
Abstract
Background:
Dengue fever transmitted primarily by Aedes mosquitoes is a growing health concern in Sudan, particularly in Port Sudan. Given the resource strain imposed by the ongoing war, this study aimed to evaluate physicians’ knowledge, attitudes, and practices (KAP) regarding dengue fever. Our central hypothesis was that sociodemographic factors, educational history, and specialized training would significantly influence KAP scores within this challenging conflict environment.
Methods:
A cross-sectional study was conducted among physicians working at Osman Digna Hospital, Port Sudan Teaching Hospital, and Sea Corporation Hospital from July to September 2024. The calculated sample size was 150 physicians, distributed across the three hospitals using a stratified sampling technique. Data collection was conducted by using a validated and reliable questionnaire from the literature. The questionnaire was developed in Google Forms and distributed to physicians via social media and email. Data were analyzed using the Statistical Package for the Social Sciences software, IBM Corp. IBM SPSS Statistics for Windows, Version 23. Armonk, NY: IBM Corp.
Results:
Of the 150 respondents, 53% were female with a mean age of 30.5 (±4.8) years. The median years of experience were 2 (interquartile range, 1–5) years. Only 37% had participated in dengue fever workshops. Despite this, 55% exhibited good knowledge, 94% had a positive attitude, and 77% demonstrated appropriate practices regarding dengue fever. Significant associations were observed between workplace and knowledge (p value = 0.044), workshop attendance and physician practices (p value = 0.05), and a highly significant association between knowledge and practices (p value = 0.010).
Conclusion:
Most physicians in Port Sudan demonstrated positive attitudes and good practices for dengue prevention and control. While overall KAP was moderately good, persistent and significant knowledge gaps were identified, particularly regarding the identification of less common symptoms, criteria for severe dengue, and effective vector control measures. These gaps were especially pronounced among those who had not attended dengue fever workshops.
Introduction
Dengue fever is a mosquito-borne viral infection transmitted primarily by Aedes mosquitoes, a major global health threat. Its epidemiology is influenced by various factors, including climate, urbanization, population density, and socioeconomic conditions.1–3 The geographic distribution of dengue has expanded rapidly, with tropical and subtropical regions experiencing the most substantial burden. This expansion is attributed to factors like increased international travel, globalization, and climate change, which have provided ideal breeding conditions for Aedes mosquitoes,2,4 it is caused by any of the four serotypes of dengue virus and is a leading cause of morbidity and mortality globally. 5 Accurate identification and early treatment of dengue patients can help reduce medical complications and mortality rates. 6 Dengue fever transmission is primarily facilitated by the Aedes aegypti and Aedes albopictus mosquitoes, which have demonstrated an increasing geographic distribution. 5 These vectors thrive in urban environments, where they breed in artificial containers and bite during the day. 7 It is transmitted from person to person via the bite of an infected mosquito. Of these, the primary vector is Aedes aegypti, which is a highly domestic mosquito, a day biter, breeding in water containers in peri-domestic areas. Its eggs could survive without losing moisture in dried condition for months and, with the first opportunity of contact with water, the life cycle begins. Aedes albopictus is a secondary dengue vector, confined to a few regions in the world. 8 Dengue fever presents with a diverse spectrum of clinical manifestations. A typical case often begins with a sudden onset of high fever, which can range from mild to severe intense headache, particularly behind the eyes (retro-orbital pain), is a hallmark symptom, often accompanied by severe muscle and joint pain, commonly referred to as “break bone fever.” A characteristic skin rash typically develops, which can vary from a maculopapular eruption to a more extensive rash. Fatigue, loss of appetite, and nausea are common accompanying symptoms. 8 In severe cases, dengue can progress to dengue hemorrhagic fever (DHF) or dengue shock syndrome (DSS). Warning signs of DHF include persistent vomiting, severe abdominal pain, rapid breathing, bleeding gums, nosebleeds, or petechiae (small red spots on the skin), and cold, clammy skin. DSS is characterized by shock, rapid, weak pulse, and low blood pressure. Early recognition of these warning signs is crucial as the disease can progress rapidly. 9
Diagnosis is often made clinically based on the patient’s reported symptoms and a physical examination. Tourniquet testing, which involves applying a blood pressure cuff and counting any petechial hemorrhages, can help in the diagnosis. Laboratory methods, including full blood count, cell culture, nucleic acid identification (PCR), and serology, can be used to confirm the diagnosis. 10
