
Abstract
Background:
Menstruation is a natural phenomenon which is an indicator of women’s health that occurs throughout the reproductive years of every female. This phenomenon is unique to the females and governed by the girl’s general health condition, genetic, socioeconomic, and nutritional factors. Although it is a normal physiological process, most females experience some degree of pain and discomfort in their menstruation period. Even though there are limited studies so far reported about the issue in some other parts of the country, there is no scientific evidence in the present study area.
Objective:
To assess menstrual-associated discomfort and associated factors among undergraduate students in Ambo University, Central Ethiopia, 2018.
Methods:
Institution-based cross-sectional study was conducted at Ambo University from 30 March to 30 April 2018. Stratified sampling technique was used and 748 study participants were randomly selected from faculties using a multi-stage sampling procedure. Only data from 713 study participants were entered into EpiData 3.1 and analyzed using SPSS version 20.0 software. Logistic regression was used to associate factors with menstrual-associated discomfort. All statistical tests were considered as significant at a p-value of < 0.05.
Result:
The prevalence of menstrual-associated discomfort was found to be 68.6%. The variables age (Being younger) (adjusted odds ratio = 3.9 (95% confidence interval: 1.28, 11.78)), Tigire ethnicity (adjusted odds ratio = 2.4 (95% confidence interval: 1.02, 5.75)), unmarried (adjusted odds ratio = 2.1 (95% confidence interval: 1.21, 3.76)), smokers (adjusted odds ratio = 2.2 (95% confidence interval: 1.12, 4.29)), drinking caffeine (adjusted odds ratio = 1.8 (95% confidence interval: 1.17, 2.74)), amount of flow (adjusted odds ratio = 2.4 (95% confidence interval: 1.28, 4.62)), and duration of pain (adjusted odds ratio = 4.2 (95% confidence interval: 1.93, 9.29)) were significantly associated with menstrual-associated discomfort.
Conclusion:
This study revealed that majority of the participants was experienced with menstrual-associated discomfort. As the tendency of smoking cigarettes, drinking caffeine, and amount of flow is increased, menstrual associated discomfort is increased. Therefore, specific plan of action and support is urgently needed in order to enlighten and treat menstrual-associated discomfort.
Introduction
Menstruation is a natural phenomenon which is an important indicator of women’s health that occurs throughout the reproductive years of every woman. It is one of the most important changes occurring among girls during the adolescent year, which is the cyclical shedding of endometrium, every 28 ± 7 days in response to hormones.1–3 It has been shown that menstrual fluid contains substances that enhance uterine contraction, for many girls physical problems can arise in relation with menstruation such as dysmenorrheal, weight gain, headache, backache, breast tenderness, mood swings, and depression. Disorders in cycles or its irregularities are major gynecological problems among female adults, especially adolescent, and a major source of anxiety to them and their family.4,5 Menstrual discomfort is a common condition in women during their reproductive years, affecting between 60% and 80% of women. Among these women, 8%–18% experience very intense discomfort, to the point of causing disruption in their normal activities. 6 Menstrual discomfort is a very common and serious problem that can often directly affect the quality of life for women, interfering in activities such as working or studying.6,7 Different studies confirmed that the most frequent menstrual disorders are polymenorrhea, oligomenorrhea, and dysmenorrhea.8,9 Study conducted in Ethiopia among high school students in Addis Ababa showed the prevalence of menstrual-associated discomfort was 65.6%, and in Nigeria, it was found to be 66.2%.10,11 Study conducted in Bahir Dar University, Ethiopia, found the prevalence of dysmenorrhea and premenstrual syndrome to be 85.1% and 72.8%, respectively. 12 In other studies, the prevalence of dysmenorrhea was 80% in Hong Kong and 84% in Thailand. In another study among secondary school students of Northern Ethiopia, the prevalence of dysmenorrhea was 72%; in Nigeria, it was 64%; and in Mexico, it was 48%.12–17 Other studies showed higher prevalence of dysmenorrhea: 88% in Turkey, 93% in Taiwan university students, and 93% in Australian high school students.18–20 Menstrual disorders study in college students showed that the prevalence of oligomenorrhea in this was 11.3%, and that of amenorrhea was 2.6%. Significant factors associated with oligomenorrhea or amenorrhea in this group were weight loss (greater than 20 pounds) and jogging. 21
Despite previous studies have been conducted in other parts of the country (Ethiopia), no recent study was reported about the magnitude and factors associated with menstrual-associated discomfort in the present study area. So that, scientific investigation is crucial to provide adequate epidemiological data for the government and stockholders to give emphasis about the issue which will have societal and economic benefits for the region and the nation at large. Therefore, the main objective of this study was to assess menstrual-associated discomfort and associated factors among undergraduate students in Ambo University, Central Ethiopia, 2018.
