
Abstract
Objectives:
Neither the current assessment tool of Sri Lanka for food establishments is based on prevailing Food Regulations 2011 nor did its focus cover serious adaptions for precautions upon prevention of the diseases. The study aims to develop a food handling practices assessment tool based on the Sri Lanka Food Regulations 2011 and to assess food handling practices using a developed tool in the Regional Director of Health Services area, Kalutara.
Methods:
The study consisted of developing food establishments’ assessment tool (FEAT) in accordance with Food (Hygiene-1742/26) Regulations of Sri Lanka 2011 and assessing the food establishments using the developed tool in the Regional Director of Health Services area, Kalutara, Sri Lanka. The development of FEAT was carried out to mark inspection scores for food establishments conforming to Food Regulations, others reviewed international food safety protocols and agreements following key informant interviews and focus group discussions. Fully developed FEAT was transferred to a mobile application for ease of use, and assessments were conducted among 421 food establishments in three Medical Officer of Health areas.
Results:
FEAT contained 11 domains including 75 items with more than 100 assessment points including a guide to conducting an assessment of food handling, compared to the current version of the assessment tool in Sri Lanka. The majority of participants included in the qualitative assessment agreed to include a 1–5 scoring scale to report hygiene levels and to use hygiene regulation to develop FEAT as a legal basis. The highest percentage of food establishments (69.4%) in the “Good” category were in the Bandaragama Medical Officer of Health Area and the highest percentage of food establishments (54.5%) in the “very poor” category were in the Walallawita Medical Officer of Health Area. Food establishments taking precautionary measures, which are not assessed in the current tool, were good, but maintenance of processing area and installation of overhead structures and fitting were poor in food establishments in all three Medical Officer of Health Areas.
Conclusions:
The novel food assessment tool FEAT is a completely valid instrument for food establishments. It is designed for easy administration and supports reliable assessments. Overall food handling practices of food establishments in the Kalutara Regional Director of Health Services area following assessment with FEAT were in the “satisfactory” category.
Keywords
Introduction
An international analysis by the world health organization (WHO) revealed, in 2019, that an estimated 600 million people—almost 1 in 10 persons in the world—fall ill after eating contaminated food, and 420,000 die each year, resulting in the loss of 33 million healthy life years disability-adjusted life years (DALYs). Children under 5 years of age carry 40% of the food-borne disease burden, with 125,000 deaths every year. 1 Diarrheal diseases are the most common illnesses resulting from the consumption of contaminated food, with 550 million falling ill and 230,000 deaths every year. 2 Indoor morbidity and mortality statistics in 2017 revealed that categories (A00–A09 of International Coding Diseases 10 coding) showed the rate of mortality due to infectious intestinal diseases for the 100,000 population from 2010 to 2017 as a plateau. In 2017, infectious intestinal diseases prevailed in all age categories with the highest rate among the working age group. 3 Diseases due to contaminated food have been still prevailing a detrimental issue for Sri Lanka.
Describing the locations and settings of food contamination, the Canadian and USA health bureaus summarized places where contaminations are best known to occur. It indicated that an average of 73.4% in Canada over a 10-year analysis and 43.2% in the United States over a 5-year analysis 4 occurred as a primary source by food service establishments following food-borne diseases and outbreaks. Food authorities in any country carried out an inspection of food establishments as one of their main duties with great importance and focusing fundamental principles of Hazzard Analysis and Critical Control Points (HACCP) to safety of food at the time of delivery to consumers. 5 In Sri Lanka, since the administration of powers of the inspection was decentralized, local food authorities were, in the majority, vested with potential responsibilities to place with food safety and quality management system to ensure that meals do not compromise public health. Essentially, adopting proper food assessment tools for inspections is pivotal, because food establishments are the final mode of delivery of the whole food chain furnishing the final product to consumers. Since food establishments were highlighted as the main source of food-borne diseases, proper and valid assessments using tools need to be introduced. Several situations can be identified where inspections were conducted to assess food handling practices such as routine inspections to monitor the food establishments, special inspections for food-borne diseases epidemics, inspections over first-time registration of food establishments, and inspections in emergencies.
Under the “Council’s Eat Safe Brisbane food safety rating scheme” checklist, which was used by food safety council officers during routine food safety inspections, all licensed food businesses within Brisbane were issued with a food safety star rating. This checklist was based on an assessment conducted by Council under the Food Act 2006 and good management practices. 6 In a study done in Nigeria on food vendors in the street, a checklist to collect data to determine the sanitary practices on food handling in food establishments was adopted using “WHO essential requirement for the safety of street-vended foods.” 7 In addition, environmental practices and observed food handling practices of food vendors were included via 10 items in the checklist, whereas scoring was allocated as “1” for correct answers and “0” for incorrect answers and as a percentage of the final score, 50% was taken to divide good and bad practices. 8 Many authors have described their food assessment tool followed in accordance with country food law or international food algorithms.
