
Abstract
Background:
Goiter is a common public health issue in Ethiopia; however, there is not much evidence of it among adolescent girls, especially in Northwest Ethiopia.
Objective:
This study aimed to determine the prevalence and associated factors of goiter in adolescent girls living in the highlands of Northwest Ethiopia.
Methods:
From 5 January to 15 February 2022, 560 adolescent girls participated in this study. A multistage sampling method was used. Participants were checked for goiter using World Health Organization guidelines. Using a quick test kit, the amount of iodine in samples of table salt was determined. After being entered into Epi Info version 7, the data were exported to the SPSS version 22 for statistical analysis. Binary logistic regression was applied. It was decided to set the statistically significant level at p < 0.05.
Results:
In this study, the total prevalence of goiter among adolescent girls was 33.4% (95% CI: 26.3%–39.4%). The odds of goiter were 5.3 times higher among adolescents whose families had a history of goiter (AOR = 5.34, 95% CI: 3.65–9.74). The likelihood of developing goiter was 3.7 times greater among adolescent girls who consumed cabbage at least once per week (AOR = 3.74, 95% CI: 2.46–8.31). In addition, adolescent girls who did not consume meat at all were 3.3 times more likely to develop goiter (AOR = 3.32, 95% CI: 1.95–6.78). Similarly, the odds of getting goiter among adolescent girls from families who use salt with inadequate levels of iodine (0–14) were 9.84 times greater compared to their counterparts (AOR = 9.84, 95% CI: 5.61–26.24).
Conclusion:
In the study area, goiter was very common. Therefore, the district’s health sector should make an effort to raise community knowledge by spreading important messages regarding the proper use of iodized salt and food sources.
Introduction
Goiter, or abnormal growth of the thyroid gland, is one of the most common endocrine illnesses that frequently occur in adolescent girls. Each lateral lobe of the thyroid is larger than the thumb’s terminal phalanges when a patient is being examined for goiter. 1 It shows how a persistent iodine deficiency can serve as a delicate long-term indicator of how well iodine intervention programs are working. 2 Iodine deficiency is the root cause of goiter, which can be clinically detected by visual inspection and palpation. Not only goiter but also hypothyroidism, physical and neurophysiologic defects, and intellectual disability are all consequences of iodine deficiency.
Furthermore, iodine is necessary for the thyroid gland to produce thyroid hormones, which are essential for the body’s development, growth, and control of metabolic processes. 3 Iodine from the day’s meals is transformed into iodide ions and then absorbed throughout the digestive tract. Iodine deficiency diseases (IDDs) are all clinical and subclinical conditions brought on by a lack of iodine. IDD is more common in underdeveloped nations, particularly in mountainous areas. The two most obvious signs of iodine deficiency are goiter and intellectual disability. 4
The majority of Ethiopia’s population, including those in our study area, resides in mountainous regions that are more susceptible to erosion and flooding, which eventually result in the risk of iodine deficiency disorders. 5 Furthermore, due to their rapid physical, psychological, and cognitive growth, as well as the shift from childhood to adulthood, adolescent girls’ demand for iodine is increasing, which makes them susceptible to goiter. 6
Iodine deficiency disorders (IDDs) affect 30% of the world’s population. IDDs affect more than 150 million people worldwide. Global estimates on the prevalence of goiter in general populations found it at 15.8%, 1 with ranges between 4.7% in America and 28.3% in Africa. 7 Moreover, factors such as sex, age, education level, place of birth,8,9 family income, site of residence, knowledge, dietary intake, unprotected water consumption, consumption of goitrogenic foods, and family history can affect the prevalence of goiter.10–12
The majority of previous studies regarding goiter focused on children at school (aged 6–12 years). According to a study conducted in Tach Armachiho District and Gazgibla District, Ethiopia, the overall prevalence of goiter among adolescent girls was 24.1% 2 and 42.5%, 13 respectively. Due to the low dietary iodine concentration, a significant occurrence of goiter was also noted in highland areas compared to lowland areas. Because iodine is often located on the top layer of soil, it can easily leach away owing to erosion, leaving crops lacking iodine. 14 Goiter still affects many adolescent girls, despite the Ethiopian government’s increasing attempts to prevent it, and the factors are different from place to place. In addition, there was not sufficient evidence regarding goiter in adolescent girls in Ethiopia, particularly in the study area. Therefore, it was crucial to assess the prevalence and associated factors of goiter in adolescent girls in the highland area of South Gondar Zone, Amhara Region, Ethiopia.