Currently, there is no specific antiviral treatment available for dengue fever. 11 The primary focus of treatment is on supportive care to manage symptoms and complications. During the febrile phase, liberal oral fluid administration is essential to prevent dehydration. Paracetamol (acetaminophen) is the preferred antipyretic medication to manage fever. In severe cases of dengue with signs of fluid leakage, intravenous fluid resuscitation using normal (0.9%) saline or Ringer’s lactate is necessary. It’s crucial to consult with a healthcare professional for proper diagnosis and guidance, as the specific treatment approach may vary depending on the severity of dengue and the individual patient’s condition. 12 While no specific treatment exists, strong preventive measures are crucial for combating this disease. 13 Effective dengue prevention requires a multifaceted approach. Vector control is essential for reducing the mosquito population, the primary vector for dengue transmission. This involves eliminating breeding sites, such as stagnant water in containers, tires, and flowerpots, and using larvicides and adulticides to kill mosquito larvae and adults. 12 Personal protection measures are equally important to prevent mosquito bites. These include using insect repellents containing N,N-diethyl-meta-toluamide (DEET), picaridin, or IR3535, wearing long-sleeved clothing and long pants, 14 and using insecticide-treated mosquito nets, especially in sleeping areas. 15 While vector control and personal protection remain the cornerstones of prevention, significant advancements have led to the development and licensing of dengue vaccines (such as Dengvaxia and QDENGA/TAK-003) for use in specific populations and endemic regions globally, marking an important step in comprehensive dengue control efforts.16,17
Community involvement is essential for effective dengue fever prevention. Awareness campaigns can educate the public regarding dengue transmission, symptoms, and preventive strategies. Prompt identification of potential dengue cases is essential for enabling timely diagnosis and intervention. Moreover, engaging the community in initiatives such as source reduction and clean-up campaigns can aid in the eradication of potential mosquito breeding sites. 18 By integrating these strategies, we can markedly alleviate the burden of dengue fever and enhance public health outcomes. Dengue fever constitutes a significant public health issue in Sudan, particularly in the Red Sea state, characterized by a rising incidence and expanding geographic distribution in recent years.
Dengue fever constitutes a significant public health issue in Sudan, particularly in the Red Sea state, characterized by a rising incidence and expanding geographic distribution in recent years. The current instability and ongoing conflict in Sudan have severely strained the healthcare system in Port Sudan, leading to significant internal displacement, infrastructural damage, disruptions in vector control and public health campaigns, and critical scarcity of medical supplies and trained staff. Physicians are among the primary healthcare providers to the community during disease outbreaks; therefore, it is essential to adhere to the management tools outlined in protocols according to guidelines, especially when systemic failures due to conflict drastically raise the risk of misdiagnosis, poor patient outcomes, and increased mortality.
An extensive assessment of physicians’ knowledge, attitudes, and practices (KAP) is crucial for pinpointing areas requiring educational interventions and policy enhancements to improve dengue fever management. 19 This study will evaluate knowledge of dengue fever to assess the efficacy of current training programs and guide the creation of customized educational resources. Furthermore, analyzing physicians’ attitudes toward dengue fever management will uncover potential obstacles to effective treatment and guide the formulation of strategies to foster favorable attitudes among healthcare practitioners. 20 This research will enhance the management of dengue fever and elevate the health of the population in Port-Sudan City. Although research on KAP related to dengue fever has been undertaken in several countries,21–24 no investigation has specifically assessed the KAP of prescribing doctors in Port Sudan under the unique and unprecedented strain of the ongoing conflict. Therefore, this study aimed to evaluate the overall KAP of prescribing physicians regarding the diagnosis and clinical management of dengue fever in Port Sudan City.
Methodology
Study area
Prescribing doctors from Port Sudan Teaching Hospital, Sea Port Corporation Hospital, and Osman Digna Hospital participated in this study.
Port Sudan Teaching Hospital – located in the city center, this major governmental hospital provides comprehensive medical services across multiple specialties, including internal medicine, surgery, pediatrics, obstetrics and gynecology, and radiology. It has a capacity of 400 beds.