In 2012, according to Food (Hygiene) Regulations, Sri Lanka, food hygiene means all conditions, measures, and practices necessary to ensure the safety and suitability of food at all stages of the food chain. 9 By defining legally, it encapsulates the concept and differs from ordinary and everyday meaning. 10 Food (Hygiene) Regulations of Sri Lanka 2011 should be applied to all establishments dealing with the processing, transport, distribution, handling, storage, or sale of food or any other matters related to food establishments. In Sri Lanka, the enforcement authority of food standards lies with the Municipal Councils and Pradeshiya Sabha and Regional Directors as gazette in 1999. 11 At present, H 800 from the Ministry of Health Sri Lanka, 12 which was the assessment tool used for food establishments and was developed in 2011 based on previous Food Regulations, is filled to assess the food establishments and it hardly reports naval HACCP principals and precautionary methods, which would have been critically important to prevent disease outbreaks. This study aimed to develop a food establishments assessment tool to cover all aspects of international algorithms and country food law, but it limits to one particular district of the country.
Materials and methods
The study was conducted in two components, first one was a qualitative study to develop an assessment tool for food establishments, and following the development of the tool, a descriptive cross-sectional study was conducted to assess the food establishments of the area.
Component 1: The development of FEAT was carried out to mark inspection scores for food establishments in accordance with Hygiene Regulation 1742/26 of Sri Lanka Food Regulations and several other reviewed international food safety protocols as a qualitative study. By reviewing the development of other checklists/instruments,13,14 the development of the FEAT consisted of two steps, item selection, and item presentation.
The item selection process involved the identification of items, which were considered important for the assessment of food establishments for food safety. The item selection process consisted of a comprehensive literature review of the available tools/checklists/instruments pertaining to the assessment of food establishments for their safety and in-depth interviews with selected key informants. Figure 1 demonstrates the process of material search and selection to develop a food establishment assessment tool. It describes how materials selected were excluded with reasoning at each stage and the number of materials excluded.

Schematic diagram of material search and selection.
The list of instruments 15 undertaken for the review is filed under Annexure I and selected instruments/Laws for selected 8 were filed as Annexure II.
Key informant interviews
The second activity undertaken for the item selection process was the conducting of key informant interviews. The objective of this section was to get relevant information and assess comparability with legal provisions to a checklist from individuals having knowledge and experience of food safety.
Recruitment of participants
The first key informant was selected by the principal investigator (PI) and subsequent informants were selected by a “snowballing” method. 13 The Former Deputy Director in charge of the Food Administration Unit of the Ministry of Health, Sri Lanka was the first key informant. Interviews were conducted with participants including Deputy Director (Field services) in charge of the National Institute of Health Sciences (NIHS), one tutor nominated by the Principal of the School of Public Health Inspectors in NIHS, two technical experts at field level, and legal officer reputed record on food safety laws.
(a) Conducting key informant interviews
Key informant interviews were conducted by the PI during the months of January and February 2017, using the prepared key informant interview guide. Some legal documents and documents considered to conceptualize at the time of drafting the original legal paper, for instance, the Sri Lanka Food Act, No. 26 of 1980 with its hygiene regulation numbers as 1742/26, were reviewed in depth to develop the assessment tool. A list of the documents is mentioned in Annexure II. The recruitment of new participants was stopped at the point that no additional information was received by three consecutive responders and data saturation was considered.
(b) Item presentation/construction of food establishments’ assessment tool (FEAT)
An expert committee was identified consisting of the following professionals to develop the tool further and a meeting was conducted as a focus group discussion (FGD). The focus group included the Deputy Director (Training)—NIHS, Consultant Community Physicians, a retired Assistant Director of the Food Administration Unit, a Food and Drug Inspector, a Legal Officer, Supervisory Public Health Inspector—NIHS, a Sociologist, a Tutor from the School of Public Health Inspectors, and Medical Officer of Health (MOH)—Kalutara.
Conducting FGDs
FGDs were conducted during the month of October 2018, using a pre-established methodology elaborated in detail in Annexure III. 13
Validation of the tool
Most of the statement in the food establishments’ assessment tool was in the form of a checklist. Statements were constructed to assess the food handling practices in food establishments. Some statements were taken directly from the Sri Lanka hygiene regulation, while some were modified and constructed by the PI based on literature evidence and international protocols. Statements were arranged in a way to maintain the best possible flow.
The judgmental validity of the checklist was tested on the face and content validity. The face validity of the checklist was checked by three experts in the field: Deputy Director (Field Services), NIHS, Kalutara; the Medical Officer of Food and Drug; and the Public Health Tutor. By validating active inputs from service users, who ultimately receive the outcome of the study and determine whether the checklist captures the favorable scope, the checklist can be enhanced its acceptability, relevance, and quality of the measures. The content validity of the checklist was assessed by a Consultant Community Physician and a Regional Director of Health Services (RDHS), Kalutara. By validating with the support of healthcare professionals, the checklist was covered to the extent to which the set of items comprehensively filled the different components of health to be measured. Necessary amendments were done according to the suggestions and comments received.
