
Abstract
Background:
Birth-related perineal trauma is a public health issue that can lead to significant maternal morbidity in low-income countries like Ethiopia. Research on the proportion and underlying factors of birth-related severe perineal tears is rare, both in the study area and throughout Ethiopia. As a result, this study was intended to determine the proportion of birth-related severe perineal tears and associated factors at hospitals in Bahir Dar town, Ethiopia.
Methods:
A cross-sectional study was undertaken at government hospitals in Bahir Dar, Ethiopia. Five hundred fifteen study subjects were selected using a systematic sampling technique. The data was collected through chart reviews and interviews. Data was entered and analyzed using SPSS Version 23. A binary logistic regression was employed to identify factors, and an adjusted odds ratio and a 95% CI were used to estimate the strength of relationships. Statistical significance was declared at p-value < 0.05.
Result:
The prevalence of severe perineal tears was 7.4%. Previous history of a perineal tear (AOR = 3.06, 95% CI = 1.24–7.59), being nullipara (AOR = 4.03, 95% CI = 1.42–11.44), occipito-posterior position (AOR = 5.49, 95% CI = 2.27–13.28), duration of second stage of labor > 2 h (AOR = 5.42, 95% CI = 2.26–12.99), birth attendant’s work experience <1 year (AOR = 5.98, 95% CI = 2.16–16.57) were found to be associated with birth-related severe perineal tear.
Conclusion:
The proportion of birth-related severe perineal tears was high at governmental hospitals in Bahir Dar town. Previous history of perineal tear, work experience of birth attendants, duration of the second stage of labor, being nullipara, and occipito-posterior position were the major determinants of severe perineal tear. This study suggests that strategies and regulations should be developed to shorten the second stage of labor.
Introduction
A severe perineal tear is a public health issue, especially in the context of maternal health, that can lead to significant maternal morbidity, including pain, infection, incontinence, sexual dysfunction, impaired emotional well-being, and poor quality of life. 1 A perineal tear is an injury to the perineal skin, vaginal mucosa, perineal muscle, or anal sphincter complex. The tear may extend to the labia, vagina, urethra, and clitoris. 2
A perineal tear is classified into four degrees: The first-degree perineal tear typically affects the perineal skin and mucosa; the second-degree perineal tear spreads to the perineal muscle; the third-degree perineal tear affects the anal sphincter; and the fourth-degree perineal tear affects both the internal and external anal sphincter and the anorectal mucosa. The perineal injuries are further classified into light (degrees I and II) and severe (degrees III and IV).3–5
Several direct and indirect factors raise the possibility of birth-related perineal injury. Some of these factors were instrumental delivery, longer duration of the second stage of labor, nulliparity, birth weight >4 kg, induced labor, shoulder dystocia, and occipito-posterior (OP) position.6–8
The magnitude of birth-related severe perineal tears is variable across different countries and ranges from 0.6% to 8%. 9 A large study done in 20 European countries showed that the rate of 3rd and fourth-degree perineal tears ranged from 0.1% to 4.9%. Specifically, it was 4.1% in Denmark, 4.9% in Iceland, and 3.2% in England. 10 Another study done in Australia found that the incidence of severe perineal tears was 3%. 11 The findings of a systematic review and meta-analysis study in low and middle-income countries showed that the overall rate of second-degree tears and obstetric anal sphincter injuries was 24% and 1.4%, respectively. 8
Worldwide, almost 295,000 women die each year due to different pregnancy- and delivery-related obstetric and medical complications. 12 The majority of these are happening in resource-limited countries, mainly in Sub-Saharan Africa, which covers more than 94% of the burden. 12 A birth-related perineal trauma is one of the causes of maternal mortality and morbidity in low- and middle-income countries. 13 Severe perineal trauma is also associated with significant maternal morbidity in European countries.10,14–16
Untreated severe perineal tears have acute and chronic complications. These complications are more prevalent in resource-limited countries, including Ethiopia, due to poor preventive practices and inadequate access to resources.8,17,18
Early complications of an untreated birth-related severe perineal tear include tear disruption, pain, hemorrhage, and puerperal sepsis.6,7 Acute complications hemorrhage and puerperal sepsis are the major causes of maternal death in low- and middle-income countries, including Ethiopia, 19 while chronic complications include urinary and fecal incontinence, persistent pain, dyspareunia, pelvic organ prolapse, and fistulas. These complications have serious consequences for women of reproductive age and can influence women’s general health, physical, psychological, and social well-being and sexual relations.5,6,8,10,20
Even though the burden of perineal tear has been extensively investigated in high- and some middle-income countries, there was a paucity of research in Ethiopia, especially in the research area. Thus, this study was aimed at determining the proportion and determinants of birth-related severe perineal tears at governmental hospitals in Bahir Dar town. The findings of this study can help to raise awareness about the prevalence and impact of severe perineal tears in resource-limited settings among healthcare providers, policymakers, and the general public. This can lead to improved recognition and management of these injuries, ultimately decreasing maternal birth-related complications and deaths. In addition, the findings of this research can inform the development of evidence-based guidelines and protocols for the avoidance, diagnosis, and treatment of severe perineal tears in resource-limited settings. These guidelines can help standardize care practices and ensure that women receive appropriate treatment when they experience these injuries.
