
Abstract
Aim and Objective:
This study was intended to compare and determine the potency of strontium-doped nano-hydroxyapatite paste against a topical cream containing casein phosphopeptide-amorphous calcium phosphate and a regular dentifrice for remineralization of white spot lesions of enamel following orthodontic debonding.
Methods:
Ninety individuals with white spot lesions on their enamel who visited the orthodontic department for de-bonding were selected for the research. Patients were randomly assigned to three distinct groups with each group consisting of 30 patients. Group 1 served as the control and received regular dentifrice, Group 2 received strontium-doped nano-hydroxyapatite paste, and Group 3 received casein phosphopeptide-amorphous calcium phosphate topical cream. Patients were instructed to locally apply a specified amount of the prescribed preparation twice daily for six weeks. The data were analysed using the statistical programme SPSS 22.0 (SPSS Inc., Chicago, IL, USA), and the level of significance had been set at p < 0.05.
Results:
Group 1 did not show any change in the enamel following the application of toothpaste. Both Group 2 and 3 demonstrated higher post-treatment scores, indicating effective remineralization potential (p < 0.001). However, Group 2 (strontium-doped nano-hydroxyapatite paste) displayed significantly greater remineralization capacity when compared to group 3 (casein phosphopeptide-amorphous calcium phosphate topical cream).
Conclusion:
Compared to conventional dentifrice and casein phosphopeptide-amorphous calcium phosphate paste, strontium-doped nano-hydroxyapatite preparation demonstrated greater enamel remineralization of the white spot lesions and favourable surface alterations in the enamel surface. strontium-doped nano-hydroxyapatite can be utilised safely and efficiently to treat early caries and remineralise white spot lesions on the enamel.
Keywords
Introduction
An imminent risk of orthodontic therapy is the demineralisation of enamel which occurs as a result of the deposition of plaque around the brackets for extended periods that subsequently creates white spot lesions (WSLs). 1 The earliest indications of caries are WSLs, which if left untreated proceed to cavitated lesions. Effective therapy can prevent and reverse these lesions. 2 This is plausible if cariogenic stressors in the particular microenvironment are adequately managed or if corrective drugs are employed to encourage tissue healing. Given the resemblance of hydroxyapatite (Ca10(PO4)6(OH)2) to the mineral compositions found in teeth, it is one of the most biocompatible and bioactive materials that is employed to remineralise the enamel.
Recently, remineralisation of enamel defects has been accomplished using nano-hydroxyapatite (nHAp). Together with saliva’s inherent ability to heal wounds, nanosized particles of hydroxyapatite (nHAp) can enter the pores of enamel, increasing the rate at which Ca2+ ions are released and thus promoting mineralisation in the teeth. 3 Many studies have been conducted replacing calcium (Ca2+) with strontium (Sr2+) in various ratios to overcome the limitations of nHAp.4 –8 Sr2+ is a trace element in the body and is readily absorbed and integrated by tissues. Strontium-doped nano-hydroxyapatite (SrnHAp) has been demonstrated to have potential for encouraging enamel repair and remineralisation. The cytotoxicity and toxicology assessment of the patented SrnHAp paste has been already established. 9
The application of casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) is one of the numerous methods that have been suggested for boosting remineralisation and lowering the incidence of WSLs and dental caries. 10 CPP-ACP (ACP) contains milk protein casein nano complexes with amorphous calcium phosphate that can promote the remineralisation of carious lesions by inhibiting the colonisation of cariogenic microorganisms on tooth surfaces.11,12
This study aimed to compare the remineralisation potential of SrnHAp, topical cream containing CPP-ACP, and regular dentifrice in the management of WSLs in enamel following debonding in orthodontic patients using visual assessment.
Materials and methods
Study population
This randomised controlled in vivo clinical trial registered with Clinical Trials Registry - India (CTRI) was conducted on patients who visited the Department of Orthodontics and Dentofacial orthopaedics in 2022, for debonding and having WSLs. Ninety individuals who completed orthodontic treatment with WSLs were selected in accordance with the inclusion and exclusion criteria.
