
Abstract
Objectives:
Household hygiene and food safety are essential parts of food security; better food safety and hygiene will help reduce the chances of illness for young children and family members rarely studied in the selected area of coastal Bangladesh. The study aimed to discover the knowledge, attitude, and practice levels for cleanliness, hygiene, and food safety in the household.
Methods:
In this study, we employed a cross-sectional survey with simple random sampling to collect data from 384 childbearing mothers. The survey used the pretested, validated, and standardized (knowledge, attitude, and practice) questionnaire-model-based interview guide.
Results:
According to our study analysis, the knowledge, attitude, and practice scores among mothers were inadequate for household cleanliness and hygiene management. In the area context, knowledge efficiency was related to family type (joint and nuclear). Family economic conditions strongly influenced mothers’ attitudes and behavior toward knowledge, attitude, and practice score. Unemployed and illiterate mothers have lower knowledge, attitude, and practice scores. Educated mothers have better knowledge, attitude, and practice score compared to illiterate mothers (p < 0.014). Nuclear family knowledge, attitude, and practice attitude was much greater (p < 0.04) and wealthier families showed better practice (p < 0.001) toward cleanliness and food safety in the household level.
Conclusions:
The study discovered the mothers’ and household members’ attention need to improve the knowledge, attitude, and practice toward proper hygiene and food safety at the household level of marginalized populations in coastal Bangladesh.
Highlights
The study investigated the coastal Bangladeshi mothers with 2 years child at home and how hygiene and food safety knowledge, attitudes, and practices play a vital role in supporting household food safety and good health for all members.
Illiterate, unemployed mothers had lower knowledge, attitude, and practice scores in this study than the literate and employed.
Effective food safety and hygiene-based education are needed in coastal areas to raise food safety knowledge and encourage safer eating habits at home.
Introduction
Food safety and hygiene is a developing global problem that significantly affects public health worldwide. 1 According to the World Health Organization (WHO), 600 million people (almost 1 in 10) in the world fall ill after eating contaminated food, and 420,000 die every year, 33 million healthy life years lost as DALYs (disability-adjusted life year) for this reason. 2 About 2.2 million deaths in the developing world occur because of foodborne illnesses each year, an estimated 1.9 million of which are children. 3 Between 2004 and 2013, among children under 5 years of age, underweight rates declined from 43% to 35%, and stunting rates declined from 51% to 39%, slow progress with regards to less-positive nutritional outcomes due to not concerning in household hygiene and food safety issue, the utilization pillar of food security and child undernutrition rates in Bangladesh remain among the highest in the world. 4 In September 2013, UNICEF reported that 2000 children under five dies daily from diarrheal infections, most of which were caused by a lack of safe water, sanitation, and hygiene conditions. 5 Now, according to the latest available data from UNICEF, 14,400 children under the age of five died from diarrhea in September 2023. 6 Epidemiological studies reveal that handwashing with soap can reduce the incidence of severe diarrhea by 48%, any diarrhea by 47%, and pneumonia by 23%. 7
There exists a significant correlation between various facets of food safety protocols, including disinfecting drinking water, and handwashing after lavatory use, and the prevalence of stunting among children residing in unsanitary slum settings in Bangladesh. 8 Food safety has been a “silent killer” for decades in both Bangladesh and India, contributing to the deaths of thousands of people and injuries to millions of others all over the world. 9 Food Security exists when people always have physical, social, and economic access to enough safe, nutritious, and culturally acceptable food for normal growth and development, as well as an active and healthy life.10,11 For the world’s population to have food security, protect natural resources, and improve health by making sure food is safe; the academics, food producers, consumers, and government agencies all need to be more aware. 12 There are several essential features of food systems that have significant implications for the health of the population, including food security, food safety, and optimal nutrition. The prevention of food-borne illnesses is the focus of food safety and hygiene, which also encompasses the handling, preparation, and storage of food. Consuming foods that are high in nutritional value is the focus of healthy nutrition. The concept of food security involves not only the safety of food and the provision of nutritious food but also a larger range of concerns concerning the availability, accessibility, use, and consistency of food. 13