Methods
Study design and settings
The study was conducted in Ambo University form March to April 2018. Ambo University is located about 212 km West of Addis Ababa, the Capital City of Ethiopia. Ambo University is one of the foremost higher learning institutions with significant contributions in the country’s overall development since its establishment in 1939 as agriculture college. An institution-based cross-sectional study design with a quantitative study approach was used. A multi-stage cluster random sampling strategy with a stratified sampling technique was employed.
Participants
All female students of Ambo University during the data collection period were the source population and all regular undergraduate female students in Ambo University who met the inclusion criteria were the study population. All female students who can menstruate were included in the inclusion criteria, while students with serious illness and pregnancy were excluded.
Variables
The dependent study variable was menstrual-associated discomfort and the independent variables were sociodemographic characteristics (which includes age, religion, ethnicity, and marital status), gynecological and obstetric variables (which includes age at menarche, period of regularity, duration of bleeding, family history of menstrual pain, and pain level), and lifestyle of the participants (coffee drinking, physical activity, smoking, and body mass index (BMI)). After this, menstrual-associated discomfort was evaluated based on the participants’ self-reported history of pain level.
The participants were asked using dichotomous question whether they feel discomfort during menstruation or not. They were asked to answer this dichotomous question as “yes” or “no.” Like, “do you feel discomfort at all times in your menses?” Similarly, the participants were asked whether the nature of physical activity was “very low active” or “low active” or “highly active” or “moderately active” using structured questionnaires.
Sample size calculation
The sample size was calculated using a single population proportion formula using expected proportion of prevalence (P) of menstrual-related discomfort (MRD) among students 0.5, margin of error 0.05, α = critical value at 95% confidence interval (1.96) with a design effect of 2, and calculated as

Since, the population size was less than 10,000, we have used population correction formula

where N is the total population of female students in Ambo University
Then, n =
Using design effect of 2, the sample is determined to be 340 × 2 = 680 + 10% non-response rate; the final sample is 748. A multi-stage sampling strategy with a simple random sampling technique was employed. The sampling technique was described as follows: first five colleges were selected randomly using lottery methods. From the five colleges, 15 departments were selected by the same technique. Then, the total sample size was allocated proportionally to each of the selected departments using proportional allocation of the sample size to the total number of the selected departments. Simple random sampling technique was applied to select study units from the list of female students in each department. Prior to the actual data collection, pre-test was conducted by taking 5% of the total sample size (748).
Ethical approval was obtained from the research and review committee of School of Medicine, Debre Markos University. Since it is not a clinical trial, the type of consent obtained was verbal informed consent, which was waived by the Review committee.
Data collection
Data were collected by interviewing participants using self-administered questionnaires which were pilot-tested before undertaking the study. Three diploma nurses were recruited as data collectors based on having previous experience of data collection, and one BSc midwife nurse was recruited as supervisor.
Statistical analysis
Quantitative data were coded, edited, cleaned, and entered into EpiData 3.1 and then exported to SPSS version 20 for analysis. The data were presented using texts, tables, and charts. Both bivariate and multivariate logistic regression analyses were conducted to identify independent factors associated with menstrual associated discomfort. All variables which showed statistical significance in the bivariate analysis with a p-value of < 0.25 were included in the multivariate logistic regression model to determine the independent contributing factors associated with menstrual associated discomfort. A p-value < 0.05 was considered as statistically significant.
Results
A total of 713 participants completed the questionnaire giving a response rate of 95.32%. The average age of the participants was 21.13 ± 2.15 years (17–28). The magnitude of menstrual associated discomfort was found to be 489 (68.6%). The sociodemographic characteristics of the participants are indicated in Table 1. Majority of them (394 (55.3%)) were in the age range of 20–22 years. From the participants, majority (351 (49.2%)) were orthodox Christian followers, followed by protestants (204 (28.6%)). Regarding the marital status, 614 (86.1%) were single, while the rest (99 (13.9%)) were married. The frequency distribution of the lifestyle-associated characteristics of the study participants—which includes BMI, smoking status, alcohol consumption, sleeping hours, and physical activity—was presented in Table 2. As indicated in Table 2, more than half (497 (69.7)) of the participants had a BMI of 18.5–24.9 kg/m2. Majority of the participants (299 (41.9%)) had very low type of physical activity. Regarding coffee drinking, most of the participants (324 (45.4)) drank 1–3 cups of coffee per day. Sociodemographic and lifestyle-associated variables associated with menstrual discomfort among undergraduate students were indicated in Table 3.
