
Abstract
Objectives:
Improper food handling contributes to many foodborne diseases and food outbreaks globally leading to witnessed morbidities and mortalities. The study aims to develop an educational package and participatory consumer groups to improve food handling practices among food handlers and in food establishments in the Regional Director of Health Services area, Kalutara, Sri Lanka.
Methods:
The study developed an educational package and participatory consumer groups to improve the food handling practices among food handlers and in food establishments. The critical knowledge gaps were identified during the first component of this study, which was conducted as a descriptive study, and the findings were further discussed in the Focus Group Discussion. Posters, info sheets, and workshops were used for educational packages, and four consumer groups were formed. The second component of the study following the development of the interventions was continued as a three-arm, non-randomized controlled community trial for 4 months in the Regional Director of Health Services, Kalutara.
Results:
The educational package for food handlers was introduced as a package of a workshop, info sheets, posters to display at workplaces, and short refresher training two weekly to direct good food handling practices in food establishments. Consumer groups were strengthened to exercise their legal rights on their purchases and the ratings showed improvements in the hygiene levels with repeated consecutive visits.
Conclusions:
The novel educational package and participatory consumer groups are designed and implemented to improve food handling practices among food handlers and in food establishments.
Keywords
Introduction
Food handling is inevitably involved with food preparation and consumption, and many developing countries operate with manpower for manufacturing, packaging, and distributing. Consequently, a major proportion of practical notions of food safety are entangled with food handling practices everywhere. Improper food handling, preparation, and storage can result in food contamination leading to food poisoning and food-related diseases caused by intestinal parasites and pathogenic bacteria. 1 Food handler means any person who directly handles packaged or unpackaged food, food equipment, utensils, or food contact surfaces and is therefore expected to comply with food hygiene requirements. 2 Food handlers play a major role in ensuring food safety throughout the chain of production, processing, storage, and preparation of food in food establishments. Many of these good practices and norms were stipulated and legally complied with food codes and regulations of the countries in the world.
Food hygiene training is vitally essential to minimize the potential threats and hazards posed by food and to ensure the safety of food consumed, as 97% of food-borne diseases occur due to the malpractices of food handlers in food establishments. 3
Any food safety training program for food handlers should include content defining awareness and responsibilities, regular instruction and supervision, and periodic updates with refresher training.4,5 A review provided evidence of the effectiveness of food handler training programs, in conjunction with certification, to improve the knowledge and practices of food handlers. 6 The results of the meta-analyses confirmed the efficacy of food safety training for increasing knowledge and improving attitudes about good hand hygiene and should be incorporated into the refresher training. 7
Many countries, where human rights and free trade prevail, apart from legal frameworks and their legislatures, work closely with a significant number of reputed consumer groups as public movements to protect consumer rights and norms. In Sri Lanka, consumer rights movements are operating on a small scale to fight for consumer rights, and hardly empower consumers individually to strengthen their knowledge and awareness of their rights on their purchases. However, provisions of the Consumer Affairs Authority Act of Sri Lanka clearly state the creation of informed groups of the public as consumer organizations, to promote, assist, and encourage their rights on purchases. 8 There are fewer research studies and gaps of new knowledge on developing packaged training to educate food handlers/managers in improving food safety and developing consumer groups to strengthen consumers toward their influence in improving food handling practices. Hence, the present study is designed to develop educational packages and participatory consumer groups to improve food handling practices among food handlers and in food establishments.
Methodology
Development of educational package
An educational package was designed targeting food handling practices among food handlers and owners of food establishments in the Regional Director of Health Services area, Kalutara, Sri Lanka, and the intervention was implemented to the target group through the Medical Officer of Health. The intervention was designed based on,
Sri Lanka Food Regulations—Hygiene Regulations. 9
Findings of the Descriptive Study. 10
From a review of literature on methods of changing food handling practices through educating food handlers.
Supervision and guidance of project supervisors.
An expert committee including the facilities of the Health Education Teaching Unit of the National Institute of Health Sciences—Kalutara, the help of field staff of the National Institute of Health Sciences—Kalutara, and the Regional Director of Health Services Kalutara.