Materials and methods
Study setting, design, and participants
A community-based cross-sectional study was employed from 5 January to 15 February 2022, in the highlands of the South Gondar Zone, Northwest Ethiopia. The zone is located at a distance of 99 km from Bahir Dar (the capital city of the Amhara region) and 666 km from Addis Ababa (the capital city of Ethiopia). Topographically, the zone is located at 11°50ʹ18.6ʺN and 38°05ʹ58.3ʺE. The 2007 overall population census report estimates that 2,051,738 people are living in this zone. Of those, 1,010,677 are women, and 9.53% are in urban areas. 15 Agriculture, specifically crop-producing subsistence farming, is the common source of income for the community. Adolescent girls (10–19 years old) who live in the study area with their families and who were apparently healthy and willing to participate in the study were included in the study, while those who have severe physical or mental problems and who had only recently moved into the study area (less than 6 months) were also excluded.
Source population
Adolescent girls (10–19 years old) living in the South Gondar zone of Northwest Ethiopia.
Study population
Adolescent girls (10–19 years old) living in the south Gondar zone of selected districts.
Sampling procedure and sample size determination
A total of 563 individuals were chosen using a multistage sampling method. Three highland districts are deliberately chosen from a total of 15 districts. Following the selection of the districts, we chose three highland kebeles within each district. Using random sampling, each sub-district’s households (HHs) were reached. HH lists were gathered from sub-district offices and health extension personnel in each of the locations. We distributed the sample size proportionally among each district and sub-district. For interviews, the chosen HHs were further sorted. If a family had more than one adolescent girl as a research participant, we randomly chose one of them (Figure 1). We determine the sample size using the Epi Info version 7.1.5.0 software and taking into account the prevalence of goiter at 42.5%, 2 with a 5% marginal error and a 95% confidence level. Taking into account the design effect of 1.5, the final sample size was 563.

Schematic presentation of sampling procedure in adolescent girls living in south Gondar zone, Northwest Ethiopia, 2022, n = 563.
Data collection procedures
A semi-structured questionnaire was prepared by reviewing prior published articles.1,2,13,16 A standardized questionnaire that had been pretested on 5% of the study subjects and presented by an interviewer was used to collect the data. The questionnaire was first translated into the study subject’s native language, Amharic, and then retranslated into English during data entry. After receiving their training for 2 days, six experienced nurses with a bachelor’s degree went through the interview process. The data were gathered on sociodemographic traits, adolescents’ eating patterns, and mothers’ and caregivers’ knowledge of the use of iodized salt. A meal frequency questionnaire was used to collect information on the adolescents’ eating habits from both themselves and their mothers or caretakers.
Ultrasonography is the standardized parameter to detect the presence of goiter but the study area is in a low-resource setting. In accordance with the World Health Organization’s (WHO) guidelines, three skilled emergency surgeons performed clinical examinations of the anterior neck to detect thyroid enlargement (goiter). The reported examination results were as follows: grade 0 for no palpable or visible goiter, grade 1 for palpable but not visible goiter, and grade 2 for obvious goiter (1). A rapid test kit for iodine (MBI Kits International) was used to determine the iodine concentration of table salt. Parts per million were used to evaluate the iodine levels in the salt samples (adequate: ⩾15 ppm, medium: <15 ppm, and no iodine: 0 ppm). 11 Adolescent girls with confirmed goiter were directed to medical facilities so they could receive treatment and assistance.
Data analysis
Following data collection, the completion and coding of each questionnaire were checked, and the data were revised and cleaned. Data were entered into the computer using Epi Info version 7 software, which was then exported for statistical analysis into SPSS version 22 software. Descriptive statistics, including frequencies, percentages, and summary measures, were used to summarize the characteristics of the study participants.
Binary logistic regression analysis was used to assess the association between each independent variable and the dependent variable. A 95% confidence interval (CI) and odds ratio were derived. The variance inflation factor (VIF) was used to check for the presence of multicollinearity. No significant multicollinearity (VIF > 10) was found. According to the Hosmer and Lemeshow test (p = 0.08), 13 the model was well fitted with the included variables. The associated factors were identified using the odds ratio and 95% CI, and statistical significance was declared at p = 0.05.
