
Abstract
Background:
A stroke is a sudden loss of blood supply to the brain, leading to permanent tissue damage caused by embolism, thrombosis, or hemorrhagic events. Almost 85% of strokes are ischemic strokes.
Objective:
To assess the incidence of mortality and risk factors among adult stroke patients in public hospitals of Jigjiga town, Somali Region, Ethiopia.
Methods:
An institution-based retrospective cohort study was conducted from 25 May to 15 June 2022 at Sheikh Hassen Yabare Referral Hospital and Karamara Hospital. Data were entered using Epi-Data version 4.3 and exported to be analyzed using SPSS 20 statistical software. Kaplan-Meier was used to estimate mean survival time, and a predictor with a p-value < 0.05 was considered to have a significant in multivariate Cox regression.
Results:
About 480 stroke patients’ charts were included in this study; among those, 229 (53.3%) were male stroke patients, and 259 (60.2%) had an ischemic stroke. The overall incidence rate was 7.15 deaths per 1000 person-day observations. The overall median survival time for adult stroke patients was 120 days. GCS level b/n 3–8 has a lower survival time with a mean survival time of 57 days (95% CI: 48.8–66.7) as compared to those who had GCS level 9–12 with a mean survival time of 103 days (95% CI: 93.4–112.9). Age ⩾ 71 (AHR = 1.9; 95% CI: 1.02–3.45), presence of pneumonia (AHR = 2.7; 95% CI: 1.52–4.63), and history of hypertension (AHR = 2.07; 95% CI: 1.08–3.89) were the predictors of mortality among stroke patients.
Conclusion:
According to the findings of this study, the incidence of mortality was high, at 7.15 per 1000 person-years. The presence of pneumonia, decreased GCS, age ⩾ 7, and history of hypertension were predictors of mortality in adult stroke patients.
Introduction
Background
The World Health Organization describes a stroke as a rapidly developing clinical symptom of focused (or global) impairment of cerebral functions that lasts longer than 24 h or results in death and has no obvious cause other than the vascular origin. 1 An ischemic stroke and a hemorrhagic stroke are two types of strokes. The brain’s blood supply is usually disrupted or diminished. 2 Stroke is a multi-factorial disease with a large number of factors. Hypertension, diabetes, heart failure, the human immunodeficiency virus, and increased red blood cells (RBCs) are all risk factors for stroke; symptoms of stroke include facial palsy, cognitive impairment, hemiplegia, loss of consciousness, and vision loss.1,3
According to the latest global burden of disease report, globally, there were 11.9 million new stroke cases, and almost one in eight deaths worldwide (12%, 6.5 million deaths) were attributable to stroke, whereby stroke takes a life every 5 s, making stroke the second leading global cause of death. 4 Stroke is the second-top cause of death beyond the age of 60 years and the fifth-leading cause of death in people aged 15–59 years old in the world. In China, about 2.4 million people have a new stroke each year. 5
In the latest update on stroke mortality by the WHO, it is reported that the highest rate of stroke mortality is represented by middle- and low-income countries. 6 In industrial countries, the in-hospital stroke fatality rate is 3%–11%. 7 Studies from underdeveloped countries, however, varied from 7% to 15%. 8 According to the recent reports of the Global Burden of Disease study, cerebrovascular diseases rank as the second primary cause of death, next to ischemic heart disease. 9 Although the incidence in developed countries has shown a 42% reduction, the incidence in low-income countries has shown a 100% increase. 10 Stroke rates have risen dramatically in sub-Saharan Africa over the last 20 years. It is currently the top cause of death, disability, and dementia in this region, just like other non-communicable diseases. 11 Infectious diseases are the main concern of the healthcare system in sub-Saharan Africa. As a result, there are insufficient resources to prevent or cure non-communicable disorders, such as stroke. Stroke care in this region is very inadequate. 12
Its incidence has increased in East Asia and sub-Saharan Africa. 13 With at least six Africans having a stroke every minute, Africa appears to be the global capital of stroke, and rates in Africa vary widely, from 15 per 100,000 in Ethiopia to 963 per 100,000 in Egypt and 1460 per 100,000 in the Niger Delta. 14 According to the latest data published in 2017, stroke deaths in Ethiopia reached 39,571, or 6.23% of total deaths. The age-adjusted death rate of stroke accounts for 89.82 per 100,000 populations. 15 Stroke is becoming more common in Ethiopia, accounting for 7.5% to 19.3% of hospital admissions and about 11%–42.8% of deaths between 2014 and 2019. Sudden mortality and sadness (12.4%–42.9%) were among the stroke outcomes. 16
