
Abstract
Objective:
Alveolar osteitis is a painful complication that often arises after tooth extraction, presenting a significant clinical challenge. It is imperative to gain a comprehensive understanding of both its occurrence and the contributing factors to enhance the quality of dental care. The aim of this study was to assess the frequency and prevalence of alveolar osteitis among patients and compare these variables based on demographic characteristics (age and sex), the number of teeth extractions, operator experience, health status, and smoking habits in the target population.
Methods:
This cross-sectional observational study was conducted from May 2019 to April 2020. It included all patients above 16 years of age, of both genders, who underwent permanent tooth extraction for various reasons. Patient demographics, smoking habits, health status, operating dental surgeon’s clinical experience, extraction technique, and the number of teeth extracted were recorded. Statistical analysis was performed using SPSS version 25. Chi-square test and regression analysis were used to assess differences between age, sex, smoking habit, dentist category, and the number of teeth extractions in relation to alveolar osteitis.
Results:
A total of 679 permanent tooth extractions were performed in 438 patients. Alveolar osteitis was observed in 107 cases (15.7%) following tooth extractions. Among these, 36 cases (33.6%) occurred in single tooth extraction cases, while 71 cases (66.4%) were present in patients with multiple extractions. Moreover, 67 cases (62.6%) of alveolar osteitis were found in cigarette smokers. In addition, 61 cases (57%) of dry sockets were reported after tooth extractions performed by dental interns, while 46 cases (43.0%) were noted in extractions performed by experienced dental surgeons and specialists.
Conclusion:
The study found a 15.7% incidence of alveolar osteitis in tooth extraction patients in the Al-Jouf region. Alveolar osteitis was more prevalent in males and the age group of 56–77 years. Multiple tooth extractions were associated with higher alveolar osteitis incidence, while operator inexperience increased post-extraction complication risks. In addition, a promising novel protocol and risk assessment scoring system have been devised which require further validation and future research.
Introduction
Alveolar osteitis (AO), also known as dry socket, is one of the frequent postoperative complications after tooth extraction. 1 Crawford (1896) named this condition “AO” which is designated as a severe inflammation of the tooth-bearing socket bone seen after 2–4 days around the site of the extracted tooth socket presented by intense discomfort, obliteration, and replacement of the preliminary blood clot in the socket with food debris.2 –4
A high incidence rate of AO has been reported, ranging between 5% and 30% when the impacted mandibular third molar is surgically extracted, and found 1%–4% in non-surgical dental extraction.5,6 The etiology of AO is still unknown, although many predisposing factors are proposed including age, sex, oral contraceptives consumption, tobacco smoking, tooth location, dental socket bone trauma due to challenging extractions, compromised dental hygiene, increased vasoconstrictive effect due to adrenaline of local anesthetics administered, operative and postoperative management, and operator skill. 7
The pathogenesis suggested is the rise in fibrinolytic activity after extraction that might lead to premature intra-alveolar blood clot disintegration.6,7 This is due to an activation of the plasminogen path that leads to fibrinolysis, initiated via direct physiologic activators following the traumatization of dental socket osteocytes or non-physiologic activator substances secreted by bacteria indirectly. 8 The exact pathophysiology linking smoking and AO is still elusive, although the suggested physical blood clot dislodgement due to the vacuum effect generated by sucking on cigarettes is the dominant theory.2,9
Despite its unknown definitive etiology, management of AO is however quite straightforward involving washing and flooding the involved empty tooth socket followed by placement of obtundent dressing while reassuring the patient. 10 Furthermore, prevention is more effective in avoiding its occurrence. 11 Several studies have reported that the preoperative and perioperative use of 0.12% chlorhexidine decreases the frequency of AO after mandibular third molar removal.4,6 –9
It is very crucial to know the predisposing factors associated with AO that could be avoided to prevent the occurrence of this painful condition. The rationale of this study lies in its potential to improve dental care outcomes and enhance the well-being of patients in the Northern Province. By elucidating the frequency and specific factors associated with AO, we can develop targeted strategies for prevention and management. Therefore, our hypothesis suggests that the frequency of AO in patients from the Northern Province of the Kingdom of Saudi Arabia is influenced by a multifaceted interplay of factors, including demographic attributes such as age and gender, in conjunction with specific etiological elements. Specifically, it is anticipated that older individuals may have a higher incidence of AO due to potential age-related differences in healing processes. In addition, certain habits and conditions, such as smoking and compromised dental hygiene, may be associated with a greater likelihood of AO in this population. Against this background, the objective of this study is to empirically assess these hypotheses. Furthermore, it aims to investigate the frequency of AO and gain a thorough insight into the elements that influence AO in the Northern Province.