Methods
We have followed the strengthening the reporting of observational studies in epidemiology checklist for observational studies to prepare this manuscript (Supplemental file 1).
Study design, area, and period
Cross-sectional study was carried out at governmental hospitals in Bahir Dar town, Amhara region, Ethiopia, from March 2023 to June 2023. Bahir Dar is the capital city of the Amhara region in northern Ethiopia. Bahir Dar town has three governmental hospitals (Tibebe Ghion Specialized Referral Hospital, Felege Hiwot Referral Hospital, and Addis Alem Primary Hospital).
Study population
The study populations were all mothers who gave birth vaginally at term at public hospitals in Bahir Dar town during the study period. All mothers who gave birth vaginally at term (gestational age of 37 – 41 + 6 weeks), regardless of their age, pregnancy status (single vs multiple), and infection status, were included in the study. Mothers with congenital genital tract, stillborn newborns, congenital anomalies of fetuses (like anencephaly), intrauterine growth restriction fetuses, and small for gestational age fetuses were excluded.
Definition and measurement of variables
Birth-related severe perineal tear: The presence of either a grade 3 or grade 4 perineal tear following delivery was considered a birth-related severe perineal tear.5,18 The tear was diagnosed using a bidigital vagnorectal examination by BSc midwives and obstetricians.
The dependent variable was birth-related severe perineal tear (yes or no), whereas maternal age, residence, occupation, educational status, parity, gestational age, antenatal care (ANC) follow-up, onset of labor, method of induction, precipitating labor, duration of second stage of labor, history of perineal tear, episiotomy, presentation, position, mode of delivery, sex of the newborn, weight of the newborn, head circumference, birth attendant’s profession, and birth attendant’s work experience were taken as independent variables.
Sample size determination
The required sample size was determined by using factors for a perineal tear from the previous study (fetal weight ⩾ 4 kg) 21 and calculated by using the open EpiInfo version 7 statistical software packages. The sample was calculated using the assumptions of a 95% confidence interval, 80% power, exposure to a non-exposed ratio of 1:1, 8.57% of the outcome in the non-exposed group, 8.57% in the exposed group, and a 10% non-response rate. Thus, the last sample size was 515.
Sampling method and procedure
Participants for the study were chosen from each institution using a systematic sampling procedure. First, study participants were assigned proportionally to each hospital, using the prior number of deliveries as a reference. As a result, 400 sample sizes were distributed to both Tibebe Gehion and Felege Hiwot Referral Hospitals (200 research participants for each). The remaining 115 sample sizes were given to Addis Alem Primary Hospital. Then, a systematic sampling procedure was employed to pick research participants from each institution. The sampling interval (Kth unit) was calculated by dividing the total number of women who delivered at each hospital during the study period by the total number of sample sizes at each hospital. During the study period, 1545 moms had their babies in three hospitals. As a result, the sampling interval was three, as calculated by dividing 1545 by the total number of samples (515). We used a lottery to choose the initial mother and then enrolled every third woman until we reached the desired sample size.
Data collection instruments and technique
Both medical chart reviews and interviewer-administered questionnaires were used for data collection. The data collection tool was validated in Ethiopia previously.5,22 Data was collected by six trained midwives with bachelor’s degrees. Questionnaires were prepared in English (Supplemental file 2).
Statistical analysis
The data were examined for correctness and inconsistency. The collected data were analyzed using SPSS Version 23. Descriptive and binary logistic regression analyses were performed. In binary logistic regression, both bivariable and multivariable logistic regression were employed. Multivariable logistic regression was applied to variables with p-values ⩽ 0.2 from bivariable analysis. In multivariable logistic regression, the level of statistical significance was set at p < 0.05. An adjusted odds ratio (AOR) with a 95% CI was used to assess the strength of the association between severe perineal tears and determinant variables. The stepwise logistic regression approach was chosen for multiple logistic regressions.