Pre-testing the FEAT
The tool was pre-tested among 10% of food establishments in one Public Health Inspector area, which had not been scheduled for the study and was tested for understandability, time adequacy, appropriateness of approaches used, and ability to improve their support from food handlers and food establishment owners. The tool was further amended with the results of the pre-test as a final version. The final version of FEAT was annexed as Annexure IV. After pre-testing, the FEAT had components, an assessment of the construction of the food establishment with legal conformity to food handling, an assessment of the processing area of the food establishment, an assessment of installation of overhead structures and fittings, assessment of water supply and storage, assessment of utensils and equipment using food handling, assessment of other facilities conducive with safe food handling practices, assessment of medical examination and certification, assessment of hygiene and food handling operations among food handlers, assessment of HACCP as precautionary measures, assessment on displaying and servings to customers, and assessment on responsibilities of food establishments’ owners on ensuring proper food handling practices among food handler and in food establishments.
Component 2: Final version of FEAT was employed to determine the level of good food handling practices among food handlers and in food establishments as a community-based descriptive cross-sectional study. The FEAT was transferred to a mobile app to minimize errors occurring at the time of data collection, to ease transferring data for analysis, and to define locations of food establishments by GPS mapping.
Sample size

Z21-/2 is the percentile of the standard normal distribution determined by the specified confidence level (1.96 for 95% confidence level).
p is the estimated proportion of satisfactory food handling in the study population (50% was taken as no previous studies had been done in Sri Lanka).
q is (1 – estimated proportion in study population).
No previous studies were not done similar nature, good food handling practices among food handlers is considered as (estimated proportion − p) is taken as 0.5.
d is the acceptable margin of error (0.05).
Considering the nonresponse rate of 10%, the sample size = 384/0.9 = 426.67.
The minimum sample size for the study = 427.
With reference to the 2017 statistics, RDHS—Kalutara reported a 1,014,705 total population with 1660 licensed food establishments 231 bakeries, 231 hotels and restaurants, 89 snack bars, 258 tea and coffee shops, and 312 non-categorized.
Development of sampling frame
List of business registration data from the current year to 5 years back from the register of business registration, list of tax-paying data for all business institutes/places from the current year to 5 years back from Pradesheeya Sabha tax register (this is the register maintained and updated every year to register all business institutes which earn more than 200 rupees per day), and compiled list of all business registration data related to food by District Secretary Office in Kalutara were the three sources included for the sampling frame development. Since divisional secretary areas were not overlapping field areas of MOH offices in Kalutara district, the list can be used for corresponding MOH areas.
Sampling technique
Out of the 12 MOH areas under the RDHS, Kalutara, three MOH areas were randomly selected using the lottery method, and food establishments were selected using random numbers generated in an Excel sheet from the sampling frame mentioned above.
If the food establishment selected was not opened at the time, a repeat visit was made within the other days (most probably the next day), in which data collection was conducted in a particular MOH field, and if not available after the second visit, the substitute was selected from the area corresponding to the similar type of food establishment using the similar method described in above. Food establishments that were opened during day time and licensed Food establishments were included. Exclusion criteria were food establishment owners and food handlers, who were unable to hear due to hearing defects during the time of data collection 16 and food handlers who had been working in the selected food establishments for less than 3 months. Developed FEAT was employed to determine the level of good food handling practices among food handlers and in food establishments, respectively.
Data collection
Data collection was carried out by PI from August 2018 to November 2018. Relevant MOH offices were informed prior to the data collection apart from official communication via RDHS—Kalutara. FEAT was transferred to a data collection mobile data collection application. The scoring system to categorize the level of hygiene in food establishments as good/poor was based on the final qualitative inputs given by the experts and participants (Table 2). Each item of the assessment tool was assigned to a 1–5 scale and each item contributed to the final score. Categorization of scoring was done as 1–2 as “very poor,” 2.1–3 as “unsatisfactory,” 3.1–4 as “satisfactory,” and 4.1–5 as “Good.” (The establishments that were identified as “Very poor” and “Poor” were finally included as “Poor” in the final category. The remaining food establishments that were “Satisfactory” and “Good” were added to the final category of “Good.”)
Data processing and statistical analysis
The first component consisted of qualitative data, which were presented in tables with themes. All the other quantitative data were manually checked and entered into Excel sheets.
Results
Development and validation of the FEAT
The results of the development of the FEAT are presented under the following subsections, item selection, and item presentation.
Item selection process
Selected items and comparisons were annexed as Annexure II A. Classification of the instruments, Target population of assessment, mode of administration, time taken to complete administering the instrument, scale of measurement, scoring system, and methodology of allocating scores were included for the review. Summarized findings of the review of instruments are presented in Annexure II B.
Key informant interviews and FGDs
Findings of Key Informant Interview (KII) and FGD are summarized in Tables 1 and 2. The following table describes the results of KII of FEAT by five experts involved in their qualitative contribution to developing the instrument over five domains identified before.