Materials and methods
General information
This cross-sectional observational study was conducted from May 2019 to April 2020 at the Department of Oral and Maxillofacial Surgery, Jouf University. The study was conducted with the permission of the ethical review board of Jouf University (Institutional ethical application no: 11-04-42). All patients or parents/guardians/patients’ legally authorized representatives who signed a written informed consent were included in the study. A convenience sampling technique was used to recruit the participants. The study was planned and executed according to the STROBE guidelines for cross-sectional studies, and the checklist is attached as Supplemental Material 1.
Sample size estimation
The sample size for our study was determined with 80% power and 95% confidence level, using α as 0.05. Considering a 48 (39%) 1 of AO occurrence after single tooth extraction. Using the formula, Z = 1.96 (Z (1.96) 48 = 3.84), we calculated the required sample size (n) as {48 [(48.0) 48/(5)2]} × 3.84, which resulted in a total of n = 438 patients being enrolled in the study.
Patients selection criteria
Inclusion criteria:
Age: Patients above 16 years old.
Gender: Both males and females.
Patients presenting for permanent tooth extraction for various reasons.
Patients who provide written informed consent to participate in the study.
Patients who are willing and able to comply with study requirements that is, Compliance with Study Protocol, Availability for Follow-up, and Open Communication.
Exclusion criteria:
Deciduous teeth extractions.
Patients below 16 years of age.
Patients with a history of osteomyelitis, coagulation disorders, or any other medical conditions that may interfere with the healing process.
Patients with a known allergy or hypersensitivity to any dental materials used during the extraction procedure.
Patients with a history of radiotherapy or chemotherapy in the oral and maxillofacial region.
Pregnant patients or nursing mothers.
Patients with a history of bisphosphonate therapy or other medications known to affect bone metabolism.
Patients who are unable to provide informed consent due to language barriers or cognitive impairment.
Grouping and methods
Patients were categorized into three groups: group A, including individuals aged 16–30 years; group B, including individuals aged 31–55 years; and group C, including individuals aged 56–77 years. Patient demographics, smoking habits, health status, the clinical experience of the operating dental surgeon, extraction technique, and the number of teeth extracted were recorded. For the selection of patients presenting with postoperative pain, clinical history, and examination findings were considered. In addition, Blum’s criteria 5 were used for the confirmatory diagnosis of AO in this study. Blum’s criteria include patients experiencing pain and discomfort surrounding the empty dental extraction socket during the first postoperative week.
Statistical analysis
The data analysis was performed using the Statistical Package for Social Sciences (SPSS) version 25 (IBM, SPSS Statistics, version 25, Chicago, IL, USA). The chi-square test was applied to assess differences among categorical variables, including age, sex, habits of participants, and dentist category, with respect to AO incidence, given its suitability for categorical data comparisons. In addition, a comprehensive regression analysis was conducted to explore the relationship between AO (the dependent variable) and a diverse set of independent study variables, encompassing the average estimation of the extent of extraction, extraction type, and systemic health status, the operator performing the extraction, participants’ habits, gender, and age. This multifaceted approach aimed to identify and quantify specific risk factors associated with AO while accounting for potential interactions among variables. To maintain statistical accuracy, the level of statistical significance was set at p ⩽ 0.05.