Ethical approval
The data collection was carried out after getting approval for the project proposal from the ethical review board (IRB) of Bahir Dar University College of Health Sciences. The ethical approval number for the study is BDU/IRB/1/254/15. An official letter was obtained from the Amhara Public Health Institute and permission from each hospital medical director and labor ward coordinator. Data were collected after informed written consent was obtained from study participants. In the case of teenagers (age < 18 years), informed written consent was obtained from parents or guardians. In addition, a legally authorized representative has signed the informed written consent for the minor study subjects and study subjects with no formal education (unable to read and write). The questionnaire was administered anonymously.
Result
Sociodemographic characteristics
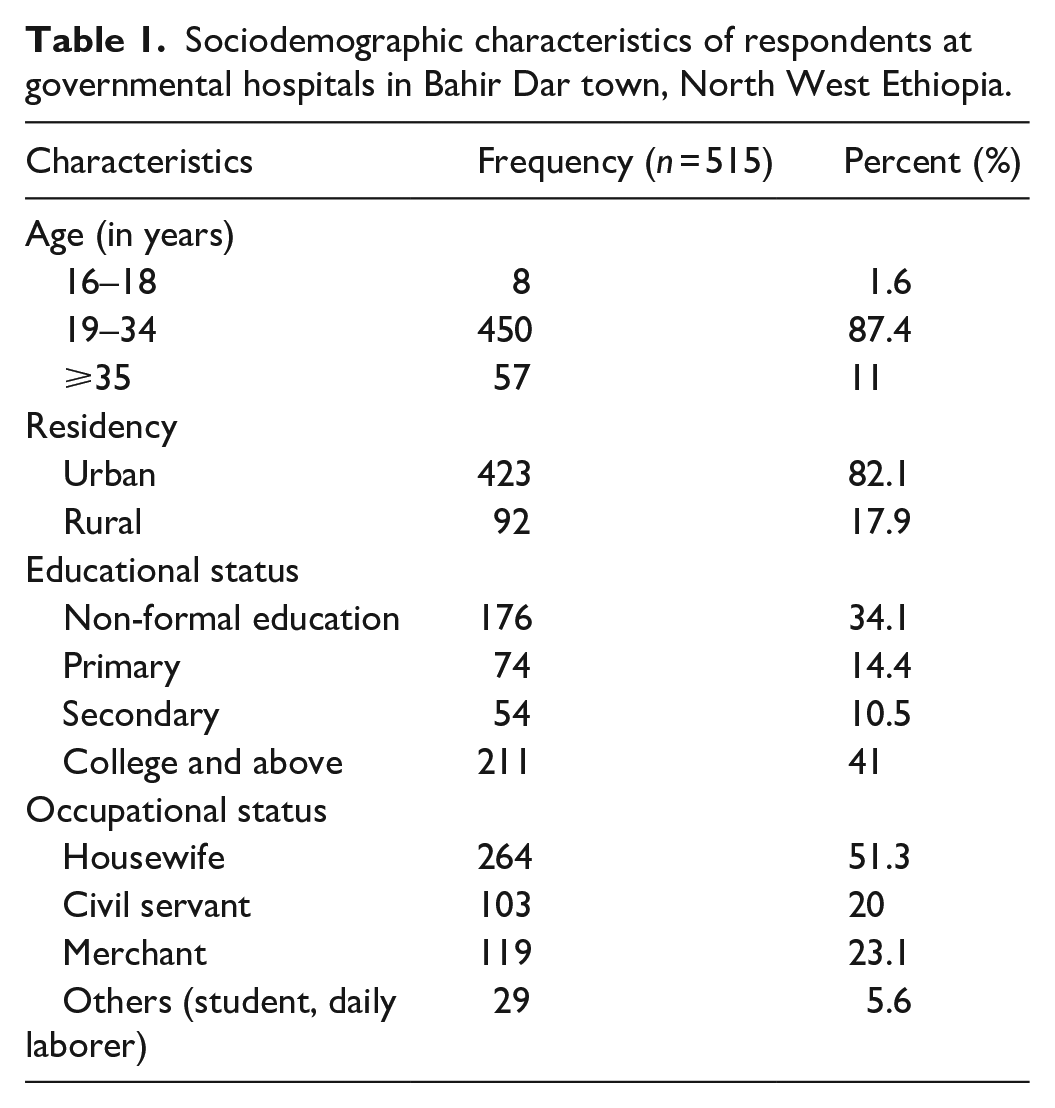
The majority of participants (95.5%) were Amhara in ethnicity, 423 (82%) of the participants were from urban areas, and nearly half (264 (51.3%)) of the participants mentioned housewives as their occupation (Table 1).