Unsafe domestic food safety is increasingly linked with foodborne illnesses, home food source can become contaminated during lack of food safety and hygiene concern. The process starts from food production and distribution along the way from farm to plate as from home management of food hygiene. 14 As a result, food safety and hygiene control were a responsibility shared by all service holders in the food supply, distribution, cooking, and processing system; with each service component operating responsibly, the supply of safe food should be guaranteed. 15 However, a considerable majority of food-borne illnesses were caused by household food handlers mishandling and poorly preparing their food. 15 About 10%–20% of outbreaks of food-borne disease were the result of contamination food by handlers, a less careful behavior toward food preparation exacerbates the spread of food-borne infections from household. 16 The role of home food handlers, typically mothers, in ensuring food safety at the household level was widely recognized, but a better understanding of their food-handling skills with knowledge, attitude, and practices was required. 17 There was a significant proportion of food-borne illnesses arises from the home kitchen. 18 Though public awareness and concern about food-related risks and diseases was increasing, yet the escalation in the number of food-borne illnesses indicates that domestic food handlers still lack adequate food safety knowledge and attitude leading to wrong food-handling practices. 19
A considerable number of food-borne illnesses were generally associated with practices in the domestic kitchens. 2 Research highlights that about 50% and 87% of reported food-borne disease incidents arise within the home20–22 enhanced by a lack of education and awareness about food safety and food-handling practices. 23 To protect children’s health and well-being, examining mother’s attitudes and behavior and obtaining information on how food becomes unsafe in the home was vital. 24 It was difficult for maintain good food preparation, handling, and storage at home, it was necessary to educate domestic food handlers to reduce potential of food-borne illness and other food-related diseases. The governments of each nation need to be able to monitor their own progress and, as a result, require a standardized method of measurement applicable to their specific environments. 25 A well-planned program can accomplish gains in life-saving behaviors for mothers and newborns, proving that the action coordinated by government leadership can move the needle in the right direction even in situations with limited resources. 26
Mother and child health is an important indication of societal overall health management system. Maternal and child health care is gaining attention worldwide. Despite it, morbidity and mortality rates in poor countries remain worrying. An inquiry-based study examined Slovenian pregnant and nonpregnant women’s food safety knowledge and practices. About 291 pregnant women attended prenatal classes and 200 nonpregnant women attended parent consultation hours in ten randomly selected elementary schools. The study shows urban life and mothers aged over 25 have better food safety awareness. Prenatal classes should educate home food safety to enhance the security of food. 27 The study of rural women of Uttarakhand area in India assessed rural women’s knowledge, attitude, and practices on mother and child health, including reproduction, family planning, prenatal and perinatal care, hygiene, and nutrition. In the pretest phase, most respondents had moderate knowledge of pregnancy signs and the first trimester, but they lacked knowledge of immunization and welfare programs and services for mothers and young children. 28 Studies have consistently shown that Infant and Young Child Feeding (IYCF) practices during the first 24 months (about 2 years) have a significant impact on child health and development. For example, exclusive breastfeeding for the first 6 months of life is associated with a reduced risk of diarrhea, pneumonia, and other infections. 29 Additionally, complementary feeding practices that supply a variety of nutritious foods can help to prevent malnutrition and promote healthy growth. Mothers with children aged 0–24 months are the primary caregivers for their children and are therefore the primary decision-makers regarding IYCF practices. 30 By understanding the knowledge, attitudes, and practices of mothers in this age group, researchers can develop targeted interventions to improve IYCF practices and ultimately improve child health and nutrition.
In a Bangladesh refugee camp (Border area with Myanmar), a cross-sectional survey was conducted to evaluate the knowledge and practices of Rohingya refugees, particularly mothers, in water, sanitation, hygiene, and nutrition sector. Data were collected through convenient sampling and face-to-face interviews with 995 households. Without access to clean water and hygiene education, eradicating diarrhea, cholera, and other diseases in Rohingya refugee camps in coastal Bangladesh is impossible. 31 Small area estimation (SAE) provides precise and representative district-level estimates of food insecurity in an area here we target Bangladesh, with vulnerable districts in northern and southern regions. 32 Lack of hygiene and inadequate legislation causes food microbiological contamination in Bangladesh, causing food-borne illnesses. 33
Here the previous study shows that mothers in lower and lower middle-income countries have limited food safety and health knowledge where Bangladesh stands one of the country. 34 The child wasting, stunting, and maternal mortality rate are still high in Bangladesh 35 where food safety and hygiene can play a vital role. The last couple of years, Bangladesh is a developing nation located in South Asia, has a population of about 142 million people, a poverty rate of 33%, and a great deal of problems that are related to health. 36 Due to lack of education and population pressure, the nation faces challenges to increasing the health and happiness of mothers, babies, and children. This is a significant objective for the field of public health all around the world. One of the most significant difficulties that a nation’s public health care system must face is the responsibility of ensuring the health of the future generation.