Figure 1 presents two different phases of the study.

Schematic presentation of phases 1 and 2 and components.
Conducting focus group discussions
Focus group discussions were conducted during October 2018, using a pre-established methodology elaborated in detail in Annexure 1. The venue, dates, and time for the discussions were fixed on mutual agreement between the principal investigator and the participants. In selecting a venue, consideration was given to accessibility, surrounding environment, seating facilities, ventilation, etc. The Focus Group Discussions were conducted by the principal investigator with the assistance of registrars at the National Institute of Health Sciences, Kalutara. On average, a group discussion lasted around 120 min. The discussion of each item was stopped at the point that no additional information was received by three consecutive responders and data saturation was considered.
Development of the educational package
According to most of the available literature, displaying posters, handing over leaflets, and conducting workshops with refresher training to the food handlers were the measures, that showed higher effectiveness and efficiency over improved food handling practices.7,11,12 Content and designing of posters, educational info-sheets, the content of the workshop, and refresher training every 2 weeks were finalized with Focus Group Discussion and project supervisors based on the Sri Lanka Food Regulations.
Development of participatory consumer groups
Consumer groups were formed to improve food handling practices in food establishments in the Kalutara, Regional Director of Health Services area by strengthening consumers on their right to have safe food. Participatory consumer group intervention had four components, formation of consumer groups for each Public Health Inspector’s area in the Medical Officer of Health—study Medical Officer of Health area, where participatory consumer groups was planned to be implemented, had four Public Health Inspector areas, development of a consumer rating tool to score food establishments—self-inspection checklist (Annexure 2), development of Standard Operating Procedure for consumer groups to use at the time of operation (Annexure 3), and development of a general evaluation form (as back-review) for owners/managers of food establishments to review consumer groups’ operations at their premises (Annexure 4).
Consumer group acted according to the developed Standard Operating Procedure as mentioned below. After they visited the food establishment, they marked the hygiene level as they perceived it during their period at the food establishment. After the consumer group marked their consumer rating tool, the score was informed officially to the owner/manager of the food establishment. Each component gave a separate mark and the final mark was formulated in percentages. 13
Developing consumer groups
Ten consumers were selected for each group and similar types of groups were formed in all Public Health Inspector areas of one Medical Officer of Health area, which was randomly selected. Groups were educated on Sri Lanka Food Regulations, developed Standard Operating Procedure, and work they had to carry out with consumer rating tools. Consumers, who owned any type of business, especially food-related businesses, and consumers, who are working in the Department of Health, departments related to veteran services or civil protection were excluded from the study.
Designing the consumer group feedback profile
Owners/managers and food handlers of food establishments in participatory consumer groups were informed about the marks in percentages by categories of hygiene at the end of the visit. The visiting session took place for 3 months for the consumer groups. The consumer group continued with four visiting sessions in 3 months. They spent at least 30 min on average in one food establishment for marking consumer rating tool. Training sessions were conducted at the respective Medical Officer of Health office, and refresher training was continued monthly to have consistency.
Pretesting the educational package and consumer groups
The developed posters, info sheets, and workshop sessions were reviewed by the project supervisors and corrected for the pre-testing. The package was pre-tested among 5 food establishments (hotel = 2, bakery = 1, restaurant = 1, other = 1) for 6 weeks in a different Public Health Inspector’s area and was tested for understandability, time adequacy, and appropriateness of training approaches used.
Interventions were implemented as a non-randomized controlled-community trial in three Medical Officer of Health areas of Kalutara district, Sri Lanka. Implementation of the educational package was conducted as described in Annexure 5. Day sessions, displaying of posters, distribution of info-sheets, and refresher sessions at their establishments were carried out as planned. The table of visited food establishments at the end of the intervention study during the 3-month review was attached as Annexure 6. Four consumer groups were designated to four Public Health Inspector’s areas in the study Medical Officer of Health area.
Results
Table 1 describes the distribution of the participants.
Distribution of participants by gender, ethnicity, religion and age category.

Findings of the Focus Group Discussion are reported in Table 2 after meeting with the expert committee on content, review of results of descriptive component, and implementation of the educational package.