Sea Port Corporation Hospital – Situated in the northern part of the city, this hospital offers a variety of healthcare services, including internal medicine, surgery, pediatrics, obstetrics and gynecology, and radiology. It has a capacity of 200 beds.
Osman Digna Hospital – located on Osman Digna Street, this hospital provides a broad range of medical services, including general medicine, surgery, pediatrics, obstetrics and gynecology, ophthalmology, otolaryngology, dermatology, dentistry, and radiology. It has a capacity of 200 beds.
Inclusion criteria
Participants selected for this study were required to meet the following criteria: They must be actively practicing prescribing physicians (e.g. House Officer, Registrar, or Specialist) involved in direct patient care within one of the three designated hospitals (Port-Sudan Teaching Hospital, Sea Port Corporation Hospital, or Osman Digna Hospital) during the specified study period (July to September 2024) and voluntarily participated and provided written informed consent for the research.
Exclusion criteria
Participants were excluded from the study if they were unavailable during the study period or who did not provide written informed consent to voluntarily participate in the study.
Study design and sampling technique
This study was a hospital-based cross-sectional descriptive study conducted from July 2024 to September 2024 using a stratified sampling technique.
The total targeted population for this study consisted of {N = 245} physicians (142 from Port Sudan Teaching Hospital, 52 from Red Sea General Hospital, and 51 from Osman Digna Hospital). The required sample size was calculated using the formula for cross-sectional studies targeting a known (finite) population, which adjusts the sample size to maintain precision given the small population size 25

Z ≡ is the critical value (1.96, consider confidence level = 95%)
P = proportion of the target population (50%)
E = desired margin of error. (5%)
N = number of populations
Using the above formula, the calculated sample size was 150 physicians, distributed across the three hospitals using a stratified sampling technique:
Port Sudan Teaching Hospital: 87 physicians
Sea Port Corporation Hospital: 32 physicians
Osman Digna Hospital: 31 physicians
This manuscript adheres to the Strengthening the Reporting of Observational studies in Epidemiology checklist for cross-sectional studies.
Operational definitions of key variables
Good knowledge: Defined as a participant scoring 70% or more of the total possible correct answers in the knowledge section.
Positive attitude: Defined as a participant scoring 70% or more of the total possible score in the attitude section.
Good practice: Defined as a participant scoring 70% or more of the total possible correct answers in the practice section.
Scores below the 70% threshold were classified as Poor Knowledge, Negative Attitude, or Poor Practice, respectively. 19
Data collection
Data were collected using a validated and reliable 58-item questionnaire adopted directly without modification or adaptation from a previously validated instrument used in similar studies. 19 The questionnaire was developed in Google Forms and distributed to physicians via social media and email. Before distribution, a pilot test was conducted on 10 physicians in Port Sudan City to assess clarity, completion time, and ease of use. Pilot test participants were excluded from the final study. The questionnaire took approximately 10–15 min to complete.
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) software (e.g. IBM SPSS Statistics for Windows, Version 26.0). Descriptive statistics were used to summarize participant demographics and KAP scores. Inferential statistics, including the Chi-square test, were employed to determine associations between KAP scores and sociodemographic variables. All statistical tests were two-tailed, and a level of significance was set at p < 0.05.
Results
A total of 150 physicians were included in the final analysis, and all completed data sets were used without exclusion.
Socio-demographic characteristics of physicians
A total of 150 physicians participated in the study, with a slight majority (53%) being female. The average age of the participants was 30.5 years (standard deviation ± 4.8). The demographic structure indicated a concentration of early-career physicians, with 72.7% reporting only 1–5 years of clinical experience. This is critical, as it highlights a systemic need for readily accessible and standardized foundational training and clinical supervision. Furthermore, the physicians represented a highly varied and largely non-specialized group: core specialties (internal medicine (15%), family medicine (13%), emergency medicine (8%), and pediatrics (4%)) constituted only 40% of the sample, while the remaining 60% were distributed across diverse, non-core fields. This substantial proportion of non-specialist staff treating endemic dengue introduces a critical risk of inconsistent adherence to established clinical management guidelines across the wider hospital workforce. Despite 85% of physicians having practical experience treating dengue patients, only 37% had attended a dedicated workshop on the fever. Regarding sources of information, the high reliance on books and scientific papers (38%) and digital sources (Internet: 21%, social media: 11%) contrasts sharply with the low use of seminars (10%), reflecting the logistical challenges and disruptions to centralized educational programs imposed by the ongoing conflict (Table 1).