Sociodemographic characteristics of respondents at governmental hospitals in Bahir Dar town, North West Ethiopia.
Obstetric-related characteristics of participants
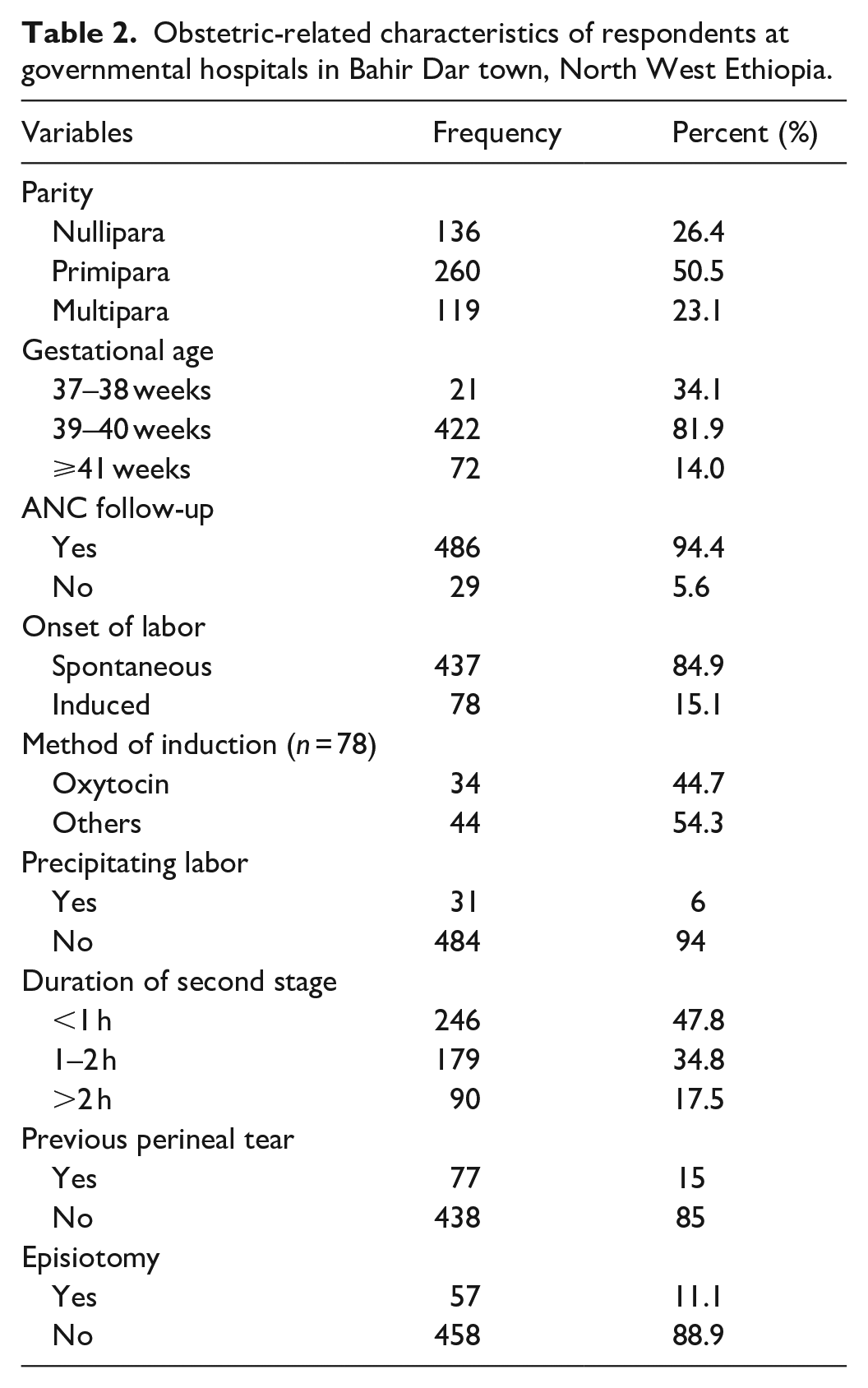
The majority (486, or 94.4%) of study participants had ANC follow-up, and half of the respondents (50.5%) were primipara mothers. The majority, 437 (84.9%) of participants, had spontaneous onset of labor, 422 (81.9%) of respondents had full-term pregnancy, and 77 (15%) of participants had a previous history of perineal trauma (Table 2).
Obstetric-related characteristics of respondents at governmental hospitals in Bahir Dar town, North West Ethiopia.