Summarized findings of the focus group discussion on educational package.

Following the results of the descriptive phase, important items, to be included in an educational package were determined. Several important deficits of knowledge, but critical errors at the time of food handling were further elaborated. For example, storing items in the refrigerator and storing critical items like milk, meat, fish, and fast-food items that contained fish and meat, lack of medical certification, betel chewing while food handling, and keeping the premises unclean were identified as having areas of poor knowledge, but those were serious deficits related to the handling of food products. Based on that, workshops and banners were further created to address optimal information.
A finalized set of posters was presented on a small scale as shown in Figure 2. Info sheets, the content of the workshop, and the PowerPoint presentation of the lecture were developed. Lectures on food handling practices were delivered by a student tutor of the School of Public Health Inspectors, who was experienced in training, education, and field-level work for more than 15 years. It was a PowerPoint presentation in the Sinhala language for 30 min with many photos and videos on incorrect food handling practices and about storing items. The questions and answers session were conducted after the lecture. Practical sessions were done to train on how to store the food in refrigerators correctly, to handle food storing cases, and to do hand washing practices. Each station was conducted as a live station with the support of field staff for 15 min each.

Sample of posters distributed as the one component of the educational package.
The findings of Focus Group Discussion related to the development of participatory consumer groups are presented in Table 3. Most of them were females who consented to be a member of consumer groups.
Summarized findings of the focus group discussion on participatory consumer groups.

Both sub-domain scores and final scores were improved over time (Table 4). Using a consumer rating tool, the consumer groups assessed the food establishments by giving marks to each tool sub-domain and calculating final percentages. The sub-domain of “general condition of the establishments” increased from 20% to 70% of food establishments. However, the sub-domain of “responsibilities of owners of food establishments” was not improved accordingly.
Final percentages given at the end of each visit for food establishments by consumer groups for each item considered for inspection over their four visits.
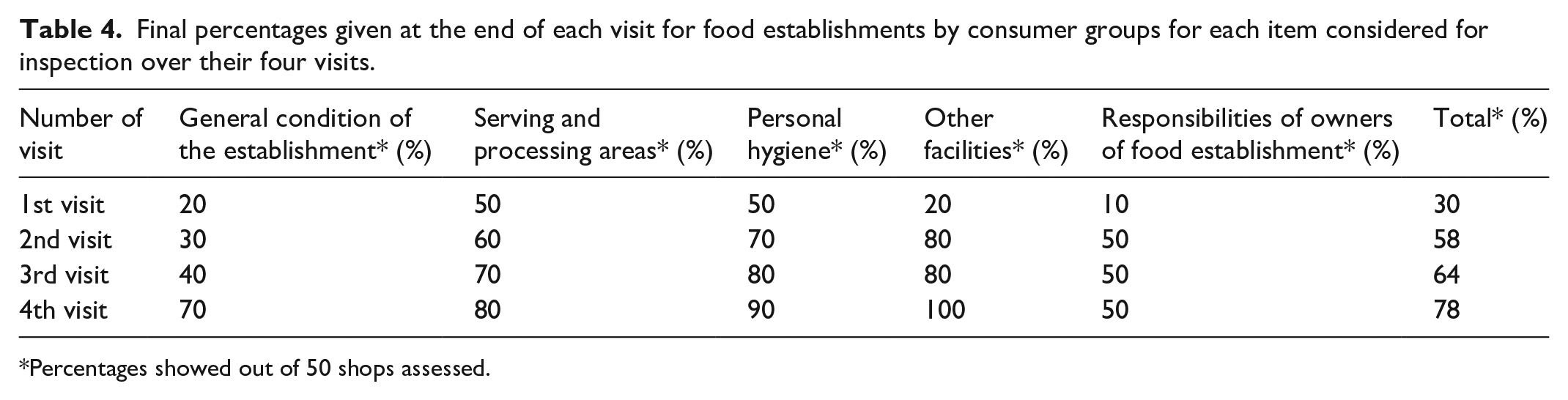
Percentages showed out of 50 shops assessed.