Inclusion and exclusion criteria
Patients were included upon meeting the following inclusion criteria:
Age range between 15 and 25 years.
Patients with at least one WSL (with score from 0 to 2) on their upper anterior teeth who had undergone debonding after concluding orthodontic treatment were included.
WSLs that were not there before orthodontic treatment are now evident on the labial surfaces of one or more of the maxillary anterior teeth.
Patients who had not received any fluoride treatment in the past 3 months.
The teeth had no caries or other structural abnormalities.
The following were the exclusion standards:
Reluctance to be randomised into one of the three treatment groups.
Existence of an aberrant oral, physiological, or psychological condition.
Maxillary anterior teeth with any structural abnormalities, such as dentin decay, hypoplasia of the enamel, or both.
The existence of periodontal pockets around the anterior maxillary teeth.
Source of data
The sample size of 90 participants was sufficient to guarantee 90% power of the study and sample size estimated was based on other orthodontic clinical trials. 13 Ninety patients aged between 15 and 25 with WSLs on enamel were selected in accordance with the inclusion and exclusion standards. Prior to the start of the study, patients were well informed about the intent and layout of the investigation. As the study involved both minor and major subjects, written consent for participation was also acquired from the study subjects or their legally authorised representative (in case of minor).
Method of data collection
A comprehensive clinical assessment was conducted on all patients after debonding by a clinician. With the use of a plain mouth mirror and a No. 23 explorer, the teeth were visually examined for WSLs under standard examination light after air drying. Ninety patients with presence of WSLs on maxillary teeth were divided into three groups of thirty at random and received different treatment regimens. Participants were randomly assigned into Group 1, Group 2 and Group 3 with a 1:1:1 allocation as per computer-generated randomisation codes using permuted blocks of random sizes. The information about the assigned groups was recorded on cards inside consecutively numbered, sealed envelopes to prevent bias. 14 Ekstrand et al. 15 criteria (Table 1) was employed to decide the initial scoring values of the enamel at baseline and at 6 weeks. The systems developed by Ekstrand et al. 15 are based on how caries present biologically and how it manifests during a clinical evaluation. The evaluation of non-cavitated lesions using indicators like the location and colour of the lesion, tactile evaluation, cavitation, and the lustre are credible predictors and when used collectively will boost the precision of activity assessment and exhibits excellent reproducibility.
Visual inspection criteria (Ekstrand et al. 15 ).

For inter-examiner and intra-examiner bias, calibration test was done before the start of study for satisfactory conformity. The visual assessment was conducted by two examiners in accordance with the scoring criteria established by Ekstrand et al. 15 Only lesions scoring from 0 to 2 were included in the study. The examiners evaluating the scores, as well as the patients were blinded to avoid bias. The examiners visually assessed for WSLs in four areas (i.e., gingival, incisal, mesial, and distal) on the labial surfaces of maxillary anterior teeth at baseline and post-treatment in all patients.
Group 1 served as the control and received regular Colgate tooth paste, Group 2 received SrnHAp paste, and Group 3 received Casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) preparation.
Preparation of SrnHAp paste
A fine powder made using the 25 mol% SrnHAp co-precipitation technique was used to formulate the paste. To get a paste-like consistency, the dry ingredients were all thoroughly crushed by mortar and pestle before being mixed with glycerin and deionized water. The freshly prepared paste weighed 100 g and contained 50 g of 25 mol% SrnHAp, 30 g of glycerine and sorbitol working as humectants, 2 g of sodium lauryl sulphate serving as detergent, 3 g sodium alginate as binder, and 15 ml of deionized water. 9 The paste was then placed in anopaque tube and utilised in the experiment.
