
Abstract
Objective:
We explored the differences in deep venous catheterization-associated complications between patients with hematological malignancies after peripherally inserted central catheter placement and such patients after implantable venous access port catheterization.
Introduction:
peripherally inserted central catheters and implantable venous access ports are the most popular devices used for chemotherapy. However, no study has revealed differences between peripherally inserted central catheters and implantable venous access ports in Chinese patients with hematological malignancies.
Methods:
The clinical data of 322 patients with hematological malignancies who were treated from January 1, 2020 to December 30, 2021 were included in a retrospective cohort study. Postoperative color Doppler ultrasonography and follow-up results were used to compare the incidence rates of deep venous catheterization -associated complications after peripherally inserted central catheters and implantable venous access ports catheterization.
Results:
The relative risk of catheter-related complications considering the type of device was 8.3 (95% CI = 3.0–22.8). In addition, chi-square segmentation analysis revealed a significant difference in the complication rate between the internal jugular vein and the basilic vein (χ2 = 22.002, p < 0.0001) and between the subclavian vein and the basilic vein (χ2 = 28.940, p < 0.0001).
Conclusion:
Implantable venous access ports are safer than peripherally inserted central catheters for Chinese patients with hematological malignancies. The implantation of implantable venous access ports could be firstly considered for systematic anti-cancer treatment.
Introduction
Peripherally inserted central catheters (PICCs) and implantable venous access ports (PORTs) are the most common venous access options for chemotherapy. A PICC is a catheter that is inserted into a peripheral vein of the arm (basilic vein, median cubital vein, or cephalic vein); the tip of this catheter is then inserted into the superior vena cava along the direction of the blood vessel. While a PORT is a catheter that is commonly inserted into the internal jugular vein or the subclavian vein; the tip of this catheter is then also inserted into the lower 1/3 of the superior vena cava. 1 Both PICCs and PORTs provide convenient venous access for clinical chemotherapy; however, they still cause certain deep vein catheterization (DVC)-associated complications. 2
DVC-associated complications mainly include thrombosis, catheter blockage, detachment, and infection. Thrombosis in intravenous catheters is caused by endothelial trauma and inflammation, especially in patients who are hypercoagulable. The majority of thrombotic events that occur in the superficial and deep veins of the upper extremity can be attributed to intravenous catheters.3,4 Catheter bloodstream infection is defined as bacteremia caused by pathogen release from an intravenous catheter. 5 However, the difference in DVC-associated complications between PICCs and PORTs in patients with hematological malignancies is still unclear. Therefore, in this study, the clinical data of 322 patients with hematological malignancies from January 1, 2020 to December 30, 2021 were analyzed at Huashan Hospital Affiliated to Fudan University. Postoperative maintenance and follow-up of patients with central venous catheters were performed to compare the incidence rates of DVC-associated complications after PICCs and PORTs catheterization.
The purpose of this study was to compare differences in DVC-associated complications between PICCs and PORTs. Additionally, we explored the relationship between the puncture approach and DVC-associated complications.
Materials and methods
General data
The inclusion criteria were as follows: patients with hematological malignancies who received chemotherapy in the Department of Hematology; patients with no history of vital organ diseases or mental illness; and patients who volunteered to participate in the study. The exclusion criteria were as follows: patients with advanced hematological malignancies, unconscious patients who were unable to cooperate with local anesthesia surgery, patients with platelet counts <50 × 109/L, and patients with hemoglobin (Hb) <70 g/L.
The data of 350 patients with hematological malignancies who were admitted to the Department of Hematology in Huashan Hospital from January 1, 2020 to December 30, 2021 were recruited. Using the above inclusion and exclusion criteria, 322 patients were included in the analyses (Figure 1). The study protocol was reviewed and approved by the Ethics Committee of Huashan Hospital Affiliated with Fudan University. Written informed consent was obtained from all subjects before the study.