Results
From the cohort of 540 patients, 438 were included in the study after meeting the eligibility criteria and providing consent, as shown in Figure 1. Among them, 297 (67.8%) were males, and 141 (32.2%) were females. The age of the patients ranged from 16 to 77 years, with 65 (14.84%) in the age range of 16–30 years, 102 (23.97%) in the range of 31–55 years, and 271 (61.87%) in the range of 56–77 years. A total of 679 dental extractions were performed on 438 patients, and dry sockets developed in 107 (15.7%) participants within the first postoperative week.

Distribution and characteristics of the participants recruited in the study.
Out of the total, 81 (75.7%) AO cases were reported in males and 26 (24.2%) in females. 28 (26.25%) AO cases belonged to group A, 39 (36.43%) to group B, and 40 (37.48%) to group C. Moreover, age-wise comparison between the three groups showed a high occurrence of multiple surgical extractions in healthy patients belonging to group C.
In the study, 36 (33%) dry sockets occurred following a single tooth extraction, while 71 (66.3%) were presented after multiple teeth extractions. In addition, 54 (50.4%) dry sockets were found in surgical tooth extraction cases, and 53 (49.5%) occurred in non-surgical extraction sites. Moreover, 58 (54.2%) dry socket cases were observed in healthy patients who were not medically compromised, while 49 (45.7%) cases were noted among patients with medical conditions such as hypertension, diabetes, autoimmune disorders, blood dyscrasias, and those on chronic drug therapy.
In our study, 61 (57%) cases of dry sockets were found after tooth extractions performed by dental interns, while 46 (43.0%) cases were found in extractions performed by experienced dental surgeons and specialists. By contrast, 67 (62.6%) cases of AO were found in cigarette smokers, while 40 (37.4%) cases were reported in non-smoker patients.
There was no significant difference (chi-square; p = 0.064) between alveolar osteitis and the health status of participants, indicating that AO was prevalent in both healthy individuals and patients with comorbid illness or drug therapy. Whereas a significant difference was found between AO and gender (Chi-square; p = 0.036), AO was more prevalent in males 67 (62.6%) as compared to female 26 (24.2%) patients. In addition, a significant difference (Chi-square; p = 0.042) was also found between AO and different ages. AO has been noticed more in the population with advancing age, comprising 58 individuals (54.2%).
A significant difference (chi-square; p = 0.028) was also seen between the extent of extraction and AO, it was more prevalent in cases with multiple extractions 71 (66.3%). However, no significant difference (p = 0.160) was found between the type of extraction and AO, indicating that AO was equally prevalent in patients with surgical and non-surgical tooth extraction. Furthermore, a significant relationship between smoker and non-smoker patients (p = 0.009) was noted meaning that AO was found more commonly in cigarette smokers. Lastly, a significant difference (chi-square; p = 0.039) was evident between alveolar osteitis and the operator, that is AO was found more in teeth extraction cases performed by dental interns 61 (57%) as compared to a specialist dentist, as shown in Table 1.
Relationship of AO with demographics and etiological denominators.