Frequency distribution of sociodemographic characteristics of undergraduate students, Ambo University, Central Ethiopia, 2018.
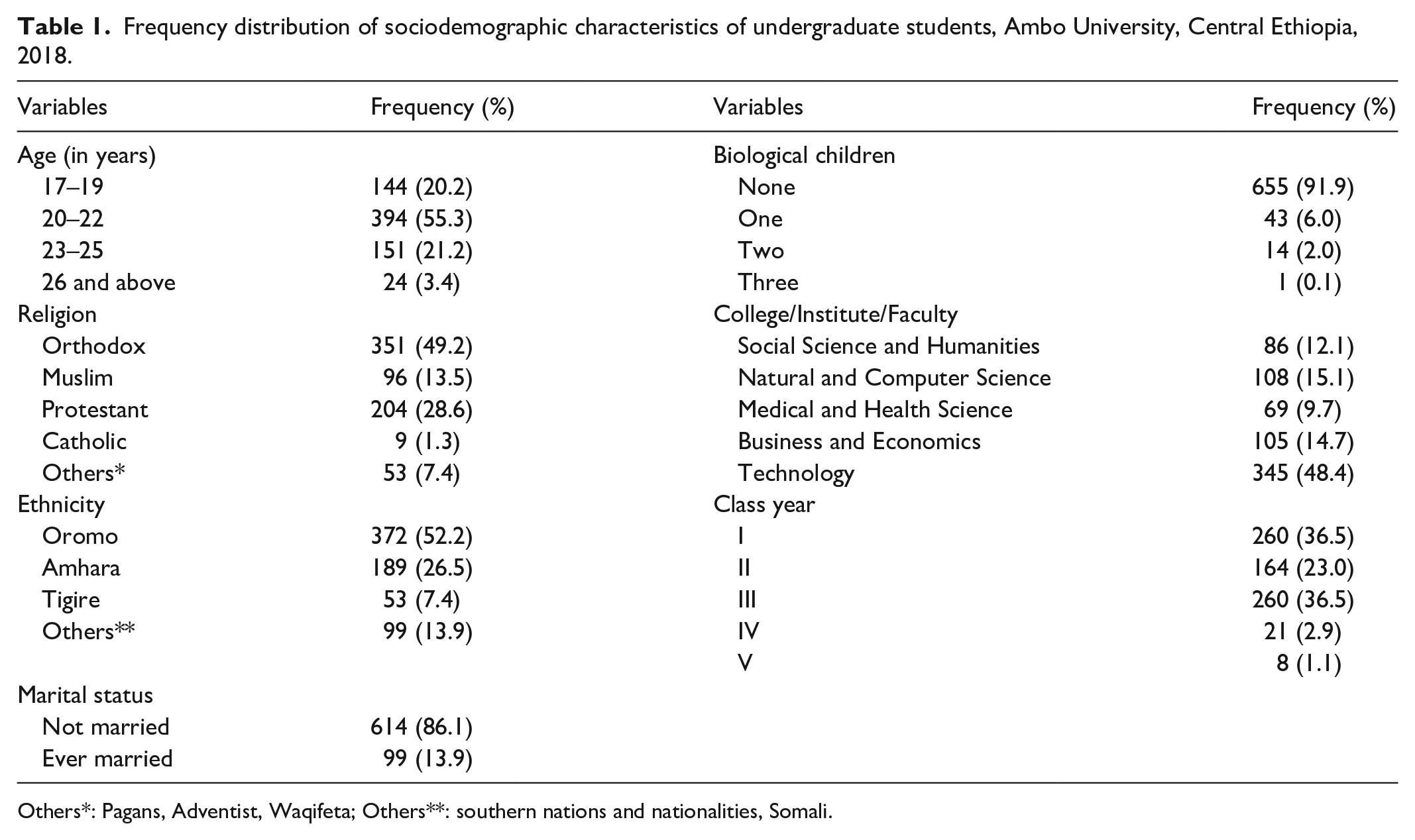
Others*: Pagans, Adventist, Waqifeta; Others**: southern nations and nationalities, Somali.
Frequency distribution of lifestyle-related characteristics of undergraduate students, Ambo University, Central Ethiopia, 2018.

Variables associated with menstrual-related discomfort among undergraduate students, Ambo University, Central Ethiopia, 2018.