Flowchart of the study procedure.
Ethical approval
The present study was approved by the Ethical Review Board of Huashan Hospital Affiliated with Fudan University in Shanghai (No. 2022-1097). Written informed consent was obtained from all subjects before the study.
Methods
Clinical characteristics such as age, sex, hypertension status, diabetes mellitus status, smoking history, and type of hematological malignancy were collected
Age (measurement data) is expressed herein as –X ± s. Sex, hypertension status, diabetes mellitus status, smoking history and type of hematological malignancy (count data) are expressed as frequencies and percentages. Due to the incomplete health insurance system in China, on the basis of each patient’s condition and economic situation, he or she was allowed to freely receive PICCs or PORTs as the intravenous infusion access for chemotherapy for hematological malignancies.
Postoperative follow-up
The retrospective cohort study design flow is summarized in Figure 1. The research study involves 350 patients entered. In the PICCs group, 9 patients were excluded, while two patients lost follow-up visits. In the PORTs group, 14 patients were eliminated, and three failed to follow-up testing. The frequency of follow-up after PICC placement and PORTs catheterization was once a month, while the status of the device was monitored once a week. Professional nurses flushed the catheter with heparin sodium saline. If the catheter was not patent, ultrasound was performed immediately to determine whether there were complications such as thrombosis or catheter blockage. If there was redness of the skin at the surgical site, complete blood counts and blood culture tests were performed immediately to determine whether there was a catheter-related infection. We aimed to collect more accurate data to avoid selection and information bias.
Central venous devices
PICC placement was performed by the same qualified nursing team in our hospital, and PORTs catheterization was conducted by surgeons in the vascular surgery department. All devices were implanted under ultrasonography-guided catheter placement. The basilic or brachial vein was selected for PICC placement, while the internal jugular or subclavian vein was selected for PORTs. We chose the proper catheter diameter for patients. In addition, we adopted the aseptic nontouch technique, transmission-based precautions and vascular visualization to reduce complications. The PICC device used was a Bard PowerPICC SOLO Catheter 4 Fr (Bard Access Systems, Tamaulipas, Mexico). single lumen, and the PORTs device used was a PEROUSE MEDICAL polysite3017ISP 6 Fr. single lumen (SYMATESE GROUP, Lyon, France). The devices were checked carefully and washed following implantation. We confirmed the position of the device through chest X-ray immediately after implantation.
Statistical analysis
SPSS 29.0 (The IBM SPSS Campus Edition, Shanghai, China ) and R software (R 4.3.1,R Foundation for Statistical Computing, Vienna, Austria) 6 was used for the statistical analysis. The sample size calculation to compare two proportions was performed through the online Power Analysis and Sample Size (PASS) calculator (http://powerandsamplesize.com/) according to Sample Size Calculations in Clinical Research, and the sample size was 59. 7 The t test and the Mann‒Whitney U test 8 were used to compare data between groups. Pairwise comparisons between peripheral venous access and central venous access were performed by chi-square segmentation. p < 0.05 indicated that a difference was statistically significant, and the chi-square segmentation was α’ = 2*α/K(K−1) = 0.003.
Results
Analysis of patient baseline data and clinical characteristics
A total of 350 patients with hematological malignancies were recruited from the Department of Hematology, Huashan Hospital Affiliated to Fudan University. The patients were divided into PICCs and PORTs groups based on the intravenous infusion method. There were no significant differences in age, sex, hypertension status, diabetes mellitus status, or smoking history between the two groups (p > 0.05). Among the hematological malignancy types, there was no significant difference in the number of lymphoma, leukemia or multiple myeloma patients between the two groups (p = 0.085) (Table 1).
Clinical features of the overall cohort stratified by the type of implanted device.