Table 5 shows the results of the assessment conducted by owners/managers of food establishments over consumer groups during their visits. Owners evaluated the consumer groups on their fair and reasonable conduct over assessments.
Final percentages of evaluation by owners/managers of food establishments at the end of each visit of consumer groups in domains over their four visits.

Out of 40 members of four consumer groups’ behavior and conduction were assessed.
Assessments of consumer groups were counter-assessed by the owners of food establishments to find any bias over each assessment and the overall conduction of the rating. Almost every domain in the general evaluation form demonstrated more than 80% marks for consumer visits and provided a fair rating by the consumer group.
COREQ (COnsolidated criteria for REporting Qualitative research) Checklist is attached as Annexure 7.
Discussion
Developing community interventions for improving food safety is very challenging. This study had a descriptive component to learn the pronounced knowledge deficits of food handlers and unattended critical hazards of food establishments. With this knowledge, the study developed two interventions, named educational package and participatory consumer groups after concurrences of Focus Group Discussion. Two interventions were conducted as a three-arm controlled trial—control, educational package intervention, and participatory-consumer group intervention, for 50 food establishments each. While the educational package included workshops, refresher training, presentations, and posters, participatory consumers continued with the Standard Operating Procedure, checklist, and the back-assessment of consumer groups by owners of food establishments.
Studies showed that lack of knowledge on storing food, obtaining medical certification for food handling, and maintaining temperature-sensitive foods were at alarming levels. Concordant to refresher training in this study, Park et al. 12 concluded that practicing continual and repetitive food safety behavior with repeated use of training material could be effective in maintaining knowledge and practice. Including posters and information leaflets to train food handlers was proved effective in many other studies,7,14 and the best practice for effective training of food handling programs was the food safety interventions, which addressed exact and pre-identified deficits of knowledge and skill. 11
This one part of the educational package was conducted as short-duration training followed by refresher training with a maximum of 2 weeks gap between two sessions. A study done with a similar methodology showed agreement with our study as a key feature of an effective training program for improved food safety practices in Nigeria. 15 Meta-analysis further confirmed and was consistent with study findings that the efficiency of food safety training – combined with refresher sessions, which was a part of the health educational package of this study, was increasing knowledge and attitudes about good food hygiene. 7
Consumer feedbacks play a pivotal role in influencing the food market related to international marketing fields. Concerning the thesis of Herath, 16 the majority of consumers (97.4%) and food handlers (96.6%) admitted the general need for food safety activities, and 93.2% of consumers and 79.8% of food handlers admitted that these activities need to be carried out as a preventive measure. Further thesis explained that a high percentage of respondents admitted that food safety is a problem that warrants high priority though correspondingly less priority is being given. Consumer rating systems are currently being engaged in many fields like international tourism, international aviation, international health tourism, international hotel booking systems, etc. Consumers are requested to participate voluntarily after consuming the product or service. To make it realistic, consumers should be empowered adequately and timely about the standards, quality, and legal requirements entangled with the products and services they claim. In participatory consumer groups, selected food establishments were visited by a group of consumers who acted according to Standard Operating Procedure and training given, monthly for up to four visits.
Rating of the services and products represented a key method of assessment of consumer perceived satisfaction. Verbal rating, pencil-and-pen rating, online rating, and telephone surveys were used in many studies on consumer assessments. The rating method of this study was in agreement with the five-star rating method analyzed in the hospital consumer system by Mayo Clinic, USA, 17 but discordant with the verbal rating method of a study done among Japanese consumers. 18 Both methods rated by consumers, demonstrated improved outcomes of the system.
Limitations
The study had an adequate and larger sample size (n = 50) to reduce the beta error of the trial. Since the development of the interventions was done in one particular district of Sri Lanka, the findings may not be generalized to the total global population. The researcher took several measures on monitoring while implementing the research study such as weekly reminders to consumer groups via telephone calls, keeping a mobile phone number dedicated to the research for clarification, monitoring the intervention through the Public Health Inspector and Medical Officer of Health, and reminding owners of food establishments in participatory consumer groups on an evaluation form upon consumer groups. The repeated questioning on intervention may synergize the effect of the intervention. Implementation of participatory consumer groups, which has some legal influence when conducted through the general public may have encountered several limitations such as: overreacting to the offenses at food establishments and misinterpretation of advice as given in Standard Operating Procedure. Yet, this will not have a large effect on the results. Both interventions were limited to a few months and the sustainability of interventions was not evaluated in the current study.