This study aimed to assess food safety and hygiene-related knowledge, attitudes, and practices among mothers at home, having children under 2 years old in Noakhali and Lakshmipur districts in Bangladesh. It seems rare in the study area but very important for health aspects. The knowledge, attitude, and practice (KAP) of the childbearing moms in the study area regarding both food safety and cleanliness was evaluated through the course of this research. As a result of the findings, relevant stakeholders and policymakers will be better equipped to determine how to improve the situation.
Methods
Study design
A simple random sampling was used to conduct a cross-sectional study of the 384 mothers’ family in two purposely selected upazillas of two coastal districts (Figure 1). The data was collected using a pretested, validated questionnaire after standardized by a pilot study to 40 households (nearly 10.4%) adapted from United States Agency for International Development (USAID) and World Health Organization (WHO), KAP questionnaire model.37,38 The questionnaire contains questions about the sociodemographic characteristics, food safety and hygiene-related questions on knowledge, attitude, and practice. Our study area administration runs in four categories starting from division, district, upazilla, and villages. The area in this study covers seven villages under two upazillas of two coastal districts in Bangladesh (Figure 1).

Map of the study areas at Noakhali and Lakshmipur coastal districts in Bangladesh.
Study population
The study’s sample population included mothers with children aged 0 to 24 months. The questionnaire survey from the respondents was taken from November 2020 to January 2021. Participants were chosen using a basic random selection method. The research used a population study of randomly selected mothers from seven villages according to population segments. The household data was collected from selected villages in a geographical structure where they work together and use each other’s strengths while also promoting each village’s unique potential. Not all houses in the selected area had mothers with children who were less than 2 years, and sometimes mothers who were not present and uninterested in attending the survey were excluded.
Inclusion and exclusion criteria
The inclusion criteria for participating in this study are (a) Mothers having 0–2 year’s child, (b) taking part in food handling operation, and (c) staying permanently at the study area. Mothers who were seriously ill, who did not take part in food handling because of family and cultural reasons or were absent during data collection were excluded from the study.
Sample size determination and sampling procedure
Simple population proportion formula is used to determine the sample size among mothers with households, primary indicator, p = 50% (0.5 decimal as default), confidence interval (CI), Z (z score for large population) as 95%, and 5% margin of error (d), Using Cochran’s formula.38–41

Data collection tool
The respondents were selected on a face-to-face basis from seven villages of both districts. To make it manageable, a survey was carried out within the streets by starting from the middle point of the villages. Based on population, around thirty respondent data were collected randomly. USAID and WHO have developed many KAP questionnaire models that can be adapted for use in a variety of contexts. These models are based on the best available evidence and are designed to be easy to administer and analyze. They can be used to assess the knowledge, attitudes, and practices of individuals, households, or communities with some modifications to adjust local custom and culture. The questionnaire was prepared according to KAP model questionnaire used in many studies and organizations,38,40 guidelines for assessing nutrition-related knowledge, attitudes, and practices and WHO guideline for KAP survey were used. 38 Seven professionals in food science and technology and educational authority verified the questionnaire’s validity after pilot testing. The questionnaire was designed in English with Bangla translation about food safety and hygiene practices, knowledge, and attitude.