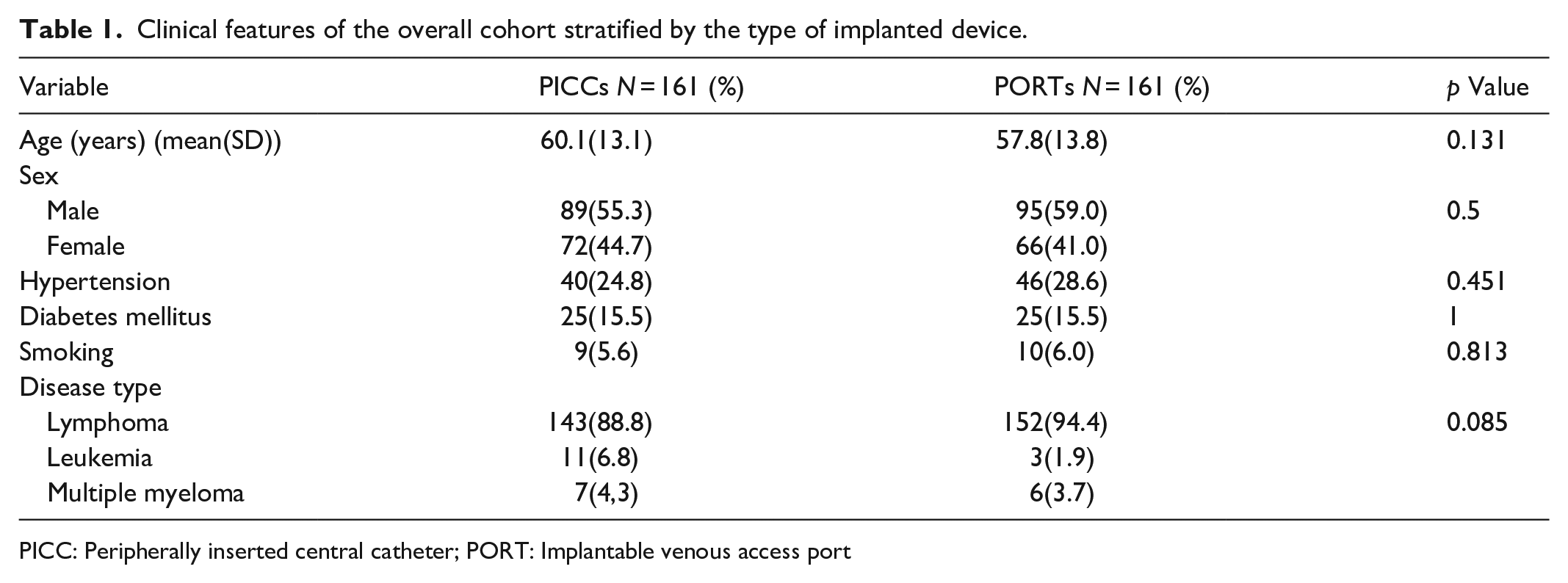
PICC: Peripherally inserted central catheter; PORT: Implantable venous access port
Comparison of DVC-associated complications
The two groups were compared for DVC-associated complications (Table 2). The total relative risk (RR) of serious catheter-related adverse events in patients who underwent PICCs placement was 8.3 [3.0–22.8] compared with those who underwent PORTs. Furthermore, we summarized the RRs of catheter-related venous thrombosis (5 [1.1–22.5]) and infection (11.5 [2.8–48.0]) in patients who received PICCs compared to those who received PORTs. Therefore, for Chinese patients with hematological malignancies, the incidence rate of DVC-associated complications was significantly higher in the PICCs group than that in the PORTs group.
Comparison of common deep vein catheterization-associated complications between the two groups.

PICC: Peripherally inserted central catheter; PORT: Implantable venous access port; RR: relative risk.