Stroke has emerged as a significant contributor to morbidity, mortality, and long-term impairment in Ethiopia. 17 Ischemic and hemorrhagic stroke prevalence varies by region and time. In contrast, previous hospital-based research in Ethiopia found that stroke patients in Ethiopia suffer at a young age and have a higher proportion of hemorrhagic strokes than ischemic strokes. 18 The rising prevalence of stroke in Ethiopia is posing a challenge to the healthcare system. Resources for stroke treatment and rehabilitation are in short supply. 19 Hypertension, diabetes, heart failure, HIV, and increased RBCs are risk factors for stroke. 1 Various studies conducted globally have indicated that age, sex, smoking, limited physical activity, obesity, alcohol consumption, non-adherence to antihypertensive medication, uncontrolled blood pressure, diabetes, and high cholesterol are risk factors for stroke. 20
In Ethiopia, the mortality rate rose with age (15–34 years: 1%, 35–54 years: 7%, 55–74 years: 16%, >74 years: 18%). In an Ethiopian study on stroke mortality, 11% of patients at Felege Hiwot Referral Hospital in Bahir Dar died 21 in Shashemene Referral Hospital 13.3% 22 and TASH (19.2%). 23 Even though recently Ethiopia’s federal minister of health (FMOH) focused on non-communicable diseases (NCD), including stroke. 24
As a result, chronic diseases have risen to prominence as major global public health issues, particularly in poorer nations. Like Ethiopia, however, there is inadequate research on determining the incidence of death among adult stroke patients in public hospitals in Jigjiga town, Somali Region, Ethiopia, which is the purpose of this study, and no study has been done in this area. This study will be valuable evidence for stroke patients’ hospitals and the Somali Regional Health Bureau in determining the burden of stroke and its determinants, as well as planning suitable stroke prevention strategies.
Methods and materials
Study area and period
The study was conducted in Jigjiga town, which is located 638 km from the capital city of Addis Ababa. There are five governmental health institutions (2 health centers and 3 hospitals) that provide services for the town and surrounding population. Sultan Sheik Hassen Yabare Referral Hospital is one of the largest health institutions in the eastern part of Ethiopia. The hospital is under the management of Jigjiga University to serve as a teaching hospital. In addition to teaching, training, and research, SSHYRH is expected to cover an estimated population of more than 7 million people living in all zones and districts of the region, the neighboring district of Oromia, and a large part of the neighboring country of Somalia. The hospital has around 342 beds, intensive care units, pharmacies, radiology departments, and clinical laboratory facilities. Since the hospital is part of Jigjiga University’s Medicine and Health Science College, it has a residential program for students on an annual basis.
Karamara Hospital is one of the oldest hospitals in the Somali region, currently serving as a general hospital for the surrounding areas of the Somali Regional State. The hospital was built in 1960–1970 G.C. The size of Karamara Hospital is 21,706 m2. Karamara was the first hospital built in town, and it is a governmental hospital in Jigjiga, Ethiopia. The data was collected from 25 May to 15 June 2022, in SHYRH and Karamara hospitals in Jigjiga, Ethiopia.
Study design
An institution-based retrospective cohort study was conducted.
Source population
All adult stroke patients who were admitted to Sheikh Hassen Yabare Referral Hospital and Karamara Hospital from January 2019 to December 2021
Study population
All selected adult stroke patients who have been admitted to SHYRH and Karamara hospitals from January 2019 to December 2021.
Inclusion criteria
All adult stroke patients with ischemic stroke or hemorrhage stroke confirmed by computed tomography (CT) scan or magnetic resonance imaging (MRI) were included.
Exclusion criteria
The stroke patients with incomplete charts and missing stroke patient chart records during the data collection period were excluded.
Sample size determination
The sample size was determined using a two-population proportion formula using Epi Info version 7.2.2.6 software, with the assumptions of a two-sided significance level (α = 5%), power (1−β) = 80%, a 95% confidence level, and a ratio of non-exposed to exposed (R) of 1:1. Accordingly, the sample size was calculated for each specific objective; the second specific objective provides the largest sample size, with an AHR of 1.66% for non-exposed subjects and an outcome of 16.9% 25 and the final sample size become 430.
Sampling technique
Stroke patient MRN was taken from the HMIS database. The total number of adult stroke patients admitted to SHYRH and KH from January 2019 to December 2021 was 810. We have found the number of admissions for each year. The samples were proportionally allocated for each year, and with systematic sampling, the study participants for each year were selected. First, we number the units of each year on the frame from 1 to N (N = total admission of each year), and then we determine the sampling interval (K) by dividing the number of units in the population by the desired sample size of each year (n = sample size of each year). K = 810/430 = 2.