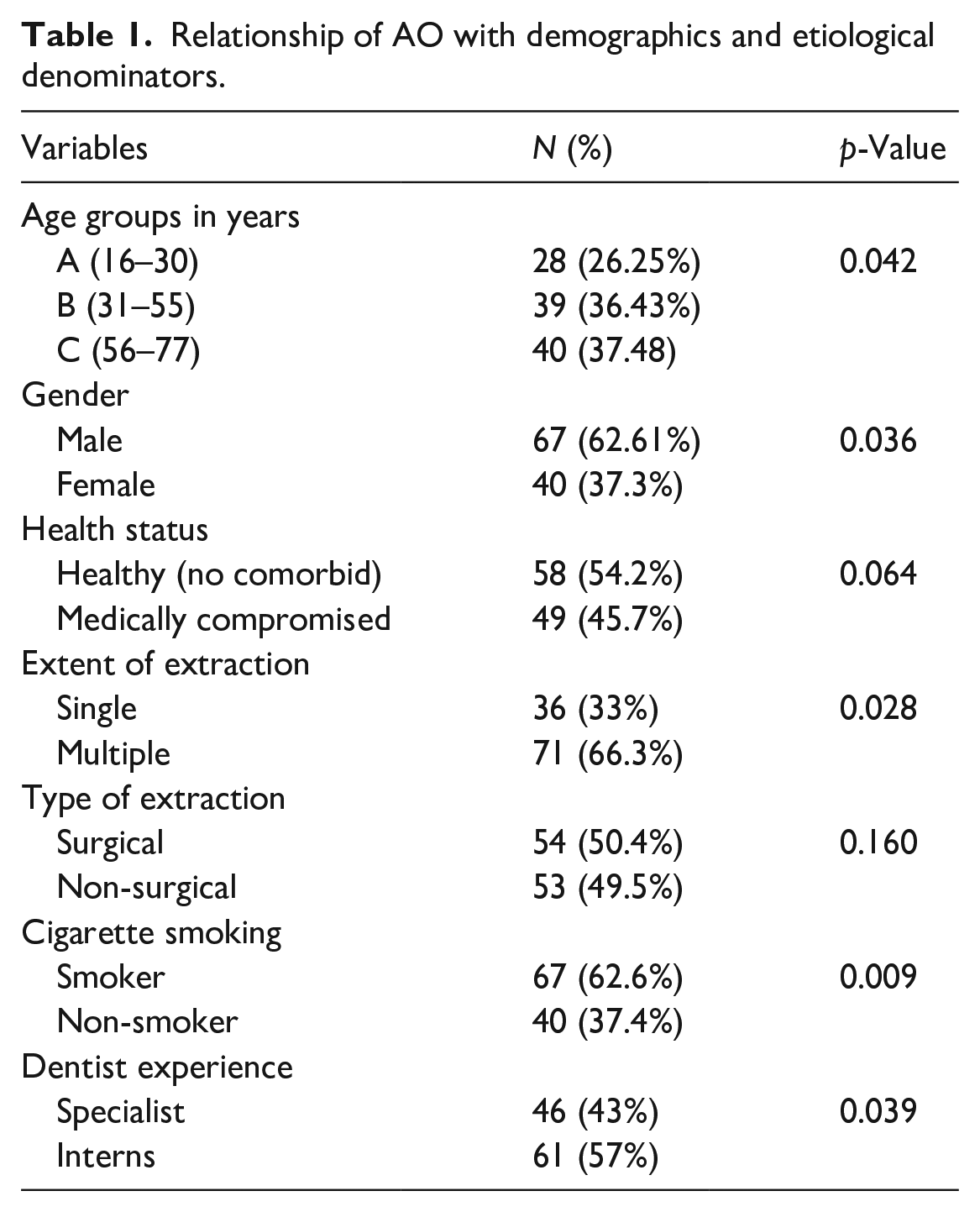
Table 2 describes a regression analysis of AO, with independent variables (average estimation of the extent of extraction, type, systematic health, extraction performed by various operators, habits, gender, and age) of the participants. The outcome of the study showed that a weak and negative correlation between AO and independent variables existed. The regression model analysis for AO to independent variables showed a constant for R-squared (R2) = 0.155 and adjusted R-squared (AR2) was 0.102; however, under the influence of independent variables, only type of extraction (p = 0.005) and age (p = 0.045) showed a significant relationship with AO. The AO to extent of extraction beta (B) value was statistically significant (B = −0.044, p = 0.005) which indicates that extent of extraction had a −0.044 relationship with AO. Whereas on average the effect of the extent of extraction on AO was B0 = −0.028 in this study. However, the age to AO beta (B) value was also statistically significant (B = 0.179, p = 0.045) which indicates that with an increase in age, the AO was increased by 0.179 or vice versa. Whereas on average the effect of age on AO was B0 = 0.068 in this study.