Delivery and fetal-related characteristics
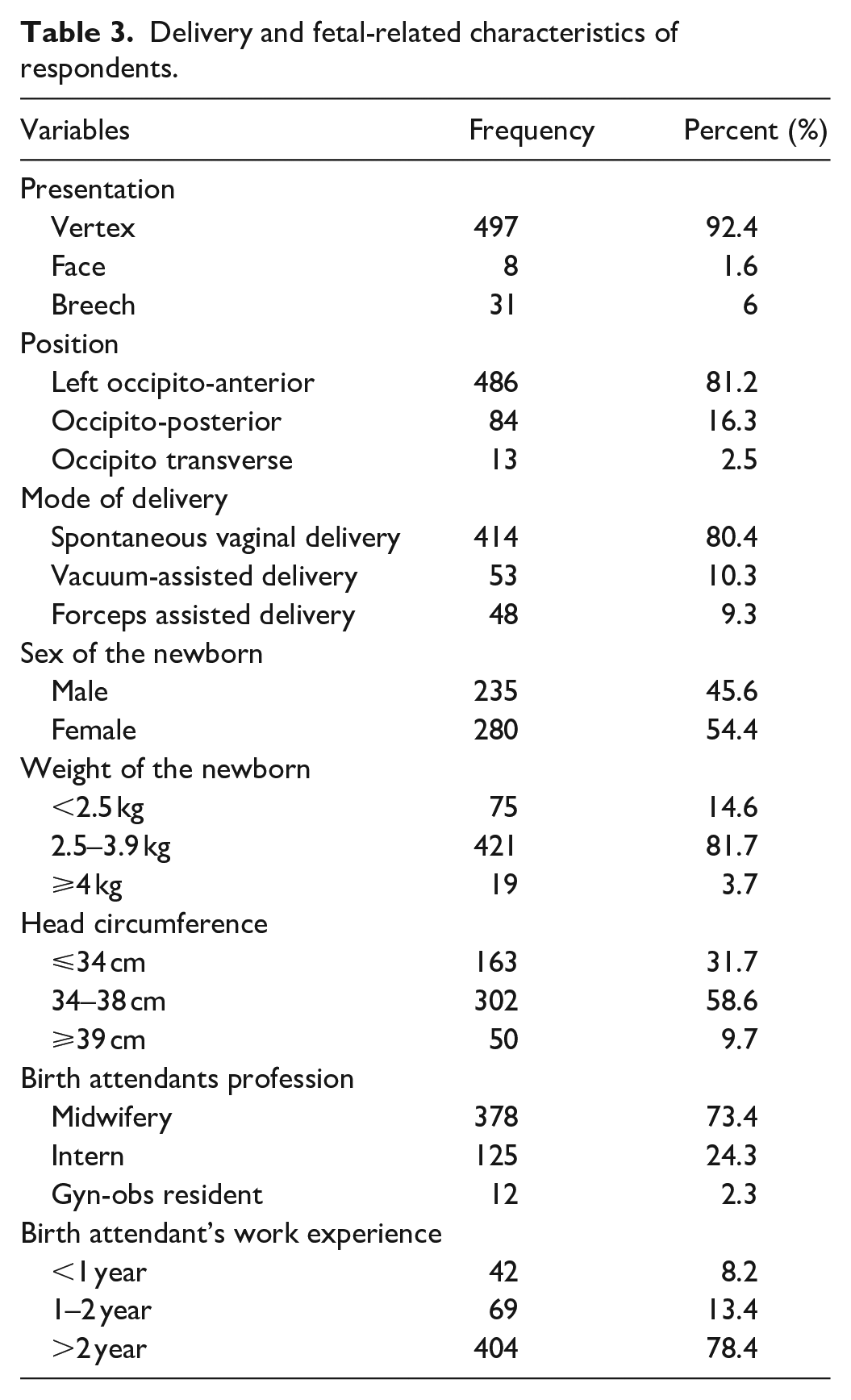
The majority, 497 (92.4%) of participants, had vertex presentation, 486 (81.2%) of participants had left occipito-anterior position, and 414 (80.4%) of the participants were delivered spontaneously through the vagina. Nearly half of the study participants (54.4%) delivered female newborns. More than three-fourths, 421 (81.7%) of the participants had normal-birth-weight newborns (2.5–3.9 kg). Nearly three-fourths (378, or 73.4%) of the respondents were attended by midwives during delivery (Table 3).
Delivery and fetal-related characteristics of respondents.
Proportion of birth-related severe perineal tear
The proportion of severe perineal tears at governmental hospitals in Bahir Dar town was 7.4% (95% CI = 5.2–9.7).