All the three preparations were transferred into opaque tubes and labelled as A, B and C. Tubes were distributed among patients as per their respective groups. Patients were instructed to use a standardised amount of the provided paste twice daily for six consecutive weeks after using dentifrices and soft-textured toothbrushes for daily oral care. 16 Since the preparations had different consistencies, to guarantee that the remineralizing agents stay on the tooth surface and to avoid relapse following orthodontic therapy, subjects were advised to wear Essix clear retainers. 17 Follow-up appointments were set at the completion of 6-week period. The trial was stopped after receiving the post-treatment scores of all the samples from all three groups. Each group were evaluated separately for pre-treatment and post-treatment scores as primary outcomes. Flowchart of the participant flow and experimental procedure is shown in Figures 1 and 2.

Flowchart of participant flow.

The flowchart of the experimental procedure.
Statistical analysis
The statistical programme SPSS 22.0 (Statistical Package for Social Sciences Inc., Chicago, IL, USA) was employed for analysing the data. To evaluate the standard deviation and mean of the various groups, a descriptive statistical analysis was carried out. The visual analogue score was compared across groups using the Kruskal–Wallis ANOVA test and intra-group comparisons using the Mann–Whitney test. A p-value of 0.05 cutoff was used to determine significance.
Ethical considerations
Prior to including any human participants in the study, their informed written consent was obtained from them or their legal representatives. Anonymity and confidentiality of subjects were maintained throughout the investigation. Ethical clearance for the study was attained from NIMS institutional ethical committee (NIMS/IEC/2022/04/02).
Results
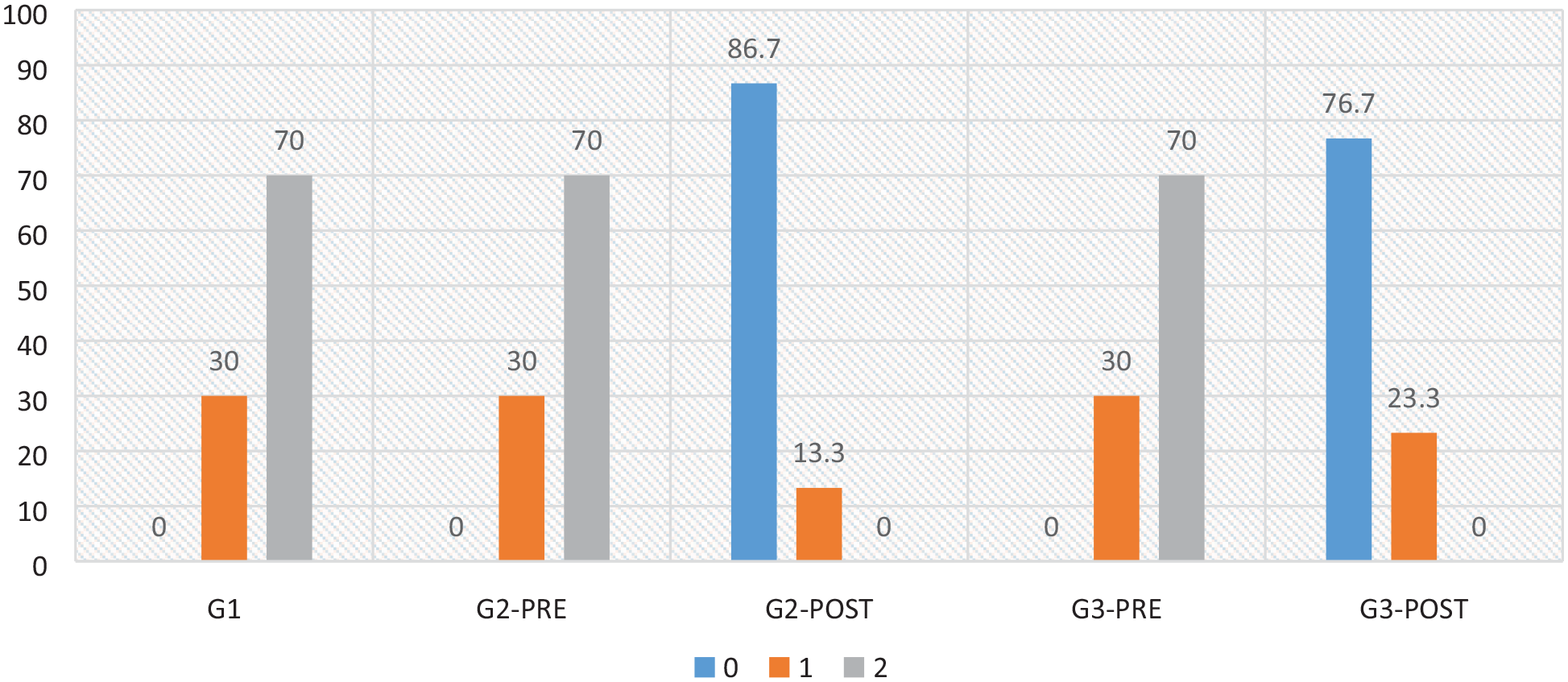