Scoring of variables
Eleven, five, and eighteen questions were asked to determine the level of knowledge, attitude, and practice about food safety and cleanliness, respectively, according to food safety and hygiene aspects with context and literature review.42,43 To calculate KAP, knowledge score, the question answer that was gathered given one score out of ten for each question. For questions at the knowledge level that contained two viable answers, one point was awarded for the correct answer, and two points were deducted for the incorrect response. The three score levels were offered for other questions about attitude and practice. In the section on practice, the participants were given a score of 0, 1, and 2 for a Bad, Fair, and Good level of practice, and in the section on attitude, the participants were given a score of 0, 1, and 2 for a Positive, Not Known, and Negative answer, respectively.42,44 The KAP score was ranked based on the overall score that was given. Mothers of the family, along with the father, who achieved a KAP score that was greater than or equal to the mean value were considered to have made the proper or positive response for knowledge and attitude. For practice mothers who gained 80%, 60%, and below the mean value of total score, respectively, indicated as Good, Fair, and Bad according to the scale.42,45
Data analysis
Data were entered using IBM SPSS (Version 27) for analysis. For categorical variables, data were presented by frequencies and percentages. The continuous variables are presented as mean ± SD (standard deviation). The ANOVA test was employed to compare the knowledge, attitude, and practice of respondents based on demographic profiles. Pearson’s correlation test was used to find out correlation among knowledge, attitude, and practice regarding food safety and hygiene.42,46 The Pearson’s correlation coefficient was used to measure the strength and direction of the linear relationship between two variables, with a value of 1 indicating a perfect positive correlation, 0 indicating no correlation, and −1 indicating a perfect negative correlation. Multiple linear regression was used to see the factors that influence the knowledge, attitude, and practice level of respondent. 47
Results
Characteristics of the childbearing mothers and family
The study focused on hygiene and food safety-related knowledge, attitude, and practice among child-bearing mothers with family. The socio demographic and family members’ dynamics affecting the KAP related to household hygiene and food safety was evaluated at the targeted area.
The demographic features of mothers revealed that most mothers completed elementary and secondary education (69.5%), while the percentage of fathers who completed higher secondary and higher education was slightly higher (70.6). The majority of mothers were housewives (95.3%). Muslim respondents made up 90.6% of the total. Only 19.3% of respondents reported a family income of greater than 310 US dollars per month (almost 26,000 Bangladeshi Taka) and maximum family income falls in the range of 125–310 USD (47.7%). The proportion of respondents who belong to each family type was nearly equal. Almost everyone has their own home (99.0%). Only 5.2% of the families used a sanitary toilet (Table 1). The family size is mostly nuclear family (50.3%) whereas joint family are half of the sample population (49.7%).
Demographic characteristics of the respondents.

Informal workers = Day laborer in other houses, weekly market business, farming helper on occasion, construction task, etc.
Formal workers = Farming regular basis, traditional local business, CNG Driver, Rickshaw Puller, etc.
The mother’s food safety and hygiene knowledge
In Figure 2, we get an illustration of the amount of comprehension that the respondents have regarding the cleanliness and safety of food. The level of knowledge that was presented seems satisfactory. The moms used safe water for cooking, cleansed their hands and utensils after handling raw meat and eggs, pasteurized milk, washed fruits, and vegetables in the proper manner, and disposed of garbage in the appropriate manner (100%). In Figure 2, it was found that 99% of moms covered food after it had been cooked, used clean and fresh utensils as containers for water, disposed of kid excrement in an appropriate manner, and utilized clean and safe water in their homes. It would suggest, on the basis of our knowledge level questions and the replies that were supplied by the mothers, that they are in accord with the cleanliness and safety of their household in line with childcare.

Food safety and hygiene-related knowledge first column denotes “No,” and the second column denotes “Yes.”
The mother’s food safety and hygiene attitude
Attitude regarding food safety and hygiene was illustrated in Table 2 based on our developed attitude questions. The finding showed that 74.5% of household respondents agreed with the term of keeping perishable foods in cool places like refrigerators. The mothers in the family believed that it was necessary to check the expiry date of packaged foods, use separate utensils for raw and cooked foods, and wash hands properly with soap before feeding child (100%). Only 9.6% respondents disagreed with the term that described, drinking water from main source should be treated (Table 2).
Food safety and hygiene-related attitude.

The mother’s food safety and hygiene practice
The practices of respondent mothers regarding food safety and cleanliness were depicted below (Table 3). The results indicated that many respondents have decent practice. More than 50% have effective child feces disposal procedures. A total of 73.7% of respondents cover their used clean water containers. Regarding the use of water for washing raw foods, 74.2% of respondents had inadequate practices. Maximum 96.9% improperly preserved prepared foods. Then nearly 65.9% do not wash hands and eggs prior to cracking them. Only 31% adequately checked the expiration dates on packaged items; then near 2.9% of respondents consumed goods that have degraded or exceeded their shelf life (Table 3). Regarding domestic waste disposal, cleaning fresh fruits and vegetables, preserving perishable goods, and boiling water supply, a moderate level of practice was demonstrated.