Data collection methods
Using standardized tools, all information was taken from patient charts. The checklist was adapted and modified from different related studies and then organized according to the objectives of the study. Five data collectors who are nurses in their profession and work in facilities other than the study area collected the data; one supervisor per hospital with a master’s degree was assigned. Study patients’ data were extracted from the hospital’s in-patient department admission and discharge register, which contains patients’ demographics, MRN (a medical record number), admission and discharge dates, and HMIS diagnoses.
Study variable
Dependent variable
Stroke mortality (death, censored).
Independent variable
Socio-demographic characteristics of adult stroke patients: age, sex, educational status, occupational status, ethnicity, residence, and marital status.
Neurologic factors: GCS, presence of pneumonia, types of stroke.
Preexisting stroke risk factors: history of hypertension, diabetic mellitus, cardiovascular diseases, alcohol drinking, cigarette smoking.
Data quality control and management
Data quality was assured by designing proper data abstraction tools. A pre-test was done for 5% of the sample size to pave the way for any modifications necessary. Two days of training were given to data collectors on the contents of the data abstraction checklist. During the data collection period, close supervision and monitoring were carried out on a daily basis. Finally, completeness and consistency were checked for all the collected data during data cleaning.
Operational definition
Event/death: is defined as recorded stroke death within the follow-up time occurring among first-ever adult stroke patients aged 18 years and above, and ascertainment of death was from death records on the patient’s medical record.
An incomplete patient chart refers to charts that have no date of admission and missed variables reviewed in the literature.
Censored: Those subjects who were discharged against medical advice, discharged with a significant neurological deficit or death other than stroke (accident or any cause not related to stroke), referred to other health facilities, or event-free until the end of the study, whichever occurred first, were considered censored.
Survival time: The survival time calculated in completed days using the time between dates of admission and the date of the event (1) (death) or date of censored (0).
Data processing and analysis
The completeness of the data was checked manually and coded accordingly. Errors were corrected and identified at the time after a review of the original data using the code numbers. After this, the data were entered using Epi-Data version 4.3 and exported to be analyzed using SPSS 20 statistical software. Continuous data, depending on the distribution, was described as mean, standard deviation, and median. Frequency and percent distribution were used for categorical data. Finally, the outcome of each participant was dichotomized into censored (0) or death (1). Kaplan-Meir was used to estimate the survival differences between categorical variables, and log-rank tests were used to compare survival time curves after admission. The Cox-proportional