Of the 90 patients that were included in the study, 46 (51.2%) were men and 44 (48.8%) were women. Table 2 revealed that there were no significant variations in the presence of WSLs between males and females. With a p-value greater than 0.05, there was no statistically significant difference in the distribution of WSLs according to gender in any group. The pre- and post-treatment scoring of all three groups were evaluated based on the Ekstrand et al. 15 Criteria and is shown in Table 3. The statistical analysis was based on the number of patients with WSLs of scores 1 and 2. For Group 1 (toothpaste without any remineralising agent), the pre-treatment score was 2 for 21 subjects and 1 for 9 subjects. There was no change in the pre- and post-treatment scores of Group 1 (30% and 70%). The pre-treatment score of both group 2 (SrnHAp paste) and group 3 (CPP-ACP) was similar to group 1. However, the post-treatment score of Group 2 (SrnHAp paste) was 0 for 26 subjects and 1 for 4 subjects, showing greatest remineralisation potential (86.7% and 13.3%) when compared to group 3 with 0 for 23 subjects and 1 for 7 subjects (76.7% and 23.3%respectively) (Figure 3).
Demographic data of the studied groups at baseline (pre-treatment).

p-value ⩽ 0.05 statistically significant.
N = number of patients.
Pre-treatment and post-treatment scores of all three groups.

The number of patients with presence of WLS on any maxillary teeth is considered.
Comparison of the change in pre-treatment and post- treatment scores among the three groups.
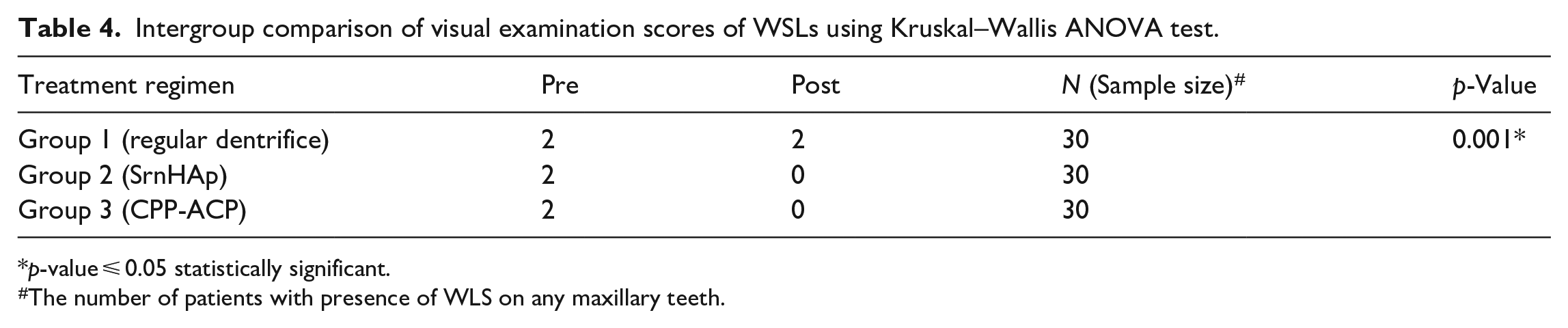
The intergroup comparison of pre- and post-treatment scores and the average median score calculated for the three groups are shown in Table 4. There was no change in the enamel after using toothpaste without a remineralising ingredient since Group 1’s pre- and post-treatment median scores were both 2, indicating that there was no difference between the two. In contrast, the pre-median treatment score in groups 2 and 3 was 2 and the post-median treatment score was 0, suggesting the remineralising efficiency of the preparations employed (Figure 4). The intergroup comparison of pre- and post-treatment scores of all three groups was made using the Kruskal–Wallis ANOVA test. The outcomes were of statistical importance (p-value 0.001) since the p-value ⩽ 0.05was considered statistically significant (Table 4).