Food safety and hygiene-related practice.

Discussion
The KAP related to the factor’s food safety and hygiene
In the mean score of KAP, we see mothers’ education, family type, and family monthly income has significant relation with household hygiene and food safety practice and attitude (p value > 0.05) (Table 4). Though knowledge has no impact on family sociodemographic characteristics statistically, we can observe the mean KAP score individually in Table 4.
Mean score of KAP related to food safety and hygiene based on demographic profile.
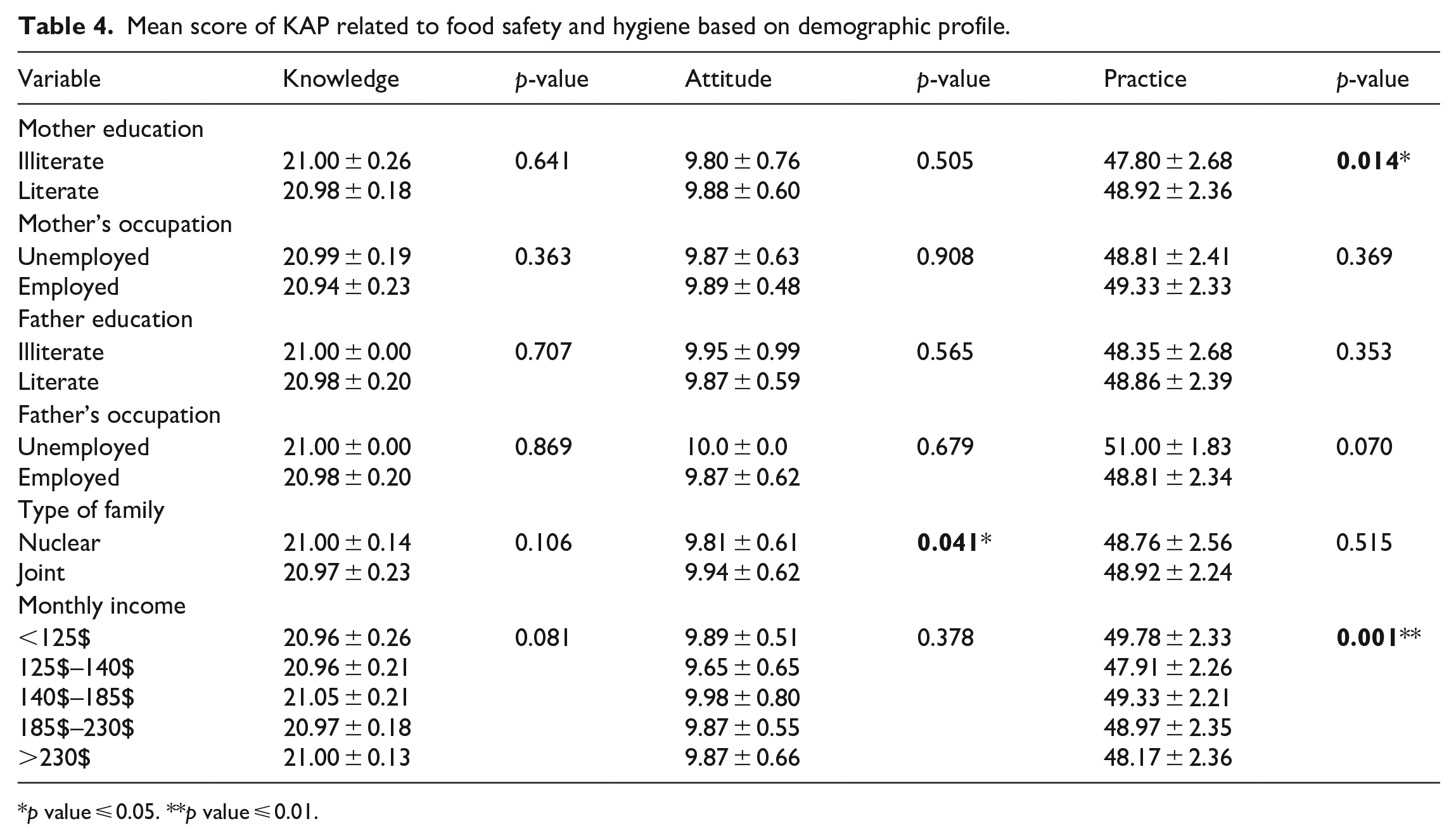
p value ⩽ 0.05. **p value ⩽ 0.01.