Determinant factors for birth-related severe perineal tear
A bivariable and multivariable logistic regression model was used to identify significant variables for a severe perineal tear. Mode of delivery, precipitating labor, previous perineal tear, fetal position, parity, duration of the second stage of labor, and work experience of the birth attendant had a p-value < 0.2 in the bivariable model. The multivariable logistic regression model adjusted the effects of mode of delivery and precipitating labor on perineal tear. After adjusting the above variables, the model has provided significant factors such as previous perineal tear, parity, duration of the second stage of labor, and work experience of a birth attendant.
The present finding showed that mothers who had a previous history of perineal tears were 3.06 times more likely to develop birth-related severe perineal tears as compared to their counterparts (AOR = 3.06, 95% CI = 1.24–7.59).
The likelihood of a birth-related severe perineal tear was 4.03 times higher in those nullipara mothers as compared to multipara mothers (AOR = 4.03; 95% CI = 1.41–1.44).
The occurrence of a birth-related severe perineal tear was 5.49 times higher in the OP position as compared to the occipito-anterior position (AOR = 5.49, 95% CI = 2.27–13.28).
The likelihood of a birth-related severe perineal tear was 5.42 times higher in those laboring mothers who had a duration of the 2nd stage of labor >2 h as compared to those mothers who had <1 h (AOR = 5.42, 95% CI = 2.26–12.99).
Mothers who were delivered by a birth attendant with work experience less than 1 year were 5.98 times more likely to develop a birth-related severe perineal tear as compared to those delivered by a birth attendant with work experience >2 years (AOR = 5.98, 95% CI = 2.16–16.57) (Table 4).
Factors that entered the bivariable and multivariable logistic regression models.
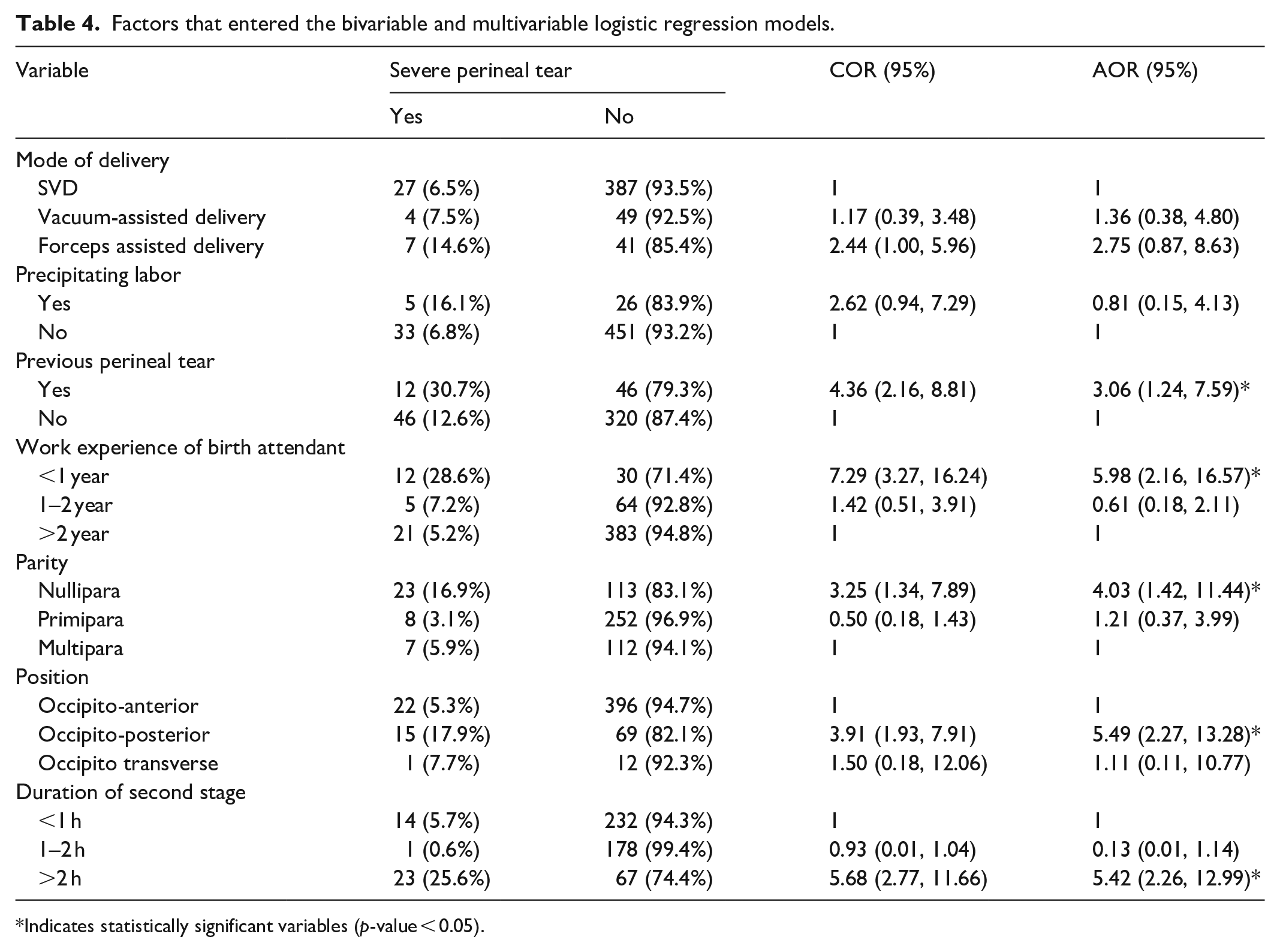
Indicates statistically significant variables (p-value < 0.05).