MRD: menstrual-related discomfort; COR: Crude Odds Ratio; CI: confidence interval.
Significantly associated with MRD at 95% CI and 1 (reference).
The variables: age (17–19 years), Tigire ethnicity, single marital status, smokers, and those who drank 1–3 cups of coffee were significantly associated with menstrual-associated discomfort. The variables were also presented in Tables 4 and 5, with bivariate and multivariate logistic regression models. As indicated in Table 4, gynecological and obstetric background of the participants in bivariate logistic regression analysis was associated with menstrual associated discomfort among undergraduate students. Table 5, indicating the final determinant factors in multivariate logistic regression analysis, is significantly associated with the participants’ menstrual-associated discomfort.
Bivariate logistic regression analysis indicating gynecological and obstetric variables associated with menstrual-related discomfort among undergraduate students, Ambo University, Central Ethiopia, 2018.

MRD: menstrual associated discomfort; COR: crude odds ratio; CI: confidence interval.
Significant at 95% level of significance, 1 = reference.
Determinant factors in multivariate logistic regression analysis associated with menstrual-related discomfort among undergraduate students, Ambo University, Central Ethiopia, 2018.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Hosmer and Lemeshow’s goodness-of-fit test produces chi-square of 5.571 with p-value of 0.695 and 8-degrees-of-freedom; hence, the model was good for the data.
Significant at 95% level of significance, 1 = reference.
Discussion
In this study, the overall prevalence of MRD was found to be 68.6%. This was in line with study conducted among high school students in Addis Ababa, Ethiopia (65.6%) and in Nigeria (66.2%).10,11 The prevalence of MRD in this study was comparable in Nigeria among female undergraduate students, which was 74.2%. However, this finding was a little bite higher than in Brazil, conducted among female undergraduate students, which was 53.1%.6,14 The possible reason for this difference may be due to age difference—in our study and in Brazil.
In this study, the overall prevalence of dysmenorrhea was 81.2%. This was similar with study conducted among university students in Bahir Dar University, Ethiopia (85.1%), in Hong Kong (80%), and Thailand (84%). However, this finding was inconsistent with other studies among secondary school students in Northern Ethiopia (72%) and among university students in Nigeria (64%) and among Mexican high school students 48%.12–17 Other studies showed higher prevalence of dysmenorrhea; 88% in Turkey, 93% in Taiwan university students, and 93% in Australian high school students.18–20
By taking age as one sociodemographic variable in our study, MRD was higher in age group of 17–19 years, and there was a significant association between younger students and MRD. Adolescent students whose age was between 17 and 19 years were 3.9 times more likely to be experienced MRD than those students whose age was 26 years and above (AOR = 3.9 (95% CI: 1.28, 11.78)). Similar findings were observed that the older age was associated with less severe symptoms and older women experienced less pain in their menstrual cycles. Younger women were more likely to complain of breast pain, discomfort, swelling, and tenderness when compared to older women.7,22
In our study, based on ethnicity, students from Tigire ethnic group were 2.4 times more likely to be encountered MRD than other ethnic group students (AOR = 2.4 (95% CI: 1.02, 5.75)).
This may be due to geographical barrier between the Tigire region and Oromia region that may cause psychological stress which may have its own influence on the students’ menstrual associated discomfort.
Smoking, as one of the lifestyle-associated factors in this study, had a significant association between smoking and MRD; smokers were more likely to be experienced more MRD than nonsmokers. Students who currently smoking cigarettes were 2.2 times more likely to be encountered with MRD than who did not/never smoked (AOR = 2.2 (95% CI: 1.12, 4.29)). This study was in line with study conducted in Turkey in which smokers had a 1.6-fold higher risk of dysmenorrhea than non-smokers. 23 Another study reported that the risk of dysmenorrhea increased with the duration of smoking and the number of cigarettes smoked every day. 24 In contrast, another study reported that smokers had significantly less dysmenorrhea than non-smokers. 25 That is, the relationship between smoking and dysmenorrhea is heterogeneous in nature.26,27
In our study, regarding drinking caffeine, students who drink 1–3 cups of caffeine per day were 1.8 times more likely to be experienced MRD than students who were not or drink less than one cup of caffeine (AOR = 1.8 (95% CI: 1.17, 2.74)). A similar finding was found in Turkey which showed that coffee consumption was an important risk factor for dysmenorrhea. Other researchers support these findings that there was a positive association between caffeine consumption and intensity of menstrual pain. Caffeine aggravates and increases symptoms of premenstrual syndrome.6,7,28 The mechanisms of action of caffeine include inhibition of hydrolysis of cyclic 3′,5′-adenosine monophosphate and 3′,5′-guanosine monophosphate 29 and antagonism of adenosine making it plausible that caffeine might alter hormonal profiles and thereby affect menstrual function. 30
In this study, as a gynecological and obstetric factor, the amount of bleeding per cycle is significantly associated with MRD. Students who had moderate menstrual flow/cycle were 1.6 times more likely to be encountered with MRD than who had experienced little amount of menstrual flow per cycle (AOR = 1.6 (95% CI: 1.05, 2.41)).