Ethical considerations
The research ethics review committee of Debre Tabor University’s College of Health Sciences provided ethical approval and permission (Ref No. CHS/3234/2013). After the university gave its approval, a letter of support from Debre Tabor University was used to inform the study’s settings regarding the purpose of the study. The goal of the study was then explained to each participant, and his or her right to refuse to participate was respected. Since no personal identifiers were used and the collected data were given to a third party, the confidentiality of the information was maintained.
Results
Table 1 shows the sociodemographic characteristics of participants.
Sociodemographic characteristics among adolescent girls and their parents/caregivers in South Gondar District, Amhara, Ethiopia, 2022 (n = 560).

Out of 563 sampled adolescent girls, 560 of them with their mothers/caregivers participated in the study (response rate 99.5%). The mean age was 16.47 years, with an SD of ±1.75; 465 (83% of the participants) lived in rural areas; 485 (86.6% of their fathers) were farmers; and 275 (49% of their mothers) were unable to read and write (Table 1).
This study reported that millet and barley were relatively frequently consumed food items by adolescent girls. Thus, at least once a week, 94 (16.8%) and 70 (12.5%) of the adolescent girls consumed millet and barley, respectively. However, they consumed a rare amount of milk and maize (Table 2).
The frequency of food consumption and utilization of iodized salt among adolescent girls in South Gondar District, Amhara, Ethiopia, 2022 (n = 560).

The total prevalence of goiter among adolescent girls was 33.4% (95% CI: 26.3%–39.4%), and grade 1 and grade 2 goiters accounted for 25.2% and 8.2%, respectively. In the age ranges 10–14 and 15–19, the prevalence of goiter was nearly identical 33.1% and 33.7%, respectively; however, it was greater among adolescent girls who lived in rural than urban areas, that is, 35.7% and 22.1%, respectively. Goiter was more common in adolescent girls who consumed millet (54.3%) and cabbage (63.1%) at least once a week. Furthermore, for adolescent girls who did not consume milk, meat, or eggs, the prevalence of goiter was greater (29.9%, 37.8%, and 37.2%), respectively. In addition, adolescent girls who used inadequately iodized HH salt (<15 ppm) had a higher prevalence of goiter (53.9%) (Table 3).
Goiter prevalence distributions by sociodemographic and feeding-habit characteristics among adolescent girls in South Gondar District, Ethiopia, 2022 (n = 560).

The odds of developing goiter among adolescent girls with a family history of goiter were 5.3 times (AOR = 5.34, 95% CI: 3.65–9.74) higher as compared to their counterparts. Likewise, adolescent girls who consumed cabbage at least once a week had 3.7 times higher odds of developing goiter (AOR = 3.74, 95% CI: 2.46–8.31) as compared to their counterparts. On the other hand, those who did not consume any meat were 3.3 times more likely to develop goiter (AOR = 3.32, 95% CI: 1.95–6.78). Furthermore, the odds of developing goiter were 9.84 times higher in adolescent girls who used home salt with an insufficient amount of iodine (<15) than in their counterparts (AOR = 9.84, 95% CI: 5.61–26.24) (Table 4).
Factors associated with goiter among adolescent girls in South Gondar District, Ethiopia, 2022 (n = 560).