Distribution of students according to demographic data (n = 150).

Knowledge about dengue fever
Participants demonstrated a strong understanding of core dengue symptoms, including fever (99%), headache (100%), joint pain (97%), and muscle pain (95%). However, knowledge of less common symptoms varied, with lower recognition of eye pain (66%), skin rash (60%), abdominal pain (69%), diarrhea (41%), dizziness (47%), and conjunctivitis (34%).
Most participants correctly identified Aedes mosquitoes as the main vector (90%), the primary transmission modes (53%), and the urban-rural disease distribution (70%). Additionally, 77% recognized dengue as a reportable disease, and a majority avoided prescribing aspirin (89%) and corticosteroids (84%).
Regarding mosquito control, most physicians identified man-made containers (72%) and stagnant water (70%) as primary breeding sites. They also emphasized personal protective measures, such as using insect repellent (91%) and sleeping under nets (80%; Table 2).
Knowledge of physicians regarding dengue fever (n = 150).

Attitude of physicians toward dengue fever
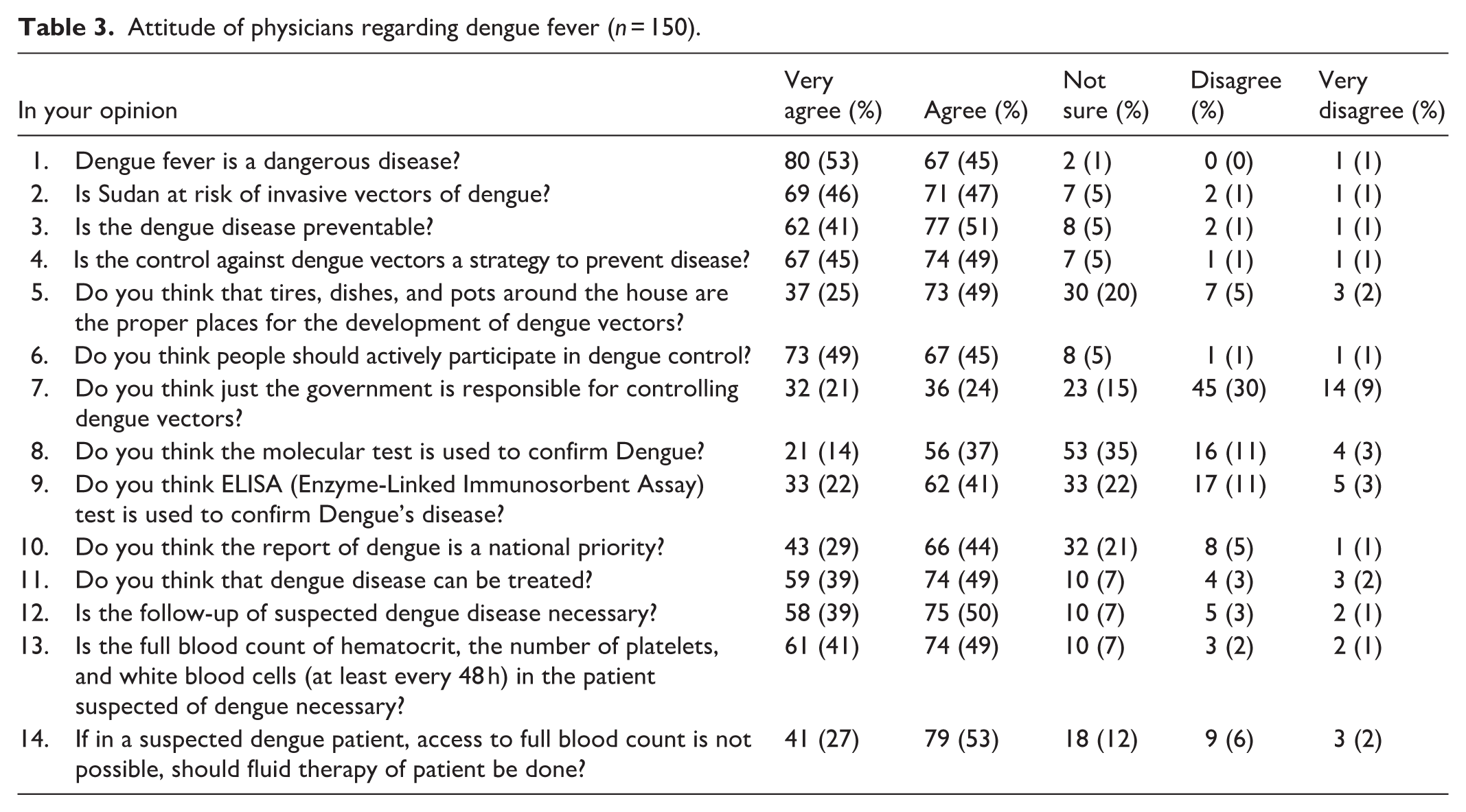
The majority of participants strongly agreed or agreed that dengue fever is dangerous (98%), preventable (92%), and treatable (88%). However, 51% and 63% believed that molecular tests and ELISA tests, respectively, are used to confirm dengue fever. Despite this, most physicians recognized the importance of follow-up (89%) and full blood count monitoring (90%) for suspected dengue cases (Table 3).