Summarized findings of the key informant interviews on the food establishment assessment tool.
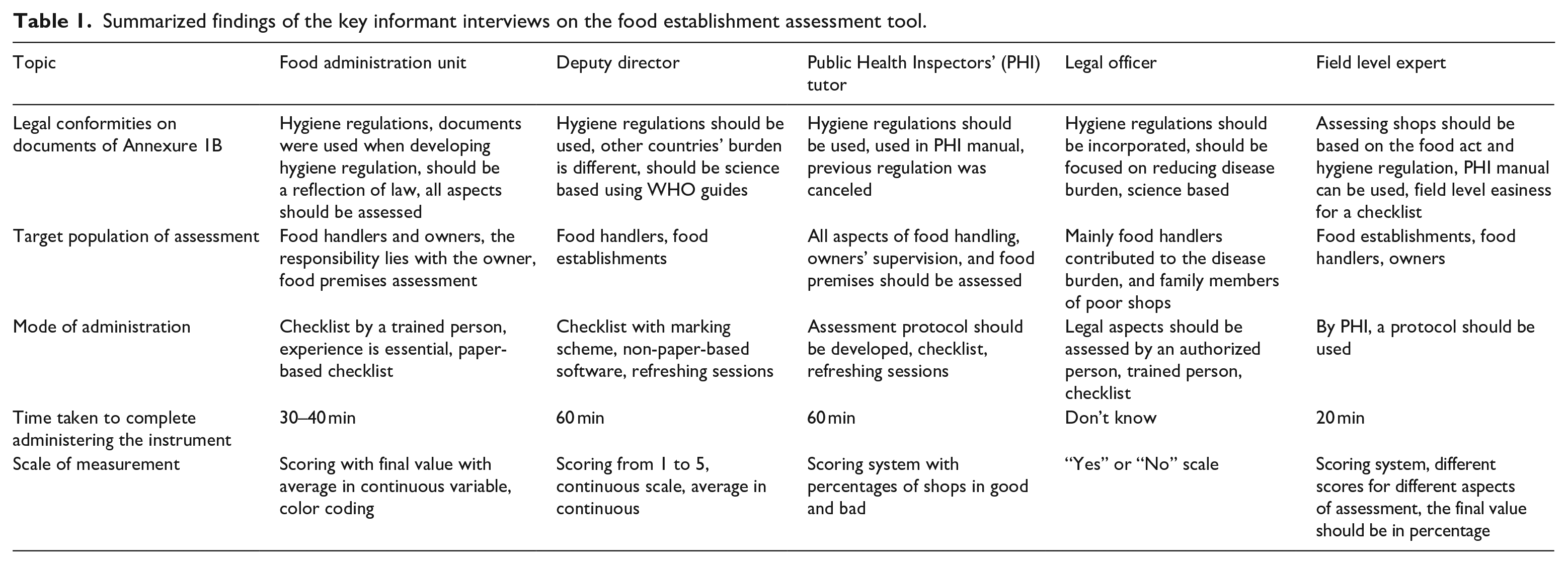
All experts conveyed, interpreted, and emphasized hygiene regulations to be used to develop FEAT and to assess food establishments and food handlers. Furthermore, four out of five reported to commence with the checklist with a 1–5 scale. Three experts showed their concern about developing a protocol to follow to administer the checklist.
Summarized findings of FGD are presented in Table 2 with experts’ opinions of nine. They contributed under six domains of FEAT to develop marking schemes and protocols.
Summarized findings of the FGD on the food establishment assessment tool.

The majority agreed to include a 1–5 scoring scale incorporating items in hygiene regulation to develop FEAT. The time to complete the checklist was listed as 30–45 min depending on the category of food establishments.
Item presentation
Several additional items found important by the FGDs were incorporated into the item list based on impact scores and keeping the flow of inspection inside and outside of the food establishments. Assessment of betel chewing by food handlers inside the premises, keeping cloths hanging near food handling area, sleeping inside the food premises by food handlers, availability of past water quality reports, checking for grade 5 food utensils, and checking of good quality raw materials was incorporated additionally to FEAT and to administration guide.
Face validity and content validity
Overall, all 12 participants expressed their satisfaction with this attempt to measure the FEAT among food establishments. Out of the 12 persons (Table 3) interviewed to assess face validity, 11 felt that overall, the FEAT did address the areas of food handling. No concerns were raised about the language of the instrument while three participants expressed their concern on the length of the instrument.
Distribution of participants by gender, ethnicity, religion, and age category.

Clarity on the themes was preserved in a way of selecting three different methods of the study via reviewing international and local protocols, conducting key informant interviews, and conducting FGDs. The study reported a predetermined group of participants to cover all aspects of food safety, using the guide for the key informant interviews and FGDs, describe and relate to the analysis, by reviewing international and best practice protocols and by the conceptualization of the assessment tool development. As the selected participants are the sample of experts in the different contexts of the food safety field, the study reported the findings are credible and transferrable. The results of the qualitative study were based on the participant’s responses and followed the developed written guides to conduct all interviews and discussions. All transcripts, notes, and audio tapes generated from KII and FGD were used for final themes/checklists, and final themes/checklists were presented to all. Dependability was assessed in 10% of the themes by the separate experts of the NIHS, Kalutara.