The regression analysis of the extent of extraction, type, systematic health, extraction performed by various operators, habits, gender, and age with AO (n = 107).
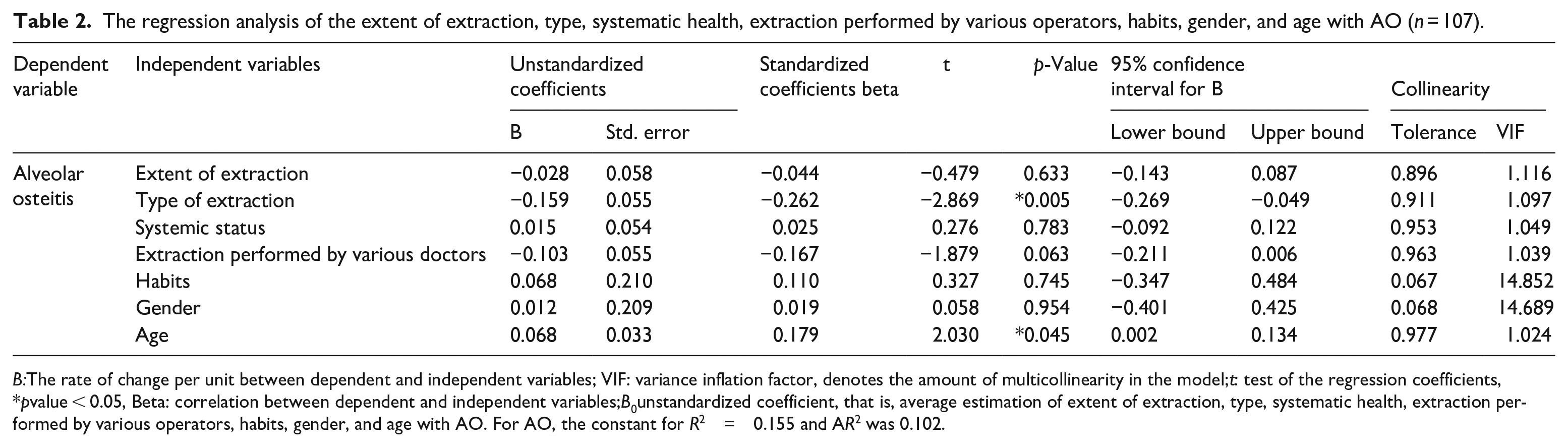
B:The rate of change per unit between dependent and independent variables; VIF: variance inflation factor, denotes the amount of multicollinearity in the model;t: test of the regression coefficients, *pvalue < 0.05, Beta: correlation between dependent and independent variables;B0unstandardized coefficient, that is, average estimation of extent of extraction, type, systematic health, extraction performed by various operators, habits, gender, and age with AO. For AO, the constant for R2 = 0.155 and AR2 was 0.102.
Discussion
In the realm of oral health research, AO has been a subject of great interest due to its variable incidence worldwide. The main cause of the study design was to investigate the frequency and etiological denominators of AO specifically in the Northern Province of the Kingdom of Saudi Arabia. The aim of the investigation was to fill the knowledge gap in the region and gain insights into the prevalence and potential risk factors associated with AO. The wide variability in the documented frequency of AO worldwide, ranging from 1% to 30%, prompted the need for a region-specific study to better understand the prevalence of this condition in the study area.1 –6 In the current study, we observed an AO incidence of 15.7%, which is notably higher compared to earlier studies conducted in various countries such as Australia, India, Palestine, Nigeria, Sri Lanka, Nepal, and other developing countries. The findings from our study highlight the significance of conducting research at a local level to capture region-specific variations in the prevalence of AO and its potential etiological factors.1 –4,11,12 By focusing on the Northern Province of the Kingdom of Saudi Arabia, we aimed to provide valuable data that can inform dental practitioners and policymakers in the region about the prevalence and risk factors of AO, ultimately leading to improved preventive measures and patient care.