Intergroup comparison of visual examination scores of WSLs using Kruskal–Wallis ANOVA test.
p-value ⩽ 0.05 statistically significant.
The number of patients with presence of WLS on any maxillary teeth.

Graphical representation of post-treatment scores of three groups.
According to the Ekstrand et al. 15 criterion, scores of 0, 1, and 2 were assigned to each category. The Mann–Whitney test was used for the intergroup comparison and when groups 1 and 2 were compared, Group 2 had the highest post-treatment score, which was deemed significant (p-value of 0.001) (Table 5). This indicates the superiority of SrnHAp paste over conventional toothpaste in terms of remineralization. The remineralising potential of groups 2 and 3 were compared. (Table 6). Both SrnHAp and CPP-ACP groups showed greater scores for remineralisation potential compared to the control, but the difference among the two groups were statistically non-significant (p-value 0.321) since only a p-value ⩽ 0.05 was considered to be statistically significant (Figure 5).
Mann–Whitney test for intergroup comparison of visual examination score for groups 1 and 2.

p-value ⩽ 0.05 statistically significant.
Mann–Whitney test for intergroup comparison of visual examination score for groups 2 and 3.

p-value ⩽ 0.05 statistically significant.
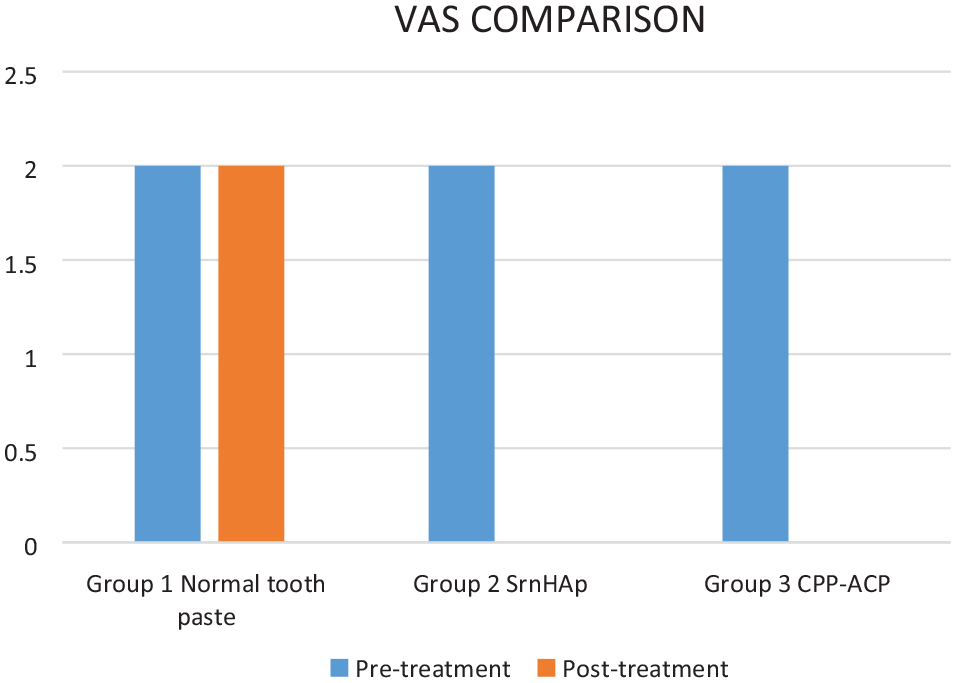
Intergroup comparison of visual analogue score.
