants reported having nearly moderate levels of depression, anxiety, and stress.
Descriptive statistics for study variables.

Table 3 lists the findings of the correlational study. Particularly, SPA showed positive correlations with depression (r = 0.375, p < 0.01), anxiety (r = 0.253, p < 0.01), and stress (r = 0.328, p < 0.05). In addition, there was a strong positive correlation between depression and both stress (r = 0.778, p < 0.01) and anxiety (r = 0.731, p < 0.01). Finally, stress and anxiety showed a positive correlation (r = 0.708, p < 0.01).
Correlations among study variables.

p < 0.01.
In Table 4, we examined the ability of demographic factors (age, gender, university major, study year, daily duration of smartphone usage per hour, smoking, and history of chronic disease) to predict depression, anxiety, and stress using a hierarchical regression analysis. SPA was used not only to predict depression, anxiety, and stress in step 2, but demographic factors (age, gender, university major, study year, daily duration of smartphone usage per hour, smoking, and history of chronic disease) were also taken into account. Our research found that depression was predicted (negatively from medicine to nursing, pharmacy, audiology, radiology, and optics) by a person’s university major (β = −0.10; **p < 0.01), smoking; smokers predicted depression (β = −0.16; **p < 0.01), having a history of chronic disease (β = −0.10; **p < 0.05), and having SPA (β = 0.33; **p < 0.01). Age, gender, study year, and amount of daily smartphone use did not, however, predict depression. However, anxiety was influenced by the following factors: gender, female (β = 0.12; **p < 0.01), university major (β = −0.14; **p < 0.01), smoking (β = −0.19; **p < 0.01), and history of chronic illness (β = −0.16; **p < 0.05). Finally, our results showed that smoking (β = −0.15; **p < 0.01) and SPA (β = 0.29; **p < 0.01) were the only variables that might predict stress.
Hierarchical regression analysis for variables predicting depression, anxiety, and stress.
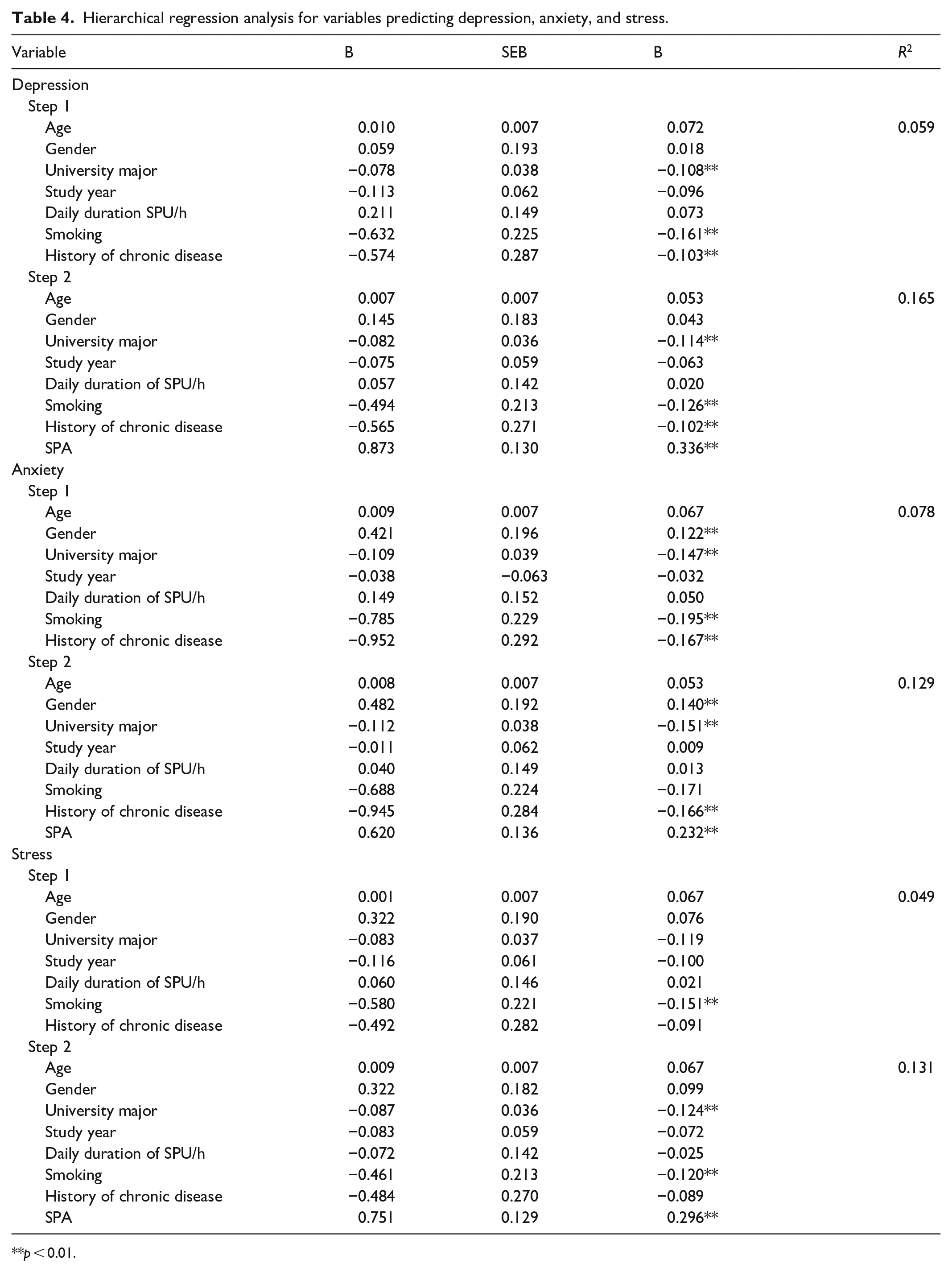
p < 0.01.
Discussion
To our knowledge, this is the first study in Palestine to investigate the associations between depression, anxiety, and stress with SPA. Our study found the SPA to be 37.9%. Consistent with the current study, a meta-analysis showed that among 3651 medical students, the pooled prevalence of internet addiction was 30.1%. 59 The prevalence of SPA can differ from one country to another, six studies with a pooled cohort size of 2236 medical students comprised another study. The combined SPA prevalence is as follows: Egypt 10.9% was the highest prevalence rate, with Saudi Arabia having the second-highest at 8.8%, Indonesia at 6.1%, and India at 3.8%. 60 The difference in SPA and internet addiction may be attributed to economic status and the availability of internet access.
The first hypothesis of the present study demonstrates an association between SPA and depression, anxiety, and stress. SPA found to be a strong predictor of depression, anxiety, and stress. Consistent with the current study, a body of evidence suggests that SPA is linked to psychopathology symptoms such as depression, anxiety, and stress.28,61,62,18