Discussion
This study found that the prevalence of birth-related severe perineal tears was 7.4% (95% CI = 5.2–9.7). This finding was higher than a study found in Brazil (1.51%), 18 Center Sestre in Croatia (0.34%), 20 and Mexico (2%). 23 This may be due to differences in the quality of labor and delivery care, the increased prevalence of predisposing factors, and the difference in the management of obstetric cases like OP positions and prolonged second stage of labor. Besides this, variation could be due to discrepancies in training and level of experience of birth attendants.
The present finding was also higher than a study finding at Benue State University Teaching Hospital in Nigeria (0.2%). 21 The discrepancies between the studies might be due to the following reasons: This study used a relatively large sample size as compared to other previous studies. The increased prevalence in our setup may be due to this increased sample size. Moreover, perineal re-examination practice following delivery is increasing in our country; as a result, the rate of birth-related perineal tear can be increase when women are re-examined by trained health care providers.
However, the present finding was lower than a study finding at King Abdulaziz University Hospital in Saudi Arabia (29.6%). 24 The variation could be due to the difference in the study period. Furthermore, differences in the frequencies of birth-related severe perineal tears across studies could be attributed to the challenges in harmonizing the perineum examination after childbirth. Furthermore, although the prior country may have relied on imaging tools to diagnose birth-related severe perineal injuries, we did not.
According to this study, a previous history of perineal tears was significantly associated with birth-related severe perineal tears. Mothers who had a previous history of perineal tears were 3.06 times more likely to develop birth-related severe perineal tears as compared to their counterparts. This finding was supported by a study in Scotland. 25 This could be due to the following reasons: When a woman has experienced perineal tears in a previous delivery, scar tissue may form in the perineal area. This scar tissue can be less elastic and more prone to tearing during subsequent deliveries, increasing the risk of severe perineal tears. Furthermore, perineal tears can impair the endurance and health of the pelvic floor muscles, which play an important role in sustaining the pelvic organs and ensuring continence. Dysfunction in these muscles might make it harder to control the baby’s descent during delivery, increasing the risk of serious tearing.
Being a nullipara mother was significantly associated with a birth-related severe perineal tear. This finding was in agreement with a study finding in Brazil 18 and King Abdulaziz University Hospital, Kingdom of Saudi Arabia. 24 This could be due to several reasons: (1) Nulliparous women have not gone through the process of childbirth before, so their perineal tissues may be less elastic and more prone to tearing during delivery. The lack of previous stretching and trauma to the perineal area can make it more susceptible to severe tears. (2) The perineal tissues of nulliparous women may not be adequately prepared for the stretching and pressure that occurs during childbirth. Without previous experience with vaginal delivery, these tissues may be less able to accommodate the passage of the baby’s head, increasing the risk of severe tears.
OP position was significantly associated with birth-related severe perineal tear. This position can indeed increase the risk of birth-related severe perineal tears for several reasons: (1) Increased pressure on the perineum: In the OP position, the baby’s head is pressing against the mother’s perineum (the area between the vagina and anus) during labor. The prolonged pressure and stretching of the perineal tissues can increase the likelihood of severe tears occurring. (2) Difficulties in descent and rotation: Babies in the OP position may have difficulty descending through the birth canal and rotating into the optimal position for delivery. This can result in prolonged labor, increased pushing efforts, and greater strain on the perineal area, all of which can contribute to severe tears. (3) Extension of the head: Babies in the OP position may have a tendency to extend their heads during delivery, leading to a larger circumference passing through the vaginal opening. This extension can put additional pressure on the perineal tissues and increase the risk of severe tears.