Discussion
Preventing demineralisation and promoting remineralisation of the lesions through the use of different remineralising agents is the main treatment strategy for WSLs. The remineralisation capacity of SrnHAp preparation were evaluated in this study in comparison to a commercially available regular toothpaste and a topical CPP-ACP cream. The research revealed that SrnHAp paste and CPP-ACP preparations both showed improved remineralisation capacity in comparison to the control toothpaste. Products with casein phosphopeptides-amorphous calcium phosphate (CPP-ACP) may be able to impede enamel demineralisation. CPP-ACP’s effectiveness depends on the integration of nano complexes on the tooth surfaces and into dental plaque, thus serving as a storehouse of calcium and phosphate. 18 According to research by C. Reynolds, CPP-ACP localises ACP in dental plaque, which buffers the free calcium and phosphate ion activities and aids in maintaining the enamel in super saturation, thereby avoiding demineralisation and promoting remineralisation. 19 This would explain the improved post-treatment scores of the CPP-ACP group. Several clinical investigations have also proven CPP-ACP to be effective in preventing and regressing WSLs during orthodontic therapy.20 –22
In contrast, the EDAX analysis performed by Krishnan et al. in his study found that ACP-CPP specimens had greater phosphate levels than calcium, which rendered it insufficient for healing damaged enamel since calcium supplementation appears to be low. 23 However, with regard to aesthetic concerns, the mode of action of CPP-ACP offers deeper ion penetration, leading to the remineralisation of the whole lesion rather than just the surface layer. This enhances the aesthetic appearance of remineralised lesions. 24
The difference between SrnHAp doped group and ACP-CPP treated group is statistically non-significant. However, results of this investigation show that Strontium-doped nHAp paste appears to have a better potential for remineralisation than ACP-CPP cream. SEM EDAX analysis of the surface topography and the calcium/phosphorous ratio of tooth specimens treated with Casein Phosphopeptide, CPP-ACP and SrnHAP for 28 consecutive days has revealed that strontium-doped nano-hydroxyapatite showed better remineralisation than CPP-ACP and can be considered for enamel repair in incipient carious lesions. 25 Similar outcomes were seen in research by Krishnan et al., 23 which determined that SrnHAp in solution was superior to CPP-ACP cream and nHAp toothpaste for recuperation of demineralized enamel surface. According to the research, adding strontium enhanced the dissolving ability and retention of material on to the tooth surface, making it more effective than CPP-ACP in remineralising and restoring enamel. 23 Moreover, the increased crystallinity and smaller-sized particles of 25% Sr-nHAp facilitate better diffusion through enamel, making it an excellent material for repairing enamel lesions and white spots.
WSLs usually develop in conjunction with orthodontic appliances that obstruct routine oral hygiene procedures and cause plaque to build up over time. 26 This increases the likelihood of caries formation. However, we observed that the SrnHAp Group’s post-treatment scores revealed no evidence of any new lesions or progression of the ones that already existed into caries. Instead, outcomes of this study demonstrated total eradication of the WSLs. This could be attributed to SrnHAp antibacterial properties. In a research on the antibacterial properties of a remineralising paste of Sr-nHAp, Rhea Mathew et al. discovered that a 20% formulation of Sr-nHAp had better antimicrobial properties against Streptococcus mutans. In addition to improving the mechanical qualities of enamel by remineralising its deeper layers, biomimetic formulations with antibacterial activity will also help to lower the occurrence of secondary caries. 27
It was statistically significant that the SrnHAp paste had a better capability for remineralisation than conventional toothpaste. Again, this may be credited to the smaller particle size, which aids in penetrating pores, and the smaller crystal size, which enhances solubility. 9 An evaluation of the remineralising effects of conventional fluoridated toothpaste with nanosized sodium trimetaphosphate was carried out by Danelon et al. 28 It was determined that as compared to ordinary toothpaste alone, the inclusion of tailored remineralising substances produced a substantially greater remineralising effect.