Comparison of DVC-associated complications for different surgical approaches
To compare the DVC-associated complications for different puncture approaches, the DVC-associated complications for each approach were summarized (Table 3). The total RR of severe catheter-related adverse events in the peripheral vein (PV) was 8.1 [2.9–22.3] compared with that in the central vein (CV) puncture approach. Furthermore, we summarized the RRs of catheter-related venous thrombosis (9.8 [1.2–75.8]) and infection (7.5 [2.3–24.6]) in the PV group compared to those in the CV group. In conclusion, the rate of complications was greater in the PV puncture group than in the CV group.
Comparison of catheterization-associated complications for different puncture approaches.

BV: Basilic vein; CV: Central vein; IJV: Internal jugular vein; MCV: Median cubital vein; PV: Peripheral vein; RR: relative risk; SV: Subclavian vein.
The R*C test value between the surgical approaches was 44.291 (p < 0.0001), indicating that the difference in DVC-associated complications between the approaches was significant (Table 4). To clarify the differences in DVC-associated complications among the different surgical approaches, we performed chi-square segmentation. The following results were obtained: χ2 (internal jugular vein versus basilic vein) = 22.002 (p < 0.0001) and χ2 (subclavian vein versus basilic vein) = 28.940 (p < 0.0001). These results indicated that the incidence rates of DVC-associated complications were significantly greater for the basilic vein approach than for the subclavian or internal jugular vein approaches. From the view of puncture approach, PORTs are more reliable than PICCs.
Comparison of the different approaches by chi-square segmentation.

Discussion
PICCs and PORTs are the most common venous access methods for chemotherapy. All patients in the Department of Hematology must have venous access established to complete chemotherapy. We summarized the common DVC-associated complications and found that the incidence rates of common DVC-associated complications were higher in the PICCs group than in the PORTs group. In addition, we analyzed the effects of different surgical approaches on common DVC-associated complications. The incidence rates of common DVC-associated complications between the internal jugular vein, subclavian vein, basilic vein and median cubital vein approaches were significantly different, and the incidence rates of common DVC-associated complications were significantly higher for the PV (basilic vein) approach than for the CV (internal jugular vein and subclavian vein) approach.
In general, there were more DVC-associated complications in the PICCs group than in the PORTs group, consistent with the results of previous studies. In retrospective studies or real-world studies, researchers have found that the incidence rates of complications are higher for PICCs placement than for PORTs catheterization and that PORTs are the first choice for venous access for chemotherapy in cancer patients.9–12 Some scholars have systematically summarized retrospective or prospective studies. In addition, regarding the PORTs insertion site, the complication rate was lower for chest wall ports than for arm ports, indicating that the chest wall is the best PORTs insertion site. 13
Catheter-related thrombosis, a common DVC-associated complication, can cause pulmonary embolism; therefore, this complication is a focus of comparative studies of PICCs and PORTs. There are some large randomized controlled trials to clarity the relationship between PICCs and PORTs. Jon Moss et al. 14 performed an open multicenter randomized trial to compare Hickman-type tunneled catheters, PICCs and PORTs. They discovered that PICCs were inferior to PORTs in terms of complications. Swedish scholars Knut Taxbro et al. 15 designed a large randomized controlled open trial to explore common DVC-associated complications after PICCs and PORTs catheterization. They recruited a total of 399 breast and colon cancer chemotherapy patients who were randomly assigned to receive PICCs placement or PORTs catheterization. They found that the incidence rates of catheter-related thrombosis and other complications were higher for PICCs placement than for PORTs catheterization. Additionally, Florian Clatot et al revealed that PICCs are connected to a greater risk of catheter-related significant adverse events. 16 On this basis, Chinese scholars Pengpeng Wang et al. summarized and analyzed the results of 22 studies and found that the incidence rate of catheter-related thrombosis was higher after PICCs placement than after PORTs. Subgroup analysis revealed that the incidence rate of catheter-related thrombosis was higher after PICCs placement than after PORTs placement in non-Asian countries but that the incidence rates of catheter-related thrombosis after PICCs and PORTs catheterization were not significantly different among Asian countries. Additionally, in a retrospective study focusing on diffuse large B-cell lymphoma, Pénichoux et al. 17 reported that the incidence rates of catheter-related thrombosis and infection 6 months after PICCs placement were greater than those after PORTs placement. Two other meta-analyses focusing on cancer chemotherapy reached similar conclusions.18,19 In general, previous large studies and our study confirmed that the incidence rate of catheter-related thrombosis after PICCs catheterization is lower than that after PORTs, indicating that the complication rates of the two procedures should be considered when choosing the venous access for chemotherapy.