According to one study, SPA was associated with anxiety at 25% and sadness at 7%. 63 In addition, a large number of studies have found a strong association between SPA with depression and anxiety.28,18,64,65 Another study revealed that depression and SPA were frequently linked. 27
Despite the fact that a large number of studies revealed a negative effect of smartphone usage on people’s mental health, some very few studies discovered that smartphone use is linked to a reduction in stress, which then results in a drop in depression. These studies found that one of the key pathogenic aspects in theories of depression is people’s failure to control or neutralize stress, resulting in anxiety state and depression comorbidity.66–68
The link between smartphone use and stress levels is now well-researched. 69 Smartphones, according to most studies, create stress by extending working hours and increasing communication pressure.70,71 The prevalence of high levels of perceived stress increased along with heavy smartphone use, according to a study that examined the relationships between physical activity, smartphone usage, and perceived stress in Chinese college students. 72 The current study found that perceived stress was positively connected with SPA in medical college students, similar to earlier studies.73,74 Also found that the more SPA felt among medical college students, the more likely to develop stress. This is in line with the general strain theory, 75 which states that any type of strain or stress that an individual encounters will result in unpleasant feelings, which will lead to harmful behaviors. Also, stress has been demonstrated in numerous studies to be a significant risk factor for individual addictive behaviors.76–78 According to the stress generation hypothesis, 79 depressive individuals have a propensity to maintain depressive interpersonal relationships, which furthers the maintenance of depression. As a result, negative interpersonal events over an extended period of time lead to the generation of stress and stress conditions. Conversely, one study found that smartphones have evolved into a very good replacement and appear to more fully meet the criteria of a social actor since they are portable, in continual communication with their users, more thoroughly address human senses and wants, and provide multifaceted methods of interacting. 80 At the same line, another study found that smartphones can act as a “first-aid-in-the-pocket.” 81 From our research data and a lot of research, we have found that many studies encounter the negative effect of stress in increasing the level of SPA among the general population, including also the University students. As shown by the current study and other studies, SPA is primarily associated with an increase in depression, anxiety, and stress, despite the fact that some earlier studies have linked smartphone use to positive effects.