Attitude of physicians regarding dengue fever (n = 150).
Practices of physicians toward dengue fever
A significant majority of participants support proactive measures to prevent dengue fever, with 87% advocating for surveying larvae at entry points and 73% supporting the installation of an oviposition trap. Additionally, 77% recognize the importance of entomological monitoring, 85% emphasize human care measures, and 93% prioritize prompt reporting of suspected cases. When addressing local transmission, participants demonstrated familiarity with various control strategies, including fogging (84%), community engagement (89%), larvicides (87%), and personal protective measures such as mosquito nets (80%) and repellents (86%; Table 4).
Practice of physicians toward dengue fever (n = 150).

Overall KAP category
Among the 150 participants, a significant majority (94%) exhibited positive attitudes toward dengue fever. Additionally, 77% (116) demonstrated good practices, while only 55% (83) had adequate knowledge (Table 5).
Overall KAP scores among physicians (n = 150).

KAP: Knowledge, attitudes, and practices.
Association of sociodemographic characteristics with KAP
The relationship between participant demographics and the mean KAP scores was analyzed using the Chi-square test (Table 6).
Association of sociodemographic and training factors with knowledge, attitude, and practices (n = 150).

A significant association was found between workplace and knowledge (p-value = 0.044), suggesting that the hospital setting plays a role in the level of professional knowledge. Furthermore, a marginally significant association was observed between workshop attendance and practice (p-value = 0.058), indicating that specialized training may influence clinical actions. Conversely, other factors such as age, gender, and experience did not show a statistically significant association with overall KAP scores.
Correlation between KAP
The majority of physicians (93.9%) demonstrated adequate knowledge and a positive attitude toward dengue fever. Additionally, 85.4% had adequate knowledge and good practice, with a highly significant association between knowledge and practice (p-value = 0.010; Table 7).
Correlation between knowledge, attitudes, and practices scores (n = 150).

Discussion
Analysis of key findings and contextual interpretation
The study sample was diverse, representing a wide range of medical specialties and job positions. However, it is important to note that the majority of participants were relatively junior physicians, with only 5% being consultants. Internal medicine, family medicine, and emergency medicine doctors are often involved in the early stages of dengue fever care. However, other specialties, like pediatrics and infectious diseases, also play a crucial role.
Only 37% of participants reported having attended dengue fever workshops, indicating a notable training gap among physicians. While this percentage is somewhat higher than that observed in a previous study conducted in Ethiopia, 26 the overall low level of training remains concerning. This finding underscores the critical need for enhanced educational initiatives and increased opportunities for professional development in dengue fever management to better prepare physicians for effective diagnosis and treatment.
A study conducted in Florida demonstrated that the knowledge of physicians toward dengue fever can increase by 19.9% after educational training. 27 This further supports the importance of such training programs.
The finding that 85% of participants had treated patients with dengue fever is significant, indicating a high prevalence of the disease in Sudan, which is in agreement with a study that suggested that physicians in the region are well-versed in recognizing and managing dengue fever. 28
Seventy-three percent of physicians answered “No” to the question, “Is there a vaccine to prevent dengue?” Frame this as a potential gap in global public health knowledge, possibly due to the focus on immediate clinical management and the war’s disruption to non-essential training, while acknowledging that vaccine implementation remains complex.