In addition to complications, the cost‒benefit ratio is an important factor to consider when choosing the best venous access for chemotherapy. Some scholars propose that although the cost of PORTs catheterization is greater than that of PICCs, the complication rate is lower; therefore, PORTs catheterization is still a good option for venous access for chemotherapy. 10 In addition, some scholars have studied the cost‒benefit ratio of the two approaches in different periods. At 3–9 months after surgery, the cost‒benefit ratio was greater for PICCs catheterization than for PORTs catheterization; at 9–12 months after surgery, the cost‒benefit ratio was greater for PORTs catheterization than for PICCs catheterization. 20 The decrease in the cost‒benefit ratio for PICCs placement at 9‒12 months after surgery might be due to the increased cost of maintenance complications. 21 Therefore, PORTs are suitable for medium- to long-term intravenous chemotherapy applications, 22 and the total cost of the long-term application of PORTs is lower than that of PICCs. 23 To clarify the cost‒benefit ratio relationship between PORTs and PICCs, Moss et al. 14 designed a large randomized controlled open trial that included 1061 patients who were randomly assigned to the Hickman catheter, PICCs and PORTs groups; through a 1-year follow-up, they found that the cost‒benefit ratio and safety were greater for PORTs than for Hickman catheters and PICCs. Although the cost of PORTs catheterization is greater than that of PICCs, considering the cost of maintenance complications caused by medium- and long-term catheterization, the overall cost‒benefit ratio of PORTs is greater than that of PICCs.
The primary limitation to the generalization of these results is that the outcome estimates in the model are based on prospective observational studies, while biases may influence the model estimates. A further weakness was that the choice of central access would be influenced by patients’ economic status due to the incomplete medical insurance system in China. This circumstance may induce bias that the outcome of catheterization is affected by the economic situation. Besides, we were researching chest ports lacking examining PICC-PORTs and arm PORTs, so we couldn't fully evaluate the safety of PICCs and PORTs. We have tried our best to avoid these biases, and we are planning to perform randomized controlled trials in China to overcome these limitations.
Therefore, the results of our study, together with those of previous studies, demonstrated that the rate of DVC-associated complications (thrombosis, infection) in both hematological and nonhematological malignancies was higher after PICCs catheterization than after PORTs. Moreover, the incidence rate of common DVC-associated complications was significantly higher in patients who received peripheral venous access than in patients who received central venous access. Therefore, implantation of PORTs is the preferred method of venous access for chemotherapy for patients with hematological malignancies.
Conclusion
In summary, PORTs are safer than PICCs for Chinese patients with hematological malignancies. The implantation of PORTs could be firstly considered for systematic anti-cancer treatment.
Footnotes
Acknowledgements
We thank every one of the patients who took part in the clinical study. We also thank the Ethics Committee for the continued support of the cohort, as well as the research nurses for their dedication and tireless efforts.
Author contributions
Aiwen Lu and Min Hu collected the data and drafted the manuscript. Xin Qi and Yujing Zhao assisted in drawing the figures and tables. Yijun Huang guided the group members in completing the publication. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was sponsored by a grant from the Shanghai Sailing Program (Grant No. 21YF1404900).
Ethics approval
Ethical approval for this study was obtained from ETHICAL REVIEW BOARD OF HUASHAN HOSPITAL AFFILIATED TO FUDAN UNIVERSITY (2022-1097).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.