Furthermore, an association was observed between prolonged 2nd stage of labor and birth-related severe perineal tear. This finding was in agreement with a study finding in Brazil 18 and King Abdulaziz University Hospital in Saudi Arabia. 24 Prolonged duration of the second stage of labor can increase the risk of birth-related severe perineal tears for several reasons: (1) Increased pressure and stretching: During the second stage of labor, the baby’s head is descending through the birth canal and putting pressure on the perineal tissues. If this stage is prolonged, the prolonged pressure and stretching of the perineum can increase the likelihood of severe tears occurring. (2) Tissue fatigue: The longer the second stage of labor lasts, the more fatigued and stretched the perineal tissues become. Fatigued tissues are more prone to tearing, especially when under prolonged pressure from the baby’s head. (3) Increased force and strain: Prolonged pushing efforts during the second stage of labor can lead to increased force and strain on the perineal area. This increased force can contribute to the likelihood of severe tears, especially if the pushing efforts are intense and prolonged. (4) Medical interventions: In cases where the second stage of labor is prolonged, healthcare providers may intervene with techniques such as forceps or vacuum extraction to assist with delivery. These interventions can increase the risk of perineal tears, especially if the baby’s position is not ideal or if there is a need for expedited delivery.
Finally, the work experience of birth attendants was significantly associated with birth-related severe perineal tears. Mothers who were delivered by a birth attendant with work experience less than 1 year were 5.98 times more likely to develop a birth-related severe perineal tear as compared to those mothers who were delivered by a birth attendant with work experience >2 years. Experienced or less skilled birth attendants may inadvertently contribute to an increased risk of severe perineal tears due to various factors: (1) Lack of skill and expertise: Inexperienced birth attendants may not have the same level of skill and expertise as more experienced practitioners. This can lead to improper techniques during delivery, such as excessive pulling or stretching of the perineum, which can increase the risk of severe tears. (2) Inadequate monitoring and support: Less experienced birth attendants may not be as adept at monitoring labor progress or providing appropriate support and guidance during the second stage of labor. Inadequate monitoring can result in missed opportunities to intervene early and prevent complications that could lead to severe tears. (3) Lack of confidence and decision-making skills: Less experienced birth attendants may lack the confidence and decision-making skills needed to manage challenging situations during childbirth, such as prolonged second-stage labor or difficult deliveries. This can result in delays in appropriate interventions or a higher likelihood of complications leading to severe tears.
Limitations of the study
The current study has some weaknesses. Some characteristics, such as past experiences of genital tears, were reported by themselves, so this study may be susceptible to recall bias. Lack of imaging to confirm the presence or absence of severe perineal trauma (sphincter injury) is also another limitation of this study. Moreover, measuring precipitated labor by asking those mothers who come to the health institution after labor is initiated at home might not be accurate.
Conclusion
The prevalence of birth-related severe perineal tears was high at governmental hospitals in Bahir Dar town. Previous history of perineal tear, work experience of birth attendants, duration of the 2nd stage of labor, being a nullipara mother, and OP position were the major determinant factors for birth-related severe perineal tear. This study suggests the need for developing strategies and guidelines to shorten the second stage of labor. In addition to this, adequate training and supportive supervision should be given to those birth attendants whose work experience is less than 1 year. Furthermore, non-modified risk factors (OP position and nullipara) should be recognized early, and appropriate prevention strategies should be employed.
Supplemental Material
sj-doc-1-smo-10.1177_20503121241252956 – Supplemental material for Risk factors associated with severe perineal tear at Public Hospitals in Bahir Dar town, Northwest Ethiopia
Supplemental material, sj-doc-1-smo-10.1177_20503121241252956 for Risk factors associated with severe perineal tear at Public Hospitals in Bahir Dar town, Northwest Ethiopia by Dagne Addisu and Betelihem Fentahun in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241252956 – Supplemental material for Risk factors associated with severe perineal tear at Public Hospitals in Bahir Dar town, Northwest Ethiopia
Supplemental material, sj-docx-2-smo-10.1177_20503121241252956 for Risk factors associated with severe perineal tear at Public Hospitals in Bahir Dar town, Northwest Ethiopia by Dagne Addisu and Betelihem Fentahun in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express gratitude to the Bahir Dar University College of Health Sciences. Our gratitude also extends to the study subjects and data collectors.
Authors’ contribution
DA wrote the main manuscript text, and BF prepared tables. All authors reviewed the manuscript.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the manuscript and its supplementary materials. Furthermore, the corresponding author will be contacted if someone wants to access the data for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
Not applicable in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.