Conclusions
Educational packages and participatory consumer groups would be doable holistically to population-level food safety concerns.
Encouraging consumers to be responsible for their purchases by developing consumer groups and regular training is challenging and does appear to provide significant realistic benefits.
Recommendations
A targeted educational package to address exact pre-identified knowledge gaps would be the next level of advancement with additional benefits compared to routine educational pieces of training.
Consumers need to be aware and, be collective as groups to improve food safety at the population level.
Further initiation with the support of relevant authorities is necessary to have collective improvement.
Supplemental Material
sj-doc-2-smo-10.1177_20503121241234009 – Supplemental material for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka
Supplemental material, sj-doc-2-smo-10.1177_20503121241234009 for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka by Lasantha Krishan Hirimuthugoda, Padmal De Silva and Palitha Abeykoon in SAGE Open Medicine
Supplemental Material
sj-doc-3-smo-10.1177_20503121241234009 – Supplemental material for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka
Supplemental material, sj-doc-3-smo-10.1177_20503121241234009 for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka by Lasantha Krishan Hirimuthugoda, Padmal De Silva and Palitha Abeykoon in SAGE Open Medicine
Supplemental Material
sj-doc-5-smo-10.1177_20503121241234009 – Supplemental material for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka
Supplemental material, sj-doc-5-smo-10.1177_20503121241234009 for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka by Lasantha Krishan Hirimuthugoda, Padmal De Silva and Palitha Abeykoon in SAGE Open Medicine
Supplemental Material
sj-docx-1-smo-10.1177_20503121241234009 – Supplemental material for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka
Supplemental material, sj-docx-1-smo-10.1177_20503121241234009 for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka by Lasantha Krishan Hirimuthugoda, Padmal De Silva and Palitha Abeykoon in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121241234009 – Supplemental material for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka
Supplemental material, sj-docx-4-smo-10.1177_20503121241234009 for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka by Lasantha Krishan Hirimuthugoda, Padmal De Silva and Palitha Abeykoon in SAGE Open Medicine
Supplemental Material
sj-docx-6-smo-10.1177_20503121241234009 – Supplemental material for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka
Supplemental material, sj-docx-6-smo-10.1177_20503121241234009 for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka by Lasantha Krishan Hirimuthugoda, Padmal De Silva and Palitha Abeykoon in SAGE Open Medicine
Supplemental Material
sj-docx-7-smo-10.1177_20503121241234009 – Supplemental material for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka
Supplemental material, sj-docx-7-smo-10.1177_20503121241234009 for Development of educational package and participatory consumer groups to improve food handling practices in food establishments in Sri Lanka by Lasantha Krishan Hirimuthugoda, Padmal De Silva and Palitha Abeykoon in SAGE Open Medicine
Footnotes
Acknowledgements
First, the authors acknowledge the National Institute of Health Sciences, Kalutara for providing all human resources and technical support. Second, our gratitude goes to the Regional Director of Health Services, Kalutara. Last but not least, the authors thank all the respondents for their volunteering and participation.
Author contributions
L.K.H. contributed to the conception and design of the work and to the training of data collectors and to supervising the overall data collection process. L.K.H. and P.D.S. contributed to the data entry, analysis, and interpretation of the data. L.K.H. and P.D.S. wrote the manuscript. P.A. reviewed the manuscript and contributed to the final approval of the version to be published.
Availability of data and material
The data underlying the results presented in the study are available from the corresponding author upon a reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Self-funded.
Ethical approval
Ethical approval for this study was obtained from the Research Ethics Committee of the National Institute of Health Sciences, Kalutara, Sri Lanka—NIHS/ERC/18/65.
Informed consent
We obtained informed written consent from the study subjects whose age is 18 years and above. Just the data were collected simply by interviewing and observation.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.