The table provides a summary of the mean values of three variables KAP in relation to several demographic factors in a sample population. The demographic factors include mother’s education, mother’s occupation, father’s education, father’s occupation, type of family, and monthly income. The mean knowledge scores range from 20.94 to 21.0, with no statistically significant differences observed between groups for education, occupation, and family income. The mean attitude scores range from 9.65 to 10.0, with statistically significant differences observed for family type. Those families that are nuclear have higher attitude scores compared to those whose family joint with more members, respectively. The mean practice scores range from 48.35 to 51.00, with a statistically significant difference observed for mothers’ education and family monthly income. Those with higher family monthly income and better mothers’ education level have better practice scores compared to those with lower monthly income.
Overall, the table suggests that factors such as type of family, education, and monthly income are the important determinants of knowledge, attitude, and practice related to hygiene and food safety topic in the population. The p-values indicate the statistical significance of the observed differences, with a p-value less than 0.05 indicating a statistically significant difference between the two groups.
The study evaluated mothers and family members’ level of knowledge, attitudes, and practices in relation to food safety and cleanliness at the household level. The knowledge, attitudes, and practices of mothers correlated with sociodemographic profile. The educational level of the parents, their employment situation, the type of family they had, and their income level are all major factors in the study KAP results concerning food safety and cleanliness of household. The study was conducted in the coastal area of Bangladesh, and most of the participants were housewife mothers (95.3%) having young child. When working with food, it was critical to practice proper food safety and hand hygiene because the hands play a significant part in the process of disease transmission.48,49 Effective motivational interventions can improve hand hygiene compliance in the foodservice sector, reducing food-borne illnesses and reducing chances of sick period and family income loss. 50 The women in this study claimed they cleansed their hands thoroughly before touching foods or participating in household activities. The mothers here employed hygienic knowledge mentioning using potable water for cooking, sanitizing their hands and utensils after encountering raw meat and eggs, pasteurizing milk, thoroughly washing fruits and vegetables, and appropriately disposing of waste as their knowledge level evaluation. Most mothers (99%) took measures such as covering food after cooking, using fresh and hygienic utensils as water containers, properly disposing of child excrement, and using clean and safe water in their households according knowledge level questionnaire score. This positive finding was synced to other study made by Sudershan et al., 19 in which the researchers discovered that 90% of women properly cleansed their hands before feeding their children, and 70% of women washed their hands before making and serving meals in the study area. It was important to thoroughly wash all raw items, including fruits and vegetables, and most participants say they did so where the question was how effective the wash process was? The household should be concerned about the quality of the water they used to wash fruits and vegetables. It was essential to keep raw and cooked foods separate since mixing them might result in cross-contamination with pathogenic germs, which can lead to foodborne illness. 43 The cleaning practice of washing fruits and vegetables was required to remove pesticides, which otherwise eaten can lead to illness. 51 Regarding the KAP home food safety and hygiene attitude, a majority of respondents (74.2%) had an inadequate attitude toward the use of water to wash raw foods. A maximum of 96.9% of prepared foods are inadequately preserved. Approximately 65.9% of people do not wash their hands and eggs before cracking them. Only 31% of individuals properly verified the expiration dates on packaged items. Here mothers’ lack of attitude due to education and family awareness can cause food-borne illnesses in family members.
The relations of the KAP mean score toward sociodemographics of families about food safety and hygiene among the household mothers
Table 5 shows the mean and standard deviation (SD) values for three variables KAP and their correlations with each other.
The correlations of mean score of KAP of food safety and hygiene among respondents.

The mean knowledge score was 20.98 ± 0.20, the mean attitude score was 9.87 ± 0.61, and the mean practice score was 48.84 ± 2.4. The correlations between knowledge and attitude were −0.083, indicating a negative correlation. The correlation between knowledge and practice was −0.046, indicating a negative correlation. The correlation between attitude and practice was 0.075, indicating a positive correlation.