The results of this study indicate a high level of knowledge among physicians in Port Sudan regarding the most common symptoms of dengue fever, such as fever, headache, joint pain, and muscle pain. This finding aligns with similar studies conducted in Iran and Pakistan, respectively.19,29 Despite this, there are gaps in understanding less common symptoms like eye pain, skin rash, and abdominal pain. While most physicians understand how dengue is spread by Aedes mosquitoes, some still have misconceptions about transmission through blood transfusions. Although most physicians demonstrated appropriate clinical management practices by avoiding aspirin and corticosteroids, the relatively high rate of physicians failing to recognize dengue as a reportable disease is a cause for concern. While physicians demonstrated a strong understanding of dengue prevention and control measures, knowledge gaps persisted regarding the role of certain environments in vector breeding. These findings align with the results from a study on healthcare professionals in Ecuador, Puerto Rico, Texas, and Nigeria.30–33
The core finding, however, revealed a significant deficit in overall professional preparedness, with only 55% of physicians demonstrating adequate knowledge. This low prevalence presents a major risk to the timely and accurate diagnosis of dengue, which is critical for reducing mortality, particularly in a high-prevalence setting like Port Sudan 34 .
These findings are consistent with studies conducted in Iran and Togo,19,34 further emphasizing the importance of ongoing efforts to improve clinical competencies in managing dengue fever. The concurrent finding regarding reliance on self-directed learning methods, also noted in a previous study conducted in Bangladesh, 27 provides crucial contextual insight. This heavy reliance on digital sources, rather than centralized training, is a likely consequence of the logistical challenges and disruption of educational programs imposed by the ongoing conflict, forcing physicians to rely on asynchronous methods. Furthermore, one of the fundamental effects of the armed conflict is the near-total deterioration of Continuous Professional Development programs; the displacement of academic staff and the closure of major medical centers have paralyzed the traditional channels for updating clinical knowledge.
A statistically significant link was established between the physician’s workplace and their knowledge acquisition (p = 0.044). This finding is highly relevant for policy, indicating that the hospital setting – rather than just individual characteristics – is a primary determinant of professional competence. Addressing this requires standardizing training resources and oversight mechanisms to ensure equitable quality of care across Port Sudan.
Crucially, the study established a highly significant association between physician knowledge and appropriate clinical practices (p = 0.010). This finding is the most impactful, as it provides strong empirical evidence that increasing professional knowledge directly translates to improved clinical management in this conflict setting, a finding consistent with research from Florida, 35 which also showed a significant correlation between knowledge and practice.
Finally, physicians in our study exhibited a generally positive attitude toward dengue prevention and control. Notably, the level of positivity in our findings was even higher than that reported in studies from Togo, 36 suggesting that local contextual factors or differences in public health interventions may contribute to these variations.
The present study found that prescribing doctors demonstrated a strong understanding of dengue’s risks and the importance of prevention strategies, prioritizing early reporting and follow-up. While knowledge gaps persisted regarding Sudan’s specific risk of invasive dengue vectors and diagnostic tests, physicians demonstrated a high level of awareness regarding the necessary measures for dengue prevention and control, including vector control strategies, personal protective measures, and community engagement. These findings align with a previous study that assessed the KAP of medical students.35,37
However, despite high levels of both knowledge and attitude, no significant association was found between these two variables (p = 0.956). This indicates that physicians’ attitudes toward dengue fever may not be directly influenced by their level of knowledge.
While attitude and knowledge were not significantly associated in this study, findings from a study conducted in Saudi Arabia, 38 similarly found no correlation between these two variables. In contrast, a study conducted in Indonesia suggested a positive correlation between knowledge and attitudes. 39
Study limitations
This study is subject to several limitations inherent to its design and context. First, its cross-sectional design restricts our ability to establish causal relationships between the sociodemographic factors and KAP scores; the associations observed are correlational.
Second, the reliance on a self-administered questionnaire carries a potential for social desirability bias, where participants may overestimate their knowledge or report practices they believe are professionally expected.