hazard regression model assumption was checked using the Schoenfeld residual test, which was fit. 26 A bi-variable Cox-proportional hazards regression model was fitted for each explanatory variable. Accordingly, those variables having a p-value ⩽ 0.20 in the bi-variable analysis were included in the multivariate Cox-proportional hazards regression model. An adjusted hazard ratio with a 95% confidence interval and a p-value < 0.05 was used to measure the strength of the association and identify statistically significant results.
Result
Socio-demographic characteristics of adult stroke patients
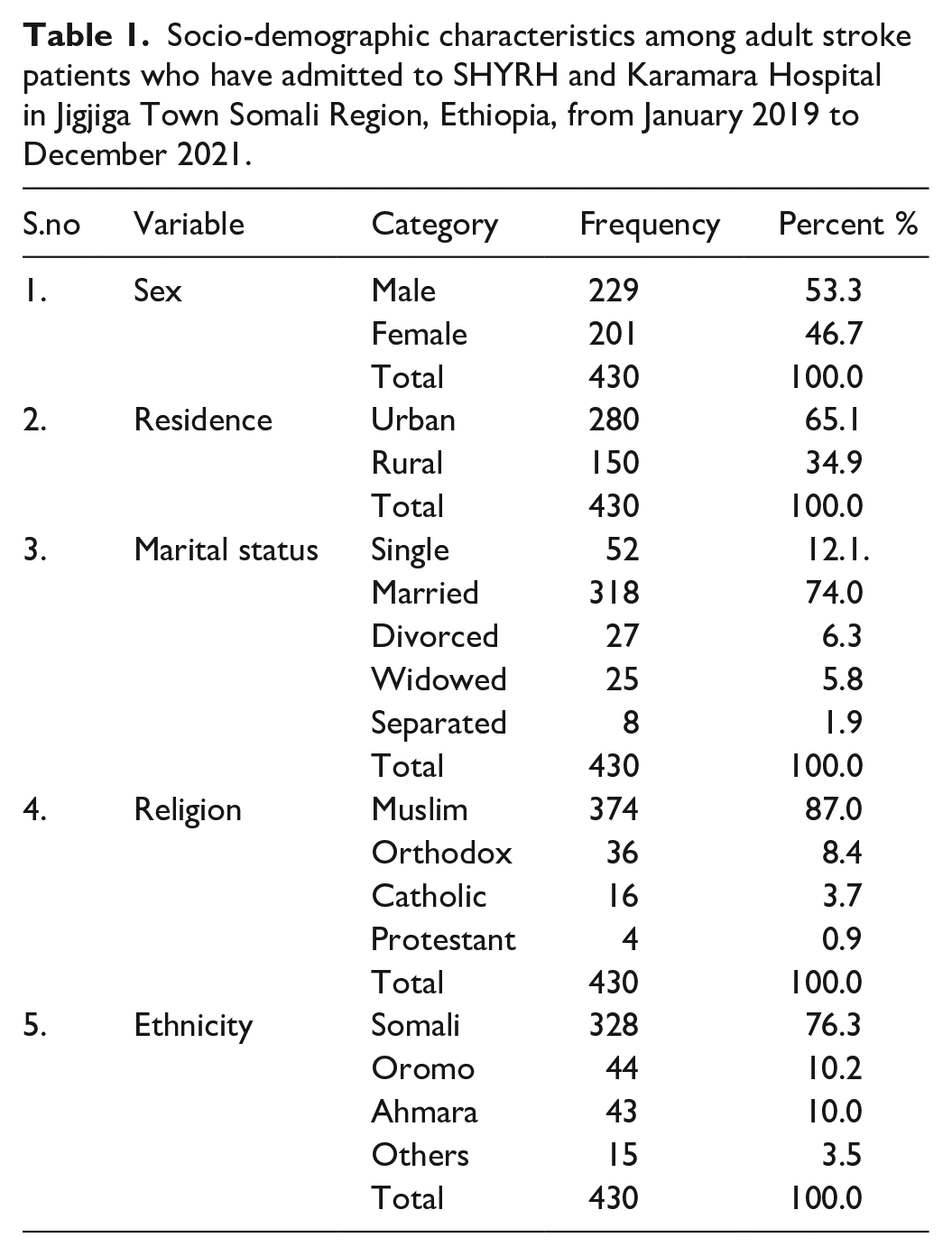
This study included 430 adult stroke patients; the mean age was 50.7 (SD ± 16.7) years. The patients’ maximum and minimum age were 95 and 20 years, respectively. More than half of the stroke patients (53.3%) were men. According to their distribution of religions, (87%) were Muslims, 36 (8.4%) were Orthodox, 16 (3.7%) were Catholic, and 4 (0.9%) were protestants. According to where they lived, the majority of participants (65.1%) were urban (Table 1).
Socio-demographic characteristics among adult stroke patients who have admitted to SHYRH and Karamara Hospital in Jigjiga Town Somali Region, Ethiopia, from January 2019 to December 2021.
Incidence of adult stroke patients
All 430 study subjects had contributed 22.3% (95% CI: 18.6–26.7) deaths, and the overall incident rate of stroke adult mortality during the follow-up time was 7.15 per 1000 person-days, a total of 13,416 person-days, and the overall mean and median survival time of stroke during follow-up were 90.8 and 120 days, respectively.
Patients’ baseline data (vital signs) of adult stroke patients
The patients’ maximum systolic blood pressure was 230, their minimum was 80, their ranges were 150, and their mean was 134.83 (SD ± 25.99). The maximum pulse rate of patients was 162, with a minimum of 32, a range of 130, and a mean of 94.22 (SD ± 17.59). The patient’s maximal respiratory rate was 43, their lowest was 13, their range was 30, and their mean was 22.73 (SD ± 3.710). The patient’s mean body temperature (°C) was 36.99 with a SD of ±0.915, and the maximum body temperature (°C) was 40.2, the minimum was 31.3, and the range was 8.9 (Table 2).
Patients’ baseline data (vital signs) among adult stroke patients admitted to SHYRH and Karamara Hospital in Jigjiga Town Somali Region, Ethiopia, from January 2019 to December 2021.

Diagnosis and neurological assessment and preexisting risk factors of adult stroke patients
Among the total number of stroke-affected adult patients, 41.6% developed pneumonia, 60.2% had ischemic strokes, and 39.8% had hemorrhagic strokes. 219 patients (51% of the total) experienced disability. The majority of adult stroke patients, 186 (43.3%), had a Glasgow coma scale score between 9 and 12. Moreover, out of 430 stroke patients, 218 (50.7%) had previously experienced hypertension, 26.7% had previously experienced diabetes, and 24.9% had previously experienced cardiovascular disease (Table 3).
Diagnosis and neurological assessment and preexisting risk factors of adult stroke patient admitted to SHYRH and Karamara Hospital in Jigjiga Town Somali Region, Ethiopia, from January 2019 to December 2021.