Food hygiene and handling procedures in an area exhibit variability across households, with factors such as greater education, food expenditure, and refrigerator temperature serving as indicators of improved practices. 52 The habits of respondents about the cleanliness and safety of food preparation were demonstrated to be fair in the current study according to KAP score index. The findings suggested that most respondents already have established practices as higher income families use refrigerators and modern equipment to keep food safe. More than half of the household mothers have efficient methods for disposing of the excrement of children as childcare programs are popular through education and mass media knowledge dissemination programs. Unsafe drinking water was a major cause of diarrheal disease among children53,54 and in this study, all women has good practice about drinking safe and clean water. Higher poor practice score was found regarding checking expiry date of packaged food, water used for cleaning utensils, and washed eggs before cracking the shells. In our study, we found a significant association between father’s unemployment and lack of good practices regarding food safety and hygiene. In Nablus, Palestine, parents who possess a positive attitude, higher education, and urban residence are more likely to have improved knowledge, practices, and attitudes regarding the prevention of food poisoning. 55 Furthermore, the findings highlight that mother’s education, occupation, and income status should be increased to improve the knowledge, attitude, and practice regarding food safety and hygiene as good handling of food at household level help to reduce the risk of food-borne illness of vulnerable groups specially children. Moreover, this study can be used as an initiative for other researchers to conduct more studies on food safety and hygiene in different geographical areas.
Table 6 demonstrates the sociodemographic factors that influence the knowledge, attitude, and practice level of respondents in family regarding food safety and hygiene. The type of family, parents’ education and occupation, total number of children, and household monthly income showed a significant association with the KAP of food safety and hygiene. The level of knowledge was significantly higher among respondents who lived in joint families compared to those who lived in nuclear families and number of family members (p < 0.021). As the mother’s education level increased, the practice of the household food safety and hygiene improved (p < 0.049). It was found that the level of practice score was much lower in families whose fathers were unemployed (p < 0.028). However, food safety and hygiene practice show better if the number of family members decrease (p < 0.038). The higher family monthly income level, the practice score significantly increased (p < 0.001). There were no statistically significant changes found in the religion, father’s education, and mother’s occupation with the knowledge, attitude, and practice score of the respondents.
Factor affecting the knowledge, attitude, and practice about food safety and hygiene.

β = standardized coefficient; SE = standard error; t = t-statistics.
Data were generated from multiple linear regression analyses. A p-value less than 0.05 is considered statistically significant.
Several studies have found a substantial correlation between a mother’s age and marital status and her offspring’s awareness of food safety issues56,57 with a strong correlation between the mother’s level of education, hygiene, handwashing practices, and sanitation status, and the child’s nutritional health in the household level. 42 Urban mothers in Addis Ababa, Ethiopia, are influenced by social and environmental factors, highlighting the need for nutrition education campaigns targeting families and children. 58 Poor WASH knowledge and practice significantly increase the risk of childhood diseases and nutritional status in rural Bangladesh. 59 Urban residence and mother’s education level significantly improve early childhood health in Turkey, with urban living conditions and better living conditions being key factors that can be applicable for other regions of the world, especially mother’s education. 60 Here, our study also consistent with the higher mother education play a crucial role in the improvement of the household food safety and hygiene practices.
However, the link that we discovered in this study was statistically significant relation between family type and knowledge scores. According to this study’s findings, mothers who were literate and had jobs had a greater knowledge base than mothers who were not literate and do not have jobs. It was believed that mothers’ knowledge and habits about food safety can be improved through education as well as other educational activities such as awareness programs.61,62 Considering that nuclear families make up 61.97% of all families in one study in Peru 2019, it is possible to use this information to inform educational efforts that will improve food safety in households. 63 There is a correlation between having a nuclear family and having better health outcomes for children and adolescents when compared to having a single parent or having stepfamilies. 64 The scenario may be caused by a nuclear family having less members and better decision taking environment compared to joint large family with many members. In case of attitude about food safety and hygiene, maximum women have positive attitudes. This result was higher than a study conducted in Ghana Accra, 65 India, 44 Ethiopia, 66 and Nigeria. 67 A significant association of parents’ education and family income with the attitude scores was found in line with the study of Mendagudali et al. 44 The female food handlers knew hygiene, cleaning, and sanitation uses in workplace hygiene maintenance including handwashing, glove use, instrument/utensil cleaning, and detergent use, but they were ignorant that Salmonella and hepatitis A are food-borne diseases if they clean and used kitchen items in diseased conditions. 65 The outcomes of the study in Malaysia led the researchers to the conclusion that persons who worked with food had adequate understanding of food safety; despite this, the researchers found that the perceived knowledge did not translate into actions carried out while working. 49 It was discovered that women in the Khaza bazar region, India, have a healthy attitude toward the KAP of food safety including the fact that there is a positive correlation between the various KAP variables suggests that regular training on safety measures, as well as its function in the propagation of the disease, is boosting awareness of food safety. 44
This investigation had some shortcomings. The inability to determine causality due to the use of cross-sectional survey data. Moreover, the samples were selected at random so there was a higher response rate, and this may have an impact on the precision and dependability of some of the conclusions. Childbearing women described their own levels of knowledge, attitudes, and practices toward food safety and cleanliness toward household food security aspects in selected areas.