In our study, AO was observed more frequently in males compared to females, which contrasts with previously reported studies in India, and Pakistan.11,13 Chandran et al. 11 reported a higher female predilection (7.86%) for dry sockets compared to males (6.18%). Similarly, Qadus et al. 13 found that females had a 2.37 times higher risk of dry sockets compared to males in their study. This difference in findings may be attributed to the fact that smoking can exacerbate socket healing, and there are more smokers among the male gender compared to their female counterparts in the studied population, also the incidence of dry socket is reported more in patients with dry socket in the past.14,15 Moreover, in Asia, oral contraceptives are more frequently used by females for population control in countries like Iran whereas in Saudi Arabia, population control is not a major issue.16,17 These factors could contribute to the observed gender-based differences in the incidence of AO in our study compared to other regions.
Parthasarathi et al. 2 reported a higher incidence of AO among patients undergoing individual tooth extraction (4.9%) compared to multiple extraction cases (1.0%). Similarly, Chandran et al. 11 explained that the low incidence of AO for multiple tooth extraction is due to the ease and uncomplicated nature of such extractions, which are usually indicated for teeth with compromised periodontal health. However, the findings of our present study contradict the previously conducted research, as we observed a higher incidence of AO in multiple tooth extraction cases compared to single extractions. This discrepancy can be better understood by considering that although multiple extractions are often indicated for periodontally compromised teeth, teeth extracted due to periodontal disease have a 7.5 times higher chance of developing dry socket, as confirmed by Parthasarathi et al. 2 in their multivariate analysis. These contrasting results emphasize the complexity of the factors influencing AO occurrence and the importance of considering various clinical scenarios when interpreting the risk factors for this condition.
In this study, AO occurred in 54 cases (50.5%) of surgically extracted teeth, while 53 cases (49.5%) were associated with non-surgical extraction cases. This finding aligns with the study conducted by Parthasarathi et al., 2 who also reported a similar slight difference in AO incidences between the two situations. The occurrence of AO in surgically extracted teeth can be attributed to the substantial forces transferred to the jawbone around tooth roots during hard and complicated extractions. In addition, excessive intra-socket instrumentation and manipulation may lead to the crushing of the bony wall of the tooth socket, potentially inducing osteoblast necrosis or apoptosis.18 –20 These factors may contribute to the increased risk of AO in surgically extracted teeth compared to non-surgical extraction cases.
In this study, 67 cases (62.6%) of AO were noted among patients who were smokers, while 40 cases (37.4%) occurred among non-smoker patients. The results demonstrate that tobacco cigarette smokers have a higher risk of developing AO as a complication after tooth extraction, relative to non-smokers. The higher incidence of AO in smokers can be attributed to several factors. First, the vacuum effect produced by smoking may disrupt the preliminary clot formation in the tooth extraction socket. Moreover, carbon monoxide from smoking limits the oxygen-carrying capacity of the blood, leading to local tissue hypoxia and delayed healing. In addition, nicotine causes vasoconstriction, reducing blood flow to tissues, and the toxic effects of tobacco smoke may damage tissue, interfering with the normal healing process.6,8,14 The platelet-rich plasma (PRP) has been suggested as an integral modality to prevent AO, while the antibiotic prescription is not an ideal strategy to treat or prevent AO after dental extractions.21,22
In our study, 61 cases (57.0%) of AO were observed in tooth extractions performed by dental interns, while 46 cases (43.0%) were found in extractions performed by qualified dentists or specialists. These results align with Puidokas et al.’s study, 20 which reported that the initial absence of a clot or its mechanical elimination (traumatic tooth extractions) or altered formation and the longer healing period are major causes of dry socket. However, our findings contrast with those of Parthasarathi et al., 2 who reported a greater risk of developing complications in cases operated by experienced practitioners compared to dental students. They attributed this finding to the fact that more experienced and skillful dental practitioners often handle hard and complicated extractions by default. The variability in these findings emphasizes the importance of considering the experience level of the dental practitioner when analyzing the risk factors for AO. Adequate training and experience in tooth extractions are essential to minimize the occurrence of complications. It also underscores the need for ongoing education and supervision of dental interns to enhance their skills and ensure optimal patient outcomes during tooth extraction procedures.