Following Table 4 summarized the themes generated from the qualitative assessments.
Grouping of themes generated.

Assessment of food handling practices in RDHS area, Kalutara using FEAT
According to the study, 421 food establishments were assessed, the profile of which is presented in Table 5.
Distribution of sample according to different categories of food establishments.
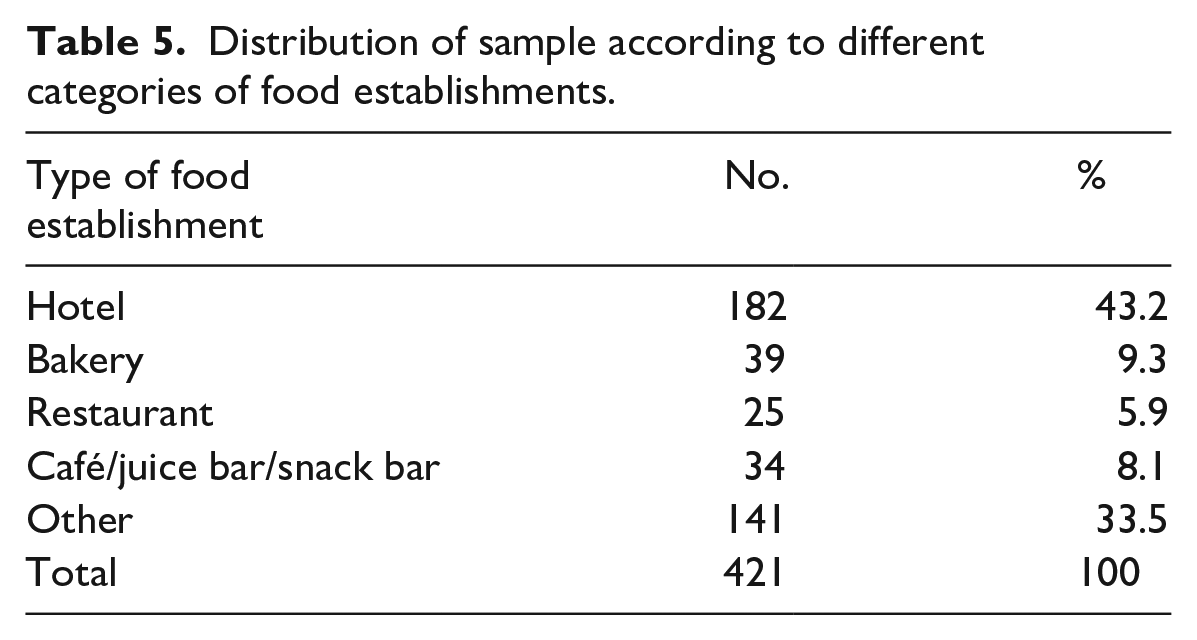
According to the data presented in Table 5, 182 (43.2%) hotels, 39 (9.3%) bakeries, 34 (8.1%) café/juice bar/snack bars, 25 (5.9%) restaurants, and 141 (33.5%) of other categories were included in the study sample.
The final summation was calculated for each MOH area for inspection score and results of which are presented in Table 7. Central tendency and measures of dispersion were mentioned after considering the distribution of inspection scores.
Table 6 describes the number and percentage of distribution of different categories of food establishments in each MOH area. The total selected from each MOH area was mentioned.
Distribution of different categories of food establishments according to MOH areas.
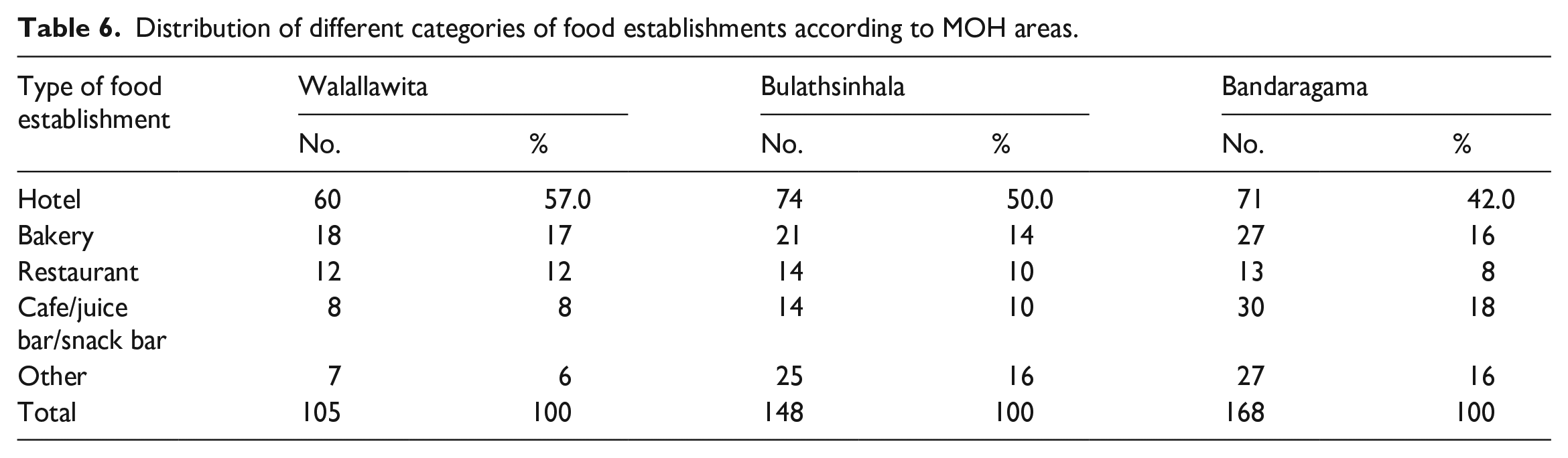
The highest percentage of hotels and restaurants was reported from the Walallawita MOH area, whereas the highest percentage of cafe/juice bars/snack bars and other shops was in the Bandaragama MOH area.