Conclusion
The majority childbearing mothers in the coastal area of Bangladesh under investigation come from low socioeconomic backgrounds and have a lower level of education in this communities. Higher levels of maternal education, increased family income, and smaller family size positively impact women’s knowledge, attitude, and practice regarding cleanliness and food safety at the household level, particularly in relation to childcare. Therefore, there was a need to increase mothers’ awareness and education on issues relating to food safety and cleanliness, particularly for those moms who were involved in the handling of foods. Despite having generally, a level of knowledge, attitude, and practice, mothers and household members still need to know and care about the food safety overall process and address family-related snags against food safety practice. Simple but important practices like the processed food expiry date check and proper food storage awareness. Regular food safety and security-related training programs at household level need to be arranged by local authorities to help improve food safety and hygiene at household level.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241264741 – Supplemental material for Assessment of the knowledge, attitude, and practice of childbearing mothers in the geographically coastal region of Bangladesh for cleanliness and food safety of food security
Supplemental material, sj-docx-1-smo-10.1177_20503121241264741 for Assessment of the knowledge, attitude, and practice of childbearing mothers in the geographically coastal region of Bangladesh for cleanliness and food safety of food security by Md Abdullah Al Mamun, Ruhina Binta A Ghani, Lincon Chandra Shill, Farjana Afroz, Akibul Islam Chowdhury, Fouzia Akter, Effat Ara Jahan, Md Masud Rana and Jianfeng Li in SAGE Open Medicine
Footnotes
Acknowledgements
The research study well supported by the department of Geography, Hong Kong Baptist University, and the department of Food Technology and Nutrition Science, Noakhali Science and Technology University, Bangladesh. The authors are thankful to the local childbearing mothers in Noakhali and Lakshmipur districts, Bangladesh for participating in the study.
Availability of data and materials
Available upon request.
Author contributions
Conceptualization: Md Abdullah Al Mamun, Farzana Afroz; Data curation: Md Abdullah Al Mamun, Farzana Afroz; Formal analysis: Md Abdullah Al Mamun, Akibul Islam Chowdhury, Ruhina Binta A Ghani, Lincon Chandra Shill; Investigation: Md Abdullah Al Mamun, Farzana Afroz, Ruhina Binta A Ghani, Effat Ara Jahan, Fouzia Akhter, Md Masud Rana; Methodology: Md Abdullah Al Mamun, Lincon Chandra Shill, Jianfeng LI; Software: Md Abdullah Al Mamun, Akibul Islam Chowdhury, Ruhina Binta A Ghani, Lincon Chandra Shill; Validation: Md Abdullah Al Mamun, Farzana Afroz, Ruhina Binta A Ghani, Effat Ara Jahan, Fouzia Akhter, Md Masud Rana; Writing—original draft: Md Abdullah Al Mamun, Jianfeng LI, Farzana Afroz; Writing—review & editing: Md Abdullah Al Mamun, Farzana Afroz, Ruhina Binta A Ghani, Effat Ara Jahan, Fouzia Akhter, Md Masud Rana, Jianfeng LI.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Ethical Review Board of Noakhali Science and Technology University, Noakhali, Bangladesh, and other appropriate authorities- approval no- NSTU/RC/20/C-166. The researchers clarified the objective of this research and obtained informed consent from the respondents.
Consent for publication
All of authors read and approved the final manuscript considering for publication.
Informed consent
Written informed consent was obtained from all respondents before the study.
Or
Verbal informed consent was obtained from all respondents before the study after the study’s purpose was explained.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.