Survival status of adult stroke patients
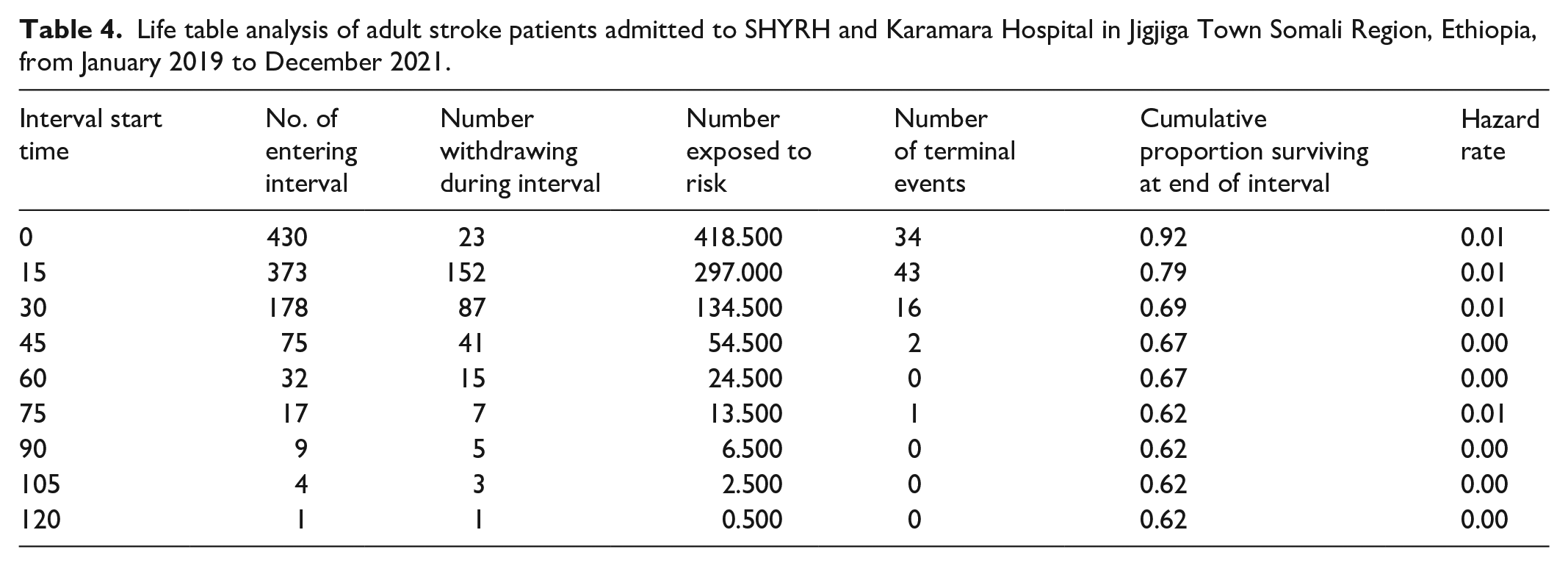
In total, 430 study subjects contributed; the total extent of follow-up was 13,416 person-days; and the overall mean and median survival time were 90.8 and 120 days, respectively. The overall incident rate of stroke adult mortality during the follow-up period was 7.15 deaths per 1000 person-days. Based on the life table analysis, the follow-up time with the cumulative proportion of survivors was 62% in SHYRH and KH stroke adults during the follow-up time. The cumulative probability of adult stroke survivors surviving in the first 15, 30, 60, and 120 days was 79%, 69%, 67%, and 62%, respectively (Table 4).
Life table analysis of adult stroke patients admitted to SHYRH and Karamara Hospital in Jigjiga Town Somali Region, Ethiopia, from January 2019 to December 2021.
Survival function and comparison of different categorical variables
The estimate of survivor function among several groups of variables for comparison is provided by the Kaplan-Meier survival curve. According to this study, adult stroke patients with GCS levels between 3 and 8 had a shorter mean survival time—57.75 days (95% CI: 48.82–66.68)—than patients with GCS levels of 9–12, who had a mean survival time of 103.19 days (95% CI: 93.38–112.99), and patients with GCS levels 13–15, who had a mean survival time of 92.04 days (95% CI: 81.72–102.36) (Figure 1).

The Kaplan-Meier survival curves compare the survival time of adult stroke patients with categories of GCS level in SHYRH and KH, Jigjiga, Ethiopia.
In this study, an adult stroke patient who had developed pneumonia had a lower mean survival time of 58.75 days (95% CI: 50.85–66.65) as compared to those who had not developed pneumonia, with a mean survival time of 111.85 days (95% CI: 104.96–118.74) (Figure 2).