Table 7 shows the distribution of inspection scores with measures of distribution.
Distribution of inspection scores calculated using the checklist in food establishments and food handlers according to MOH areas.*
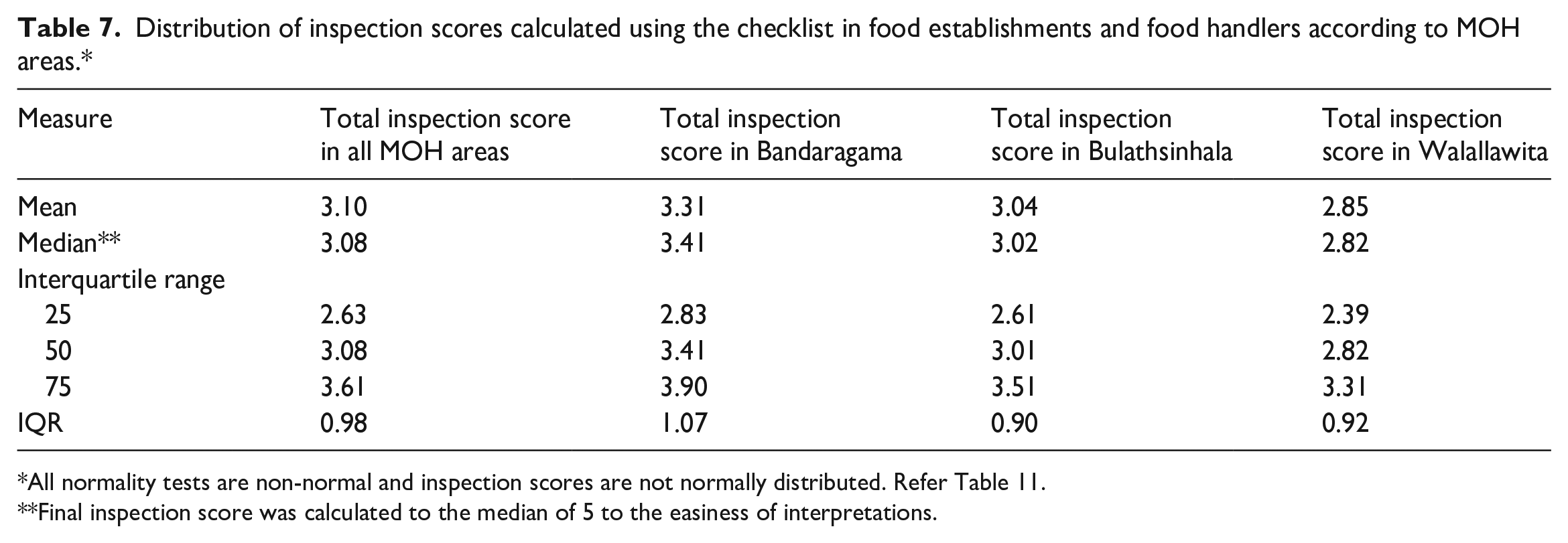
All normality tests are non-normal and inspection scores are not normally distributed. Refer Table 11.
Final inspection score was calculated to the median of 5 to the easiness of interpretations.
This table describes the distribution of the median, centiles (25,50,75), and interquartile range in all three MOH areas separately and as a whole. The food establishment assessment tool (checklist/FEAT) had 75 points to be checked and scored, but some assessment points were found not relevant to some food establishments. The median score varied from the lowest value of 2.82 in Walallawita to the highest value of 3.41 in the Bandaragama MOH area. The median value as a whole was 3.08. There were no significant differences among the three MOH areas.
Median values were calculated for all 11 main domains of FEAT according to MOH areas and results are presented in Table 8. In all, 11 domains were assessed in FEAT with different numbers of items. The number of points for each domain ranged from 2 to 14 items. The average was calculated for each domain according to MOH area in the range of a minimum score of 1 and a maximum score of 5 for each point.