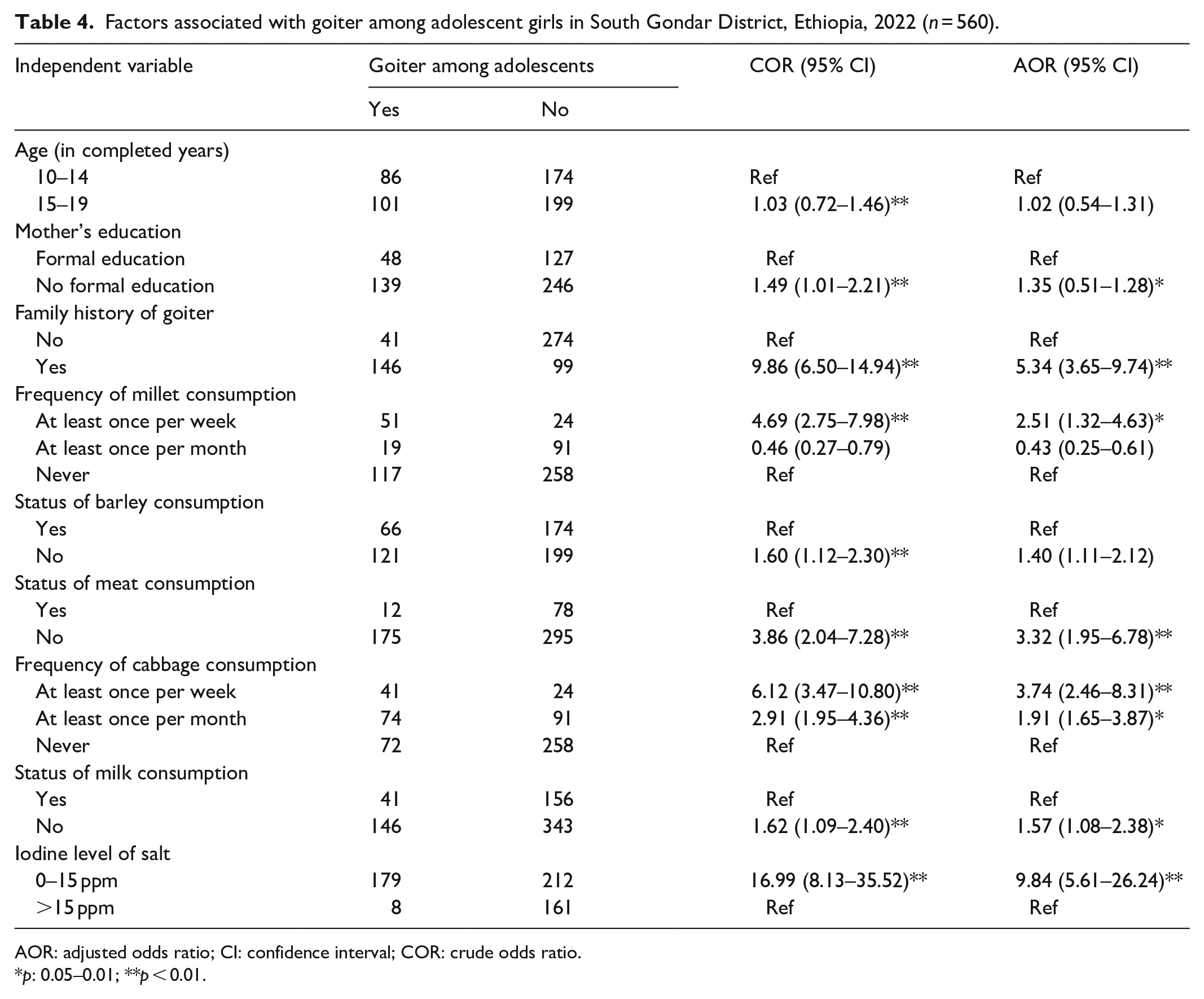
AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio.
p: 0.05–0.01; **p < 0.01.
Discussion
Goiter has several frequent causes, one of which is iodine deficiency. If the gland does not have enough iodine, it cannot produce adequate thyroid hormone. “Thyroid hormone deficiency leads to increased secretion of thyroid stimulating hormone from the pituitary.” As the thyroid struggles to keep up with the need for thyroid hormone synthesis, it gradually grows larger (develops a goiter). 17
Since 2011, Ethiopia has practiced the widespread iodization of salt, and the nation has more than 89% of its HH salt iodized. 18 However, according to the WHO guidelines, the prevalence of goiter in this study was relatively high. 1 The high prevalence of goiter observed in this study despite the use of iodized salt in more than 85% of HHs might be because of the reduced iodine bioavailability, either due to iodine loss from iodized salt or due to cooking. Improper storage of iodized salt, such as exposure to sunlight and a humid atmosphere, reduces the iodine content of both packaged and open salt brands. Iodine loss also occurs during cooking, depending on the type of cooking method and the time of adding salt.19,20
The prevalence of goiter among adolescent girls aged 10–19 years in the study area was 33.4%, which was lower than the prevalence found in four Ethiopian zones, including Metekel (39.4%), 21 Gazgibla (42.5%), 13 Wolaita and Dawro Zones (60.9%), 11 and North Shewa Zone (50.4%). It is also lower than in other studies, such as those conducted in Bangladesh (44%), 22 Rawalpindi (57.1%), and Pakistan (57.1%). 23 Variations in topography and dietary practices may be to blame for this discrepancy. For instance, the community’s dietary history in Wolaita and Dawro Zones, Ethiopia, depends on frequent and substantial consumption of cassava (81.3%) and limited use of iodized salt. 11 In addition, the discrepancies could result from various study settings and study periods.