The Kaplan-Meier survival curves compare the survival time of adult stroke patients with developed pneumonia and those not developed admitted in SHYRH and KH, Jigjiga, Ethiopia.
In this study, an adult stroke patient who had a previous history of hypertension had a lower survival time with a mean survival time of 66.71 days (95% CI: 57.05–76.34) as compared to those who had no previous history of hypertension with a mean survival time of 110.74 days (95% CI: 103.48–117.99) (Figure 3).
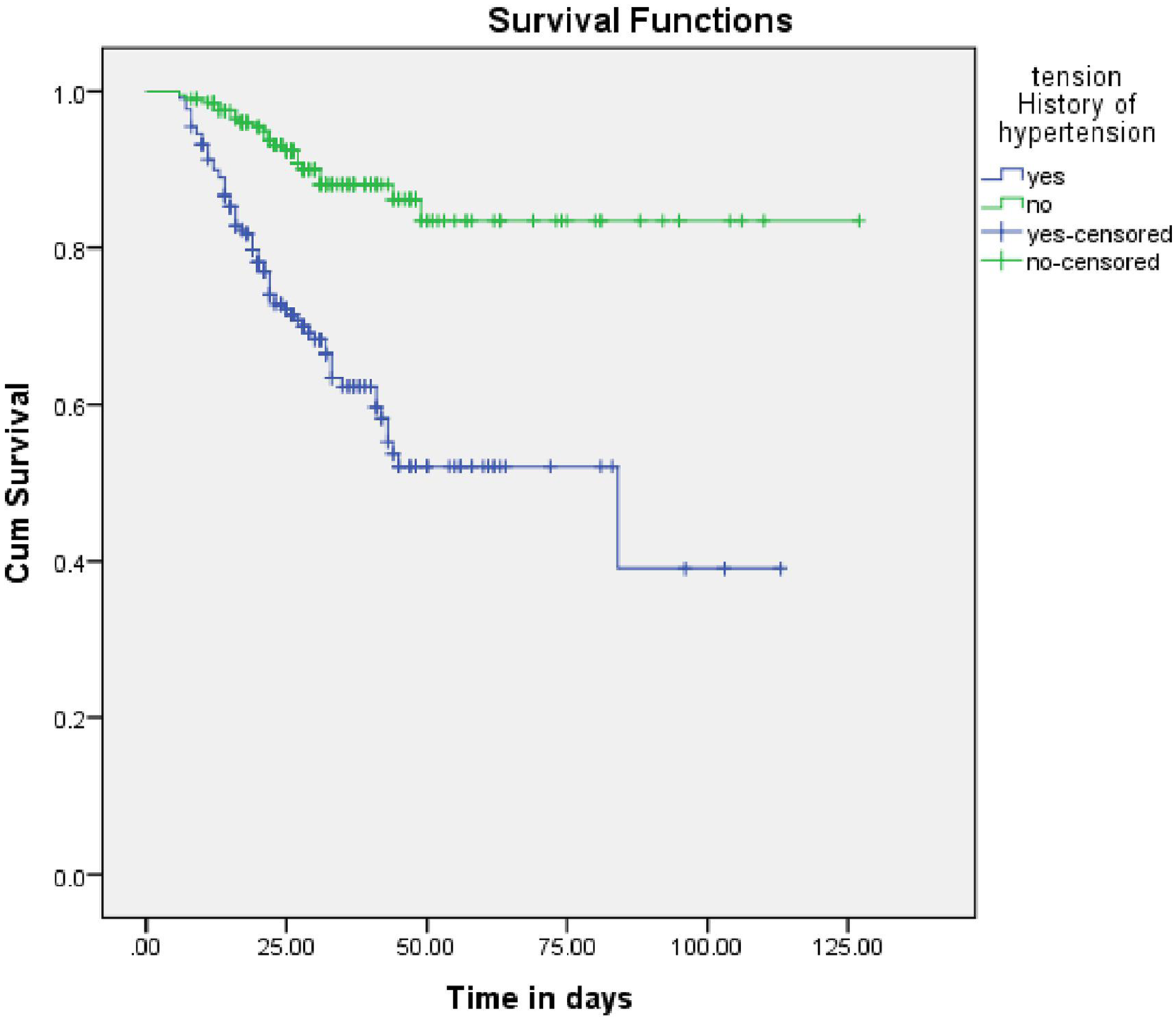
The Kaplan-Meier survival curves compare the survival time of adult stroke patients who had a previous history of hypertension and those who did not have previous history of hypertension admitted in SHYRH and KH, Jigjiga, Ethiopia.