Distribution of median values of inspection score calculated in food establishments and food handlers according to each component of the checklist over MOH areas.*

All normality tests are non-normal and inspection scores are not normally distributed.
All three MOH areas scored a maximum score of 5 for the domain listed as water supply and storage and a minimum score of 1 for the domains of availability of medical certification and responsibility of owners of food establishments over optimal practicing of good food handling practices in the premises. In addition, taking precautionary measures was good, but maintenance of processing area and installation of overhead structures and fitting were poor in food establishments.
The distribution of the demographic characteristics of food handlers is reported in Table 9.
Distribution of food handlers by gender, ethnicity, religion, and age category.

Average age 45.7 years, mode 45 years.
Table 10 reports the level of hygiene in food establishments over three MOH areas. Categorization of scoring was done as 1–2 as “Very poor,” 2.1–3 as “Unsatisfactory,” 3.1–4 as “Satisfactory,” and 4.1–5 as “Good”.
Distribution of hygiene levels according to MOH areas.

According to the classes defined by the expert committee and literature review, the highest percentage of food establishments (69.4%) in the “Good” category were in the Bandaragama MOH area and the highest percentage of food establishments (54.5%) in “Very poor” category were in Walallawita MOH area.
According to Table 11, the inspection score of food handlers and food establishments was assessed for normality. The visual method was used with histograms and Q–Q plots. 17 Histogram showed non-normally distributed data while the Q–Q plot (observed vs. expected values) reported non-normally distributed data with deviation away from the line, while Q–Q plot (observed vs. deviation of normal values) demonstrated similar distribution with deviation away from zero.
Distribution of skewness, kurtosis, normality tests, and normality plots of inspection score in food establishments and food handlers in the descriptive component.
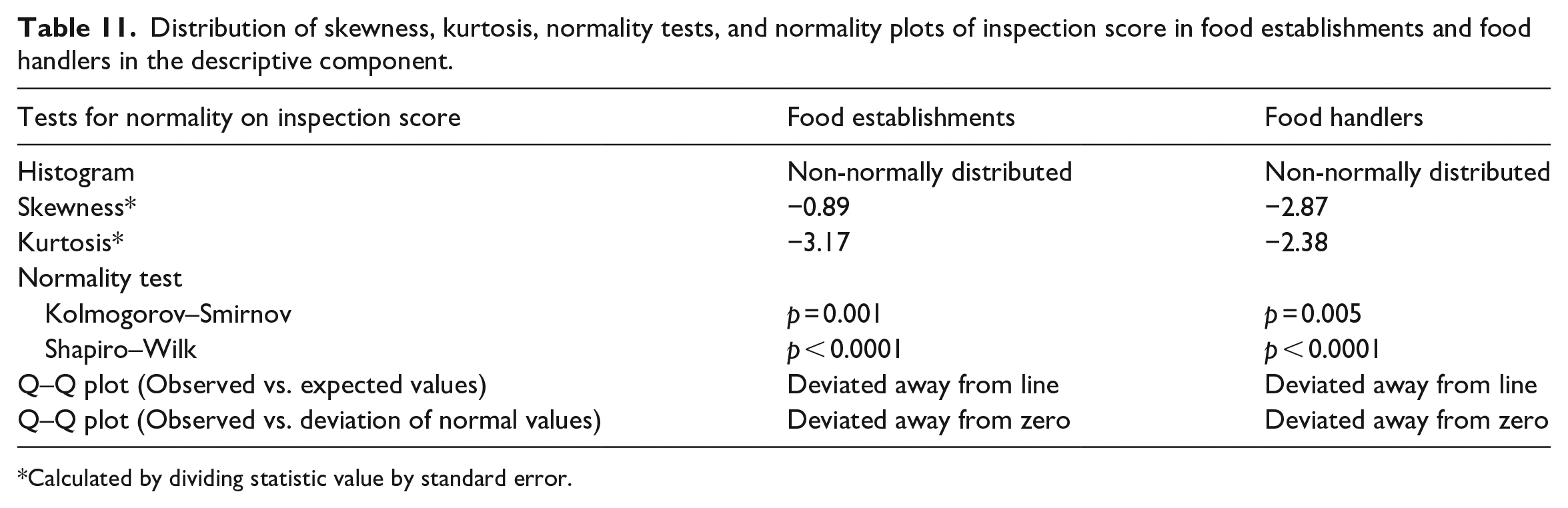
Calculated by dividing statistic value by standard error.
Skewness and kurtosis values greater than +2.58 were significant at p < 0.01. 18 Both inspection scores showed the value is greater than 2.58 and both of them were non-normally distributed.