“The current study observed a higher prevalence of goiter among adolescent girls compared to studies from Tach Armachiho District, Ethiopia”. The different topographies could be the cause of this discrepancy. Additional reasons for the discrepancy were explained, as this study was conducted in a high-altitude region that had inadequate soil conservation over an extended period and contributed to the evaporation of the iodine-rich soil layer, revealing the layer below that was deficient in iodine.
Adolescent girls who reported a family history of goiter were about five times more likely to have it compared to their counterparts. This finding is consistent with a previous study conducted in northwestern Ethiopia. 9 Iodine deficiency among various population segments that is intergenerational in many parts of the country due to either poverty or low coverage of the national salt iodization program could be used to explain the consistency in findings regarding the associations between family history and goiter among adolescent girls in Ethiopia.24,25
In addition, according to the WHO, for the effective eradication of the iodine deficiency disorder or goiter, 90% of the HHs in a community should have access to salt with an iodine content of at least 15 ppm. 26 Adolescent girls who consumed salt with insufficient iodine were nine times more likely to develop goiter than their counterparts were. This is consistent with other study results.9,27 This could be a result of the fact that adequately iodized salt is the primary treatment for IDDs and has both preventive and curative effects for iodine-deficient disorders or goiter.
Limitation
The study’s cross-sectional design prevents it from demonstrating the temporal relationship between the independent and dependent variables. Thyroid ultrasound and autoimmune antibodies to check for thyroid autoimmune disease were not assessed. Due to the dietary habits questionnaire being based on recall knowledge, there is a possibility of recall bias.
Conclusions
Goiter prevalence remains high and is a significant public health concern in the Gondar Zone District. The development of goiter in adolescent girls was positively associated with having a family history of goiter, eating cabbage and millet at least once a week, not eating meat at all, and having inadequate iodine levels in HH salt. Therefore, the health sector should concentrate on spreading information to raise community awareness of how to prevent goiter using iodized salt and eating iodine-rich foods. The Ethiopian government should implement the iodine prophylaxis program by raising public awareness in the community, mainly in the highland areas.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241229643 – Supplemental material for Prevalence of goiter and associated factors among adolescent girls in the highland area of Northwest Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121241229643 for Prevalence of goiter and associated factors among adolescent girls in the highland area of Northwest Ethiopia by Assefa Agegnehu Teshome, Berhanu Kindu Ashagrie, Atalo Agmas Ayenew, Misganaw Asmamaw Mengstie, Yalew Melkamu Molla, Nega Dagnaw Baye, Agmas Wassie Abate, Asaye Alamneh Gebeyehu, Taklo Simeneh Yazie, Ermias Sisaye Chanie, Amare Kassaw Wolie, Fitalew Tadele Admasu and Gashaw Walle Ayehu in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Debre Tabor University for providing ethical clearance and funds to conduct this study. We also forward our great thanks to the data collectors. The authors would like to extend their gratitude to the study participants.
Authors’ contributions
AAT designed the study and was involved in data collection, supervision, and data processing. AAT, BKA, GWA, MAM, YMM, TSY, NDB, ESC, AAA, AWA, AKW, and FTA have prepared the manuscript and cleaned, analyzed, and interpreted the data. The final manuscript has been read, approved, and critically reviewed by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Debre Tabor University raised the funds for data collection only.
Availability of data and materials
The data set and materials used in this study can be obtained from the corresponding author upon reasonable request.
Ethics approval
The research ethics review committee of Debre Tabor University’s College of Health Sciences provided ethical approval and permission (Ref No. CHS/3234/2013).
Informed consent
Adolescent girls who are 18 years old and above provided written informed consent for participation in the study, and participants under the age of 18 acquired consent from their parents or legal guardians.
Consent for publication
Not applicable.
Trial registration
Not applicable.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.