Participants who had heavy menstrual flow per cycle were 2.4 times more likely to be encountered with menstrual associated discomfort than who had experienced little amount of menstrual flow per cycle (AOR = 2.4 (95% CI: 1.28,4.62)). Similar finding was observed in Nigeria. 14
Limitations of the study
One of the limitations of this study was the nature of the study design; we have used cross-sectional study design using questionnaires. Therefore, it would be better if conducted using prospective cohort study design. In addition, the study did not differentiate the nature of the menstrual pain from any confounder pain among the participants. Furthermore, this study did not incorporate factors, such as types of diet that may be used by the students and lifestyle variables including the types of sport activities that may associate with menstrual associated discomfort. In addition, the levels of menstrual pain are not investigated in our study, hence it needs further study.
Conclusion
This study concludes that majority of the participants experienced with menstrual-associated discomfort. As the tendency of smoking cigarettes, drinking caffeine, and amount of flow is increased, menstrual associated discomfort is increased. In addition, factors like being younger, and for unmarried individuals, the tendency of menstrual-associated discomfort is increased. Therefore, specific plan of action and support is urgently needed in order to enlighten and treat menstrual associated discomfort. For example, students may miss class due to menstrual-associated discomfort so that makeup class must be arranged to compensate the class. In addition, awareness creations must be provided to the female students, to avoid smoking and alcohol consumption to reduce menstrual associated discomfort.
Operational definitions
Alcohol consumption: Drinking of 21 g/day or greater of daily or 1–2 standard drinks per day is risky. For local drinks in Ethiopia, those who drink more than 60 mL of Areki or 500 mL of Tella or 300 mL of Teji are considered risky, or consumption of ⩾4 drinks (56 g) on a single occasion. 31
Menstrual cycle: The process of ovulation and menstruation, or it can be defined as the monthly cycle of changes in the ovaries and the lining of the uterus (endometrium), starting with the preparation of an egg for fertilization.
Menstrual-associated discomfort: discomfort results from the premenstrual syndrome or due to extended menstrual pain, which can often directly affect quality of life including interfering in students’ classroom activities, such as working or studying, and disturb any other activities.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211003361 – Supplemental material for Menstrual related discomfort and associated factors among undergraduate students in Ambo University, Central Ethiopia
Supplemental material, sj-pdf-1-smo-10.1177_20503121211003361 for Menstrual related discomfort and associated factors among undergraduate students in Ambo University, Central Ethiopia by Mesenbet Terefe Yirsaw and Mengistu Zelalem Wale in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Ambo University, Debre Markos University, and all the study participants.
Author contributions
M.T.Y. and M.Z.W. wrote the proposal, participated in data collection. M.Z.W. and M.T.Y. analyzed the data and drafted the manuscript. All the authors approved the study and preparing the manuscript by analyzing the data. All the authors revised the subsequent drafts of the manuscript, read, and approved the final manuscript.
Availability of data and materials
We have sent all the available data and we do not want to share the raw data as we are doing associated study.
Ethical approval and consent to participate
The study was approved by Research and Ethical Review Committee of School of Medicine, Debre Markos University. After information was provided about the objectives and importance of the study, verbal informed consent was obtained from the participants. There were no potential risks that may cause any harm in any form on the study subjects. All information, which was communicated with the study participants was kept and will be keep private and confidential. Coding and aggregate reporting were used to eliminate respondents’ identification and ensure anonymity and the data will not transfer to the third body and was used only for the research purpose to ensure confidentiality.
Informed consent
After information was provided about the objectives and importance of the study for the study participants, only verbal informed consent was obtained; this was because the study did not involve any clinical trial or no blood sample collection and/or/ no other experimental activities which may harm the study participants in any form. Rather, the study was conducted only using questionnaires (interview method). This procedure of obtaining verbal consent was approved by the Research and Ethics Review Committee of School of Medicine, Debre Markos University. Written informed consent for minor subjects to conduct the study was obtained from the legally authorized representative of the participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.