Bivariate and multivariate Cox regression analysis of adult stroke patient mortality and predictors
The relationship between the outcome variable and the risk of mortality was analyzed using the Cox-proportional hazard regression model. In the bi-variable Cox regression model, sex, age ⩾ 71, presence of pneumonia, GCS level, type of stroke, pulse rate, body temperature, previous history of cardiovascular diseases, previous history of hypertension, and previous history of DM became candidates for the multi-variable Cox regression model at a p-value < 0.20. Moreover, to identify independent predictors of mortality and survival, multivariate Cox regression was performed for all predictors from the bi-variable analysis. However, only GCS level, presence of pneumonia, age ⩾ 71, and previous history of hypertension were statistically significant (p-value < 0.05) predictors of mortality in the multivariate analysis.
The result of multivariate analysis showed that stroke patients with Glasgow coma scale levels between 3 and 8 were 6.9 (AHR: 6.9; 95%CI: 2.8–17.1) times more likely to die as compared to those with GCS 3–8, and similarly, stroke patients with Glasgow coma scale levels between 13 and 15 were 2.8 (AHR: 2.8; 95%CI: 1.1–7.4) times more likely to die as compared to those with GCS 3–8.
Regarding pneumonia, patients with pneumonia were 2.7 (AHR: 2.7; 95% CI: 1.5–4.6) times more likely to die as compared to those without pneumonia.
Patients aged ⩾ 71 years were 1.9 (AHR: 1.9; 95% CI: 1.02–3.4) times more likely to die as compared to stroke patients aged ⩽ 49.
Patients with a history of hypertension were 2.07 (AHR: 2.07; 95% CI: 1.08–3.9) times more likely to die as compared to those adult stroke patients with no previous history of hypertension (Table 5).
Results of bivariate and multivariate Cox regression analysis among adult stroke patients admitted to SHYRH and Karamara Hospital in Jigjiga town Somali Region, Ethiopia, from January 2019 to December 2021.

Discussion
This study showed that the overall mortality of adult stroke patients admitted to SHYRH and KH during the study period was 96 (22.3%) (95% CI: 18.6–26.7). This finding is higher than a study conducted in Albania 16.6%, 27 Ethiopia at Shashemene Referral Hospital (13.3%), 22 Felege Hiwot Referral Hospital Bahir Dar 11%, 21 North West Ethiopia 56 (15.2%). 1 This study is consistent with TASH (19.2%), 23 Middle east in Azerbaijan province (22%), 28 Zimbabwe (25%), 29 and lower than the study conducted in a Nigerian teaching hospital (35%), 30 in Uganda (26.8%). 31 This difference could be due to different ways of stroke diagnosis, types of strokes, treatment approaches, comorbidity, complications, and in-hospital patient care. Also, the arrival time of the patients at the hospital after the onset of a stroke may be different. This difference could be that this study was conducted at the two major health facilities in the city, which covered the largest portion of the city as well as regional referral patients.
According to this study, the incidence of stroke is 7.15 deaths per 1000 person-day observation (95% CI: 5.27–9.03). This finding is lower than the study conducted at Saint Paul’s hospital in Ethiopia, where the incidence of 251 stroke participants was 9.5 deaths per 1000 people per day, 32 in Zimbabwe, stroke mortality reported was 107/100,000, 29 in Africa, by using Systematic Review and Meta-Analysis, 535,000, or 89.9 (87.0–625.3) per 100,000 person-years of new stroke cases 33 and in India, the incidence of stroke was 15.2 deaths per 1000 persons per year. 34 This difference might be because study participants differ in many socio-demographic and environmental aspects and types of study design. Another reason might be stroke incidence in Africa, based on a systematic review using ten different types of research.
Stroke patients with Glasgow coma scale levels between 3 and 8 were 6.9 (AHR: 6.9; 95% CI: 2.8–17.1) times more likely to die as compared to those with Glasgow coma scale levels between 3 and 8, and similarly, those with Glasgow coma scale levels between 13 and 15 were 2.8 (AHR: 2.8; 95% CI: 1.1–7.4) times more likely to die as compared to those with Glasgow coma scale levels between 3 and 8. The current findings agree with a study in Uganda that found people were three times more likely to die, 31 in Nigeria, 30 and in Saint Paul’s hospital, Ethiopia, four times more likely to die. 32 The reason for the similarity might be that patients with a decreased GCS level have decreased brain stimulation and other activities of the body, which result in airway obstruction, aspiration, and being unable to control hunger. This variable has clinical significance during patient management as it affects the length of stay, the functional outcome of the patient, and the overall cost of stroke treatment. And the reason for the difference might be due to variations in early hospital admission.