In line with the second study hypothesis, it was discovered that sociodemographic factors and SPA can both predict depression, anxiety, and stress. In particular, university major, smoking, and history of chronic disease can predict depression. Also, gender, university major, smoking, and history of chronic disease predicted anxiety. Finally, only the smoking variable predicted stress in the current study. These results are consistent with earlier research findings. A study conducted among 10,000 residents of Yazd Greater revealed a strong relationship between depression, anxiety, and stress and sociodemographic factors. 82 Also, a significant association among smokers 41.5% were addicted to smartphones (p = 0.039). 83 Regarding the effect of differences in age groups and other demographic variables with their relation to SPA, another study found that there are significant differences in age groups, work situations, and time invested. 84 Finally, consistent with our current study, one study found that the more time spent on the mobile device, the higher the score on the SAS measurement scale. 85
There are a few limitations to the study that should be acknowledged. First, our sample was limited to medical college students. When conclusions are applied to other populations, caution should be exercised. Second, our research is based on a cross-sectional design. When it comes to causation, we should pay great attention to how we interpret our findings. Furthermore, the cross-sectional survey design of our study, which examined only one point in time, may have limited the study’s generalizability.
Third, male respondents accounted for 17.2%, whereas female respondents accounted for 82.8 %, the main cause to take this male to female ratio is that the actual female student ratio in the medical college is 75%, according to university statistics. Experimental and longitudinal approaches may be used in future studies in Palestine to discover causal correlations between these factors. Future studies should examine the possibility of using smartphones to deliver specific therapeutic interventions in place of problematic behaviors.
The current study has a lot of potential because it is the first in Palestine to look into the relationship between SPA and three main mental health disorders. Additionally, during COVID-19 accounting, specific attention was given to investigating SPA. The community’s stigma was found to be a negative factor that reduced intrinsic motivation and decreased work retention among medical students in a study that examined the effects of COVID-19 on career choices in health professionals and medical students. 86
Implications for clinical practice
It is critical to explore the impact of smartphone usage among university students. The impact can extend to cause anxiety, depression, and stress for university students. The current study can shed light on the severe consequences of excessive smartphone use, allowing stakeholders to plan how to reduce and avoid the negative consequences of smartphone use. Additionally, the study results can guide and encourage university students to decrease their smartphone use to the satisfied normal and below 4 h per day.
Conclusions
When combined, our data offer strong support for a bidirectional hybrid theory that takes into account the link between SPA and depression, anxiety, and stress. The current study’s findings might assist national health authorities in strengthening their efforts to prevent depression, anxiety, and stress associated with the use of modern technology.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241227367 – Supplemental material for The relationship of smartphone addiction with depression, anxiety, and stress among medical students
Supplemental material, sj-docx-1-smo-10.1177_20503121241227367 for The relationship of smartphone addiction with depression, anxiety, and stress among medical students by Adnan Lutfi Sarhan in SAGE Open Medicine
Footnotes
Acknowledgements
The author would like to thank all the participants. Also, would like to express gratitude to An-Najah National University for their support, interest, and cooperation in completing this study.
Author contributions
AS: Conceptualization, Data collection, Writing—Original draft preparation, reviewing, and editing, Methodology, Software analysis, Supervision.
Availability of data and materials
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Institutional Review Board (IRB) of An-Najah National University (Ref. no. 1.201, 08.1.2021).
Consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.