Third, the scope of data collection was severely constrained by the ongoing conflict. This limited the accessible physician population, geographically confining the study to three governmental hospitals in Port Sudan. Consequently, the sample may not represent specialists who fled the region, private sector physicians, or those who received their training in different, non-conflict-affected institutions. This restriction limits the generalizability of the findings and potentially skews conclusions regarding the overall effectiveness of diverse training exposures on physician competency.
Contribution to knowledge and policy implications
This research provides crucial and novel data by evaluating physicians’ preparedness to manage dengue in the unique and highly demanding context of a war-affected, resource-strained environment, where evidence is extremely scarce. The demonstrated link between knowledge and practice (p = 0.010) provides a clear, evidence-based mandate for intervention. Given the operational constraints of the ongoing conflict and the specific nature of the identified knowledge deficits, the key policy recommendation is the urgent development and deployment of targeted, remote-based educational interventions (e.g. mobile-based training or pre-recorded webinars). These initiatives are logistically feasible, despite the war, and necessary to rapidly elevate the clinical competency of the young, non-specialized workforce, thereby improving patient outcomes and public health in Port Sudan.
Conclusion
This study successfully assessed physicians’ KAP regarding dengue fever in the challenging context of Port Sudan amid ongoing conflict and severe resource scarcity. The findings revealed that physicians demonstrated a strong understanding of key dengue symptoms, transmission routes, and clinical management protocols. However, notable gaps were observed in their knowledge of less common symptoms, specific vector transmission pathways, and environmental factors contributing to mosquito breeding. Attitudes toward dengue prevention and control were generally positive, and most physicians reported effective practices in case management.
Because hospitals are under severe strain and resources are limited, there’s a vital need for specialized training that is accessible and adapted for war zones. This kind of training is essential to ensure patient care remains consistent and standardized.
Overall, this research gives health planners important initial data for conflict areas. It shows that while doctors’ knowledge and skills (KAP) are being maintained, they are also very fragile and easily broken under the extreme stress of the conflict.
The statistically significant correlation between knowledge and practice (p = 0.010) highlights the potential impact of targeted educational interventions in enhancing clinical outcomes for dengue fever, and these findings have immediate policy relevance, urging health authorities to prioritize resilient and continuous medical education to safeguard dengue management protocols and clinical outcomes in unstable environments.
This study provides crucial, novel data on dengue management in a resource-limited, conflict-affected environment. We recommend urgent, targeted educational interventions, such as remote-based training, to address these specific knowledge gaps and enhance the clinical and policy response to dengue outbreaks.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251408941 – Supplemental material for Doctors’ knowledge, attitudes, and practices in managing dengue fever amid war: A study in three governmental hospitals in Port Sudan, Red Sea State, Sudan (2024)
Supplemental material, sj-docx-1-smo-10.1177_20503121251408941 for Doctors’ knowledge, attitudes, and practices in managing dengue fever amid war: A study in three governmental hospitals in Port Sudan, Red Sea State, Sudan (2024) by Tasneem Ebrahim, Ali Awadallah Saeed, Wamda Ahmed Ali Allam and Safaa Badi in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251408941 – Supplemental material for Doctors’ knowledge, attitudes, and practices in managing dengue fever amid war: A study in three governmental hospitals in Port Sudan, Red Sea State, Sudan (2024)
Supplemental material, sj-docx-2-smo-10.1177_20503121251408941 for Doctors’ knowledge, attitudes, and practices in managing dengue fever amid war: A study in three governmental hospitals in Port Sudan, Red Sea State, Sudan (2024) by Tasneem Ebrahim, Ali Awadallah Saeed, Wamda Ahmed Ali Allam and Safaa Badi in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank the staff and physicians of the three governmental hospitals in Port Sudan for their participation and cooperation. We also thank the staff of the Department of Clinical Pharmacy, University of Khartoum, and Dr. Safa Badi for supervising this research.
Ethical considerations
Ethical Approval was obtained from the Research Ethical Committee (REC), Clinical Pharmacy department, Faculty of Pharmacy, University of Khartoum (Approval Number: A241224-6). Participants were informed about the study’s purposes, and gathered data would be confidential and used only for research purposes. Written informed consent was obtained from all participants prior to filling out the questionnaire, in accordance with the Declaration of Helsinki.
Author contributions
All authors approve of the final version to be published, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data in the study are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.