The cytotoxicity of regular toothpaste and SrnHAp paste was evaluated in a previous study of 2021. 9 The nontoxic nature of SrnHAp paste was established by an in-vitro study comparing ordinary toothpaste to SrnHAp paste on 60 extracted teeth. The percentage viability of cells was higher with SrnHAp paste than with conventional toothpaste, showing its nontoxic nature. In the research by Tabatabaei et al., the evaluation cytotoxicity of various doses of standard dental paste against mouthwashes revealed that a significant portion of cells were eliminated, with toothpaste having the maximum cytotoxicity. 29 Every toothpaste contains a substantial amount of detergents, which have been demonstrated to cytotoxically affect the different cells in the oral cavity. However, the SrnHAp paste used for this investigation only has 2 g of detergent. This may have contributed to the increased bioactivity and decreased cytotoxicity, together with the addition of strontium to HA. Since synthetic hydroxyapatite most closely resembles the mineral component of tissue, it has remarkable bioactive properties including cytocompatibility. The results of Rajabnejadkeleshteri et al.’s 30 MTT experiment demonstrate that increasing the amount of strontium has a favorable impact on both cell proliferation and remineralization. His research also indicates that the incorporation of strontium into HA has favorable and stimulating effects on cell development and differentiation. Hence, it has been proven that SrnHAp paste is nontoxic and may be utilized as an enamel repair remineralising agent safely and efficiently.
The results obtained from this comparative study supports the use of SrnHAp pasteover CPP-ACP cream and regular dentifrice. SrnHAp paste can be used to prevent demineralization or treat WSLs formed following orthodontic therapy. SrnHAp can be utilised to efficiently treat early caries and repair of enamel. However, further clinical studies incorporating different Sr2+ ion concentrations and other clinical aspects of the paste must be conducted before it can be used commercially.
Limitations of the study
Within the limitations of this study SrnHAp containing remineralising paste had a remarkable remineralisation effect in the 6 weeks evaluation period but a longer observation period with a larger sample size is advised to confirm whether the greater remineralisation in early caries lesions is maintained. To confirm the results for possible therapeutic uses, further clinical studies incorporating different Sr2+ ion concentrations and other clinical aspects of the paste must be conducted.
Conclusion
Within the constraints of this investigation, it can be concluded that, in comparison to conventional dentifrice, both the CPP-ACP cream and the SrnHAp preparation caused more favorable surface alterations in enamel and showed remineralization of WSLs following orthodontic therapy. Interestingly, the findings imply that SrnHAp paste has a slightly better potential for remineralisation than CPP-ACP cream. The efficacy of using SrnHAp paste as a remineralising agent has been proven by this investigation.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231221634 – Supplemental material for Remineralization potential of strontium-doped nano-hydroxyapatite dentifrice and casein phosphopeptide-amorphous calcium phosphate cream on white spot lesions in enamel following orthodontic debonding – a randomized controlled trial
Supplemental material, sj-docx-1-smo-10.1177_20503121231221634 for Remineralization potential of strontium-doped nano-hydroxyapatite dentifrice and casein phosphopeptide-amorphous calcium phosphate cream on white spot lesions in enamel following orthodontic debonding – a randomized controlled trial by Ratheesh Rajendran, Delphine Priscilla Antony S, Mohammed Ashik P, Subin Bharath, Arun Jacob Thomas and Artak Heboyan in SAGE Open Medicine
Footnotes
Acknowledgements
None.
Author contributions
All the authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical clearance for the study was obtained from NIMS institutional ethical committee (NIMS/IEC/2022/04/02).
Informed consent
As the study involved both minor and major subjects written consent for participation was also acquired from the study subjects or their legally authorised representative (in case of minor).
Trial registration
This study was registered in the Clinical Trials Registry- India under the ID: CTRI/2022/06/043066 (Registered on: 07/06/2022 – Trial Registered Prospectively).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.