The normality tests are supplementary to the graphical assessment of normality. The main tests for the assessment of normality are Kolmogorov–Smirnov (K-S) test and Shapiro–Wilk test. 17
A Shapiro–Wilk test was conducted to determine whether inspection scores of food handlers and food establishments could have been produced by a normal distribution. 19 The results of the Shapiro–Wilk test were significant, with p < 0.0001 for both inspection scores. These results suggested that the inspection score was unlikely to have been produced by a normal distribution; thus normality cannot be assumed.
K-S test was used to assess whether the distribution of inspection scores was met with normality. The result of the K-S test was significant, p = 0.001 and p = 0.005, indicating that the assumption of normal distribution was violated.
Discussion
Modern food safety measures have prevented morbidities and prolonged the onset of mortalities, whereby the level of unsafe food in a global context has decreased exponentially over the last decades. Although we have been able to adapt many new food safety measures to our system, we have not been as successful in our attempts at improving and implementing at the ground level. 20
In the first component of the study, a food assessment tool for the food establishments was developed and validated following a review of legal and international documents, key informant interviews, and FGDs similar to the methodology used by De Silva et.al., 13 The interviewer guide tool was pilot-tested in 10% of the population and it would be a limitation for the study. Considering the nature of the target population, a balance was reached between the desire to have a comprehensive, brief, and practical instrument, since a study done among canteens of schools in the Colombo municipal council area showed 100% non-availability of H 800 (food establishment assessment tool of Sri Lanka at present), which has been used as a food safety assessment tool and method of educating food handlers in the current context of the country. 21 Food establishments’ assessment checklist in Brazil based on their regulations and restaurant assessment protocols in Florida agreed with the FEAT (Annexure II A) and FEAT contained many domains which are not present in H- 800 such as details related to medical certification, precautionary measures, and the responsibility of owners to train food handlers. An instrument to be used in the community needs to be easily administered and easily coded and easily scored. The FEAT uses simple summation within the domains, and the domains being transformed into a scale of 0–5 has further simplified the FEAT. Protocols for food handling practices in food establishments and food handlers essentially need to be aligned with the legal acts of the respective country referring to the global and local scientific food safety codes. The FEAT measures food handling practices according to international codes and regulations of the user’s country.
Lacking medical certification and proper supervision by owners/managers with training for food handlers are markedly alarming in the study compared to the systematic review and meta-analysis of Tadele et al., 22 and Tamene et al. 23 The study further reported the parallel findings emphasizing the management’s responsibility for enhancing food handlers’ knowledge and increasing training and supervision on food safety practices. 24
Since the study was limited to three MOH areas of Kalutara RDHS, the findings may not be generalized to the total population of the country and all districts. Street food vendors might be the worst sample of sociodemographic and economic status and might be different in relation to food handling practices over food establishments. So, that was not reflected in the study.
Conclusion
The developed and validated FEAT was used to assess food handling practices in food establishments and among food handlers with 11 domains with 75 items and more than 100 assessment points. It is a completely valid instrument for food establishments and its nature of easy administration supports reliable assessment.
Overall food handling practices of food establishments in the Kalutara RDHS area following assessment with FEAT were in the “satisfactory” category, though future directions and recommendations are required to improve the subsections of medical certification of food handlers and to ensure the supervision of food handlers by owners/managers of the establishments.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231196009 – Supplemental material for Development of a food handling practices assessment tool based on the Sri Lanka food regulations
Supplemental material, sj-docx-1-smo-10.1177_20503121231196009 for Development of a food handling practices assessment tool based on the Sri Lanka food regulations by Lasantha Krishan Hirimuthugoda, Padmal De Silva, Palitha Abeykoon, Sameer Altaf Tunio and Hasadari Pamoda Madarasinghe in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231196009 – Supplemental material for Development of a food handling practices assessment tool based on the Sri Lanka food regulations
Supplemental material, sj-docx-2-smo-10.1177_20503121231196009 for Development of a food handling practices assessment tool based on the Sri Lanka food regulations by Lasantha Krishan Hirimuthugoda, Padmal De Silva, Palitha Abeykoon, Sameer Altaf Tunio and Hasadari Pamoda Madarasinghe in SAGE Open Medicine
Footnotes
Acknowledgements
First, the authors acknowledge the National Institute of Health Sciences, Kalutara for giving us an ethical clearance letter and writing a support letter for the study area. Second, our gratitude goes to the Regional Director of Health Services, Kalutara. Last but not least, the authors thank all the respondents for their voluntariness and participation.
Author contributions
L.K.H. contributed to the conception and design of the work and the training of data collectors and to supervising the overall data collection process. L.K.H. and P.D.S. contributed to the data entry, analysis, and interpretation of the data. L.K.H. and P.D.S. wrote the manuscript. P.A., S.A.T., and H.P.M. reviewed the manuscript and contributed to the final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Research Ethics Committee of the National Institute of Health Sciences, Kalutara. The ethical approval number of the study was NIHS/ERC/18/65.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Self-funded.
Informed consent
We obtained informed written consent from the study subjects whose age is 18 years and above. Just the data were collected simply by interviewing and observation.
Availability of data and material
The data underlying the results presented in the study are available from the corresponding author upon a reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.