Regarding pneumonia, patients with pneumonia were 2.7 (AHR: 2.7; 95% CI: 1.5–4.6) times more likely to die as compared to those without pneumonia. This study agrees with a study conducted in Zimbabwe, 29 Nigeria, 30 and Saint Paul’s hospital, Addis Ababa Ethiopia. 2 Pneumonia is a predictor of mortality in stroke patients, which might be related to decreased GCS that leads to abnormal lip closure, lingual in coordination, delay, or absence of swallowing trigger reflex. Additionally, most stroke patients can’t feed themselves, which means they develop aspiration if they feed without a nasogastric tube or during the insertion of a nasogastric tube, which is a risk for aspiration pneumonia. But there is a difference in the pneumonia mortality rate of stroke patients who develop pneumonia in the three studies above. In this study, 74 (41.34%) people who developed pneumonia were dead in Zimbabwe, 29 a total of 108 stroke patients were exposed to pneumonia; 44.0% of the patients died, and in Nigeria 30 and 65 (60.7%) were dead in Saint Paul’s hospital, Addis Ababa Ethiopia. 2 This percent difference might be due to the arrival time of a patient to a hospital; it may be after a severely complicated condition. Another reason might be the sample size of the studies.
In this study, the history of hypertension was associated with stroke mortality. This result supports other studies conducted in Chang Gungs, 35 Southwestern Saudi Arabia, 8 Ayder Comprehensive Specialized Hospital, Tigray, Ethiopia, 20 stroke units of Jimma university medical center, southwest Ethiopia, 36 The reason may be that hypertension increases intracranial pressure, which leads to a decreased level of consciousness, which lasts until death. The possible mechanisms by which hypertension can lead to stroke and increase the hazard of death are: Hypertension causes auto-regulatory dysfunction with excessive cerebral blood flow, which leads to a higher risk of re-perfusion injury and hemorrhagic transformation.
In the previous Study in the Netherlands 37 for hemorrhagic stroke patients, Singapore, 38 ischemic stroke patients, Azerbaijan 28 for all stroke-type patients, and Uganda. 31 For all stroke-type patients, older or advanced age is a relevant predictor of mortality. Similarly, in this study, advanced age has an association with stroke mortality. This similarity may be due to stroke patients with advanced age being late to arrive at the hospital after the onset of stroke, as well as decreased ability, which may be related to the level of consciousness in almost every setting.
Limitations of the study
Limitations of the study, secondary data and a checklist were used. This may introduce information bias during data collection because the study variables that were useful may be missed, as is commonly asserted in retrospective cohort study design.
Conclusion
According to the findings of this study, stroke mortality was high; 96 (22.3%) died, and the incidence of mortality was 7.15 per 1000 people per year. Decreased GCS, the presence of pneumonia, being older than 71, and having a history of high blood pressure were predictors of mortality in adult stroke patients. A multifaceted work should be done by focusing health education on preventive activities for hypertension, special care for stroke patients with low Glasgow coma scale, advanced age, pneumonia, and history of hypertension. In addition to that, a prospective cohort study is recommended to be done by including socio-demographic and behavioral factors that could not be found on the patients’ charts.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241258147 – Supplemental material for Incidence of mortality and risk factors among adult stroke patients in public hospitals Jigjiga town Somali region, Ethiopia: Cohort study design
Supplemental material, sj-docx-1-smo-10.1177_20503121241258147 for Incidence of mortality and risk factors among adult stroke patients in public hospitals Jigjiga town Somali region, Ethiopia: Cohort study design by Ahmed Mohammed Ibrahim, Abdirasak Abdulahi Abdi, Ramadan Budul Yusuf, Mohamed Omar Osman, Abdilahi Ibrahim Muse, Girma Tadesse Wadajo, Afework Hailu, Abdurahman Kedir Roble, Mohamed Ali Issack and Ali Ahmed Mahamed in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Jigjiga University and hospitals. Also, we express our gratitude to all the data collectors who participated in this study for their hard work and diligence.
Author contributions
All authors contributed to the study’s conceptualization, design, acquisition, data analysis, and result interpretation. During manuscript submission, authors examined the work critically and contributed to its development. The authors all agreed to take responsibility for the content of the work, having read and approved the final draft.
Data sharing statement
The responsible author will provide the datasets used for the analysis upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical consideration
Ethical approval for the research was obtained from the Jigjiga University Institution of Research and Ethics Review Board (JJURERB0051/2022). Permission was obtained from these hospitals to extract data from patient medical records, and the data from the medical records is handled with strong confidentiality.
Informed consent
Informed consent was not sought for the present study because the data included was retrospective and it was not necessary for obtaining informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.