This study serves as a preliminary investigation conducted at our center. However, it is important to acknowledge certain limitations. The study was single center based, using convenience sampling, and lacking randomization, which may affect the generalizability and establish causality. In addition, reliance on self-reporting, missing data, limited variables, and geographical focus may affect accuracy and external validity. Subjective bias and unaccounted confounding factors could also influence the results. Lack of intervention limits the assessment of preventive measures. Convenience sampling was chosen for its ease of implementation, cost-effectiveness, and ability to efficiently gather data from participants who were readily accessible to us within the given time frame. However, it is essential to acknowledge the potential limitations of this sampling strategy. Convenience sampling may introduce selection bias, as participants were not selected through randomization, which may limit the generalizability of our findings to the broader population. Moreover, we did not consider maxillary versus mandibular extractions, this could have yielded stronger results, given the knowledge of higher association with mandibular extractions versus maxillary extractions in relation to AO. These are important aspects that we will take into account in future research to further strengthen our findings.
Based on the initial findings, we propose a “Dry Socket Prevention (DSP) Protocol” and a “Dry Socket Development Risk (DSDR) Score” for future more comprehensive investigations, as presented in Tables S1 and S2 (Supplemental Material 2). The DSP protocol was extracted from the findings of our study by identifying key risk factors and designing preventive measures based on the observed associations. In addition, the DSDR score was derived from the findings of our study, and it offers a promising approach to risk assessment and prevention of AO following tooth extraction. The DSDR score comprises preoperative, perioperative, and postoperative risk factors. A preoperative risk factor score of more than 6, a perioperative risk factor score above 8, and a postoperative risk factor score exceeding 5 points should be considered as high risk for the development of a dry socket in a patient. The DSDR score has the potential to assist dental professionals in identifying at-risk patients and implementing tailored preventive strategies to further reduce AO incidence and improve patient care. Furthermore, it is imperative to emphasize that while the DSDR score holds promise as a risk assessment tool for the prevention of AO following tooth extraction, its validation through rigorous empirical studies is an essential step toward its clinical utility. The derivation of the DSDR Score was based on the findings of our study and represents a significant step toward improving patient outcomes in dental practice. However, we acknowledge the need for comprehensive validation to confirm its accuracy and reliability.
We intend to further investigate and validate the DSDR score in larger-scale studies, involving a diverse range of patients and dental practitioners. This validation process will involve a thorough examination of its predictive capabilities and effectiveness in identifying patients at high risk for AO. We will also assess the practicality and feasibility of implementing the DSP protocol in various dental practice settings.
We firmly believe that strict adherence to the DSP protocol, combined with a validated DSDR score, has the potential to significantly contribute to the prevention of this painful condition in dental patients. The validation of these tools will not only enhance their clinical relevance but also serve as a foundation for evidence-based practices in the prevention and management of dry sockets.
Conclusions
The incidence of AO among patients undergoing tooth extraction in the Al-Jouf region was 15.7%. Notably, AO was more prevalent among males than females in our population, and individuals aged between 56 and 77 years exhibited a higher risk of developing AO. Furthermore, multiple tooth extraction cases were associated with a greater incidence of AO. Interestingly, we observed minimal variation in AO incidence between surgical and non-surgical tooth extraction cases and among medically compromised and healthy patients. Nevertheless, operator inexperience significantly increased the likelihood of post-tooth extraction complications. In addition, a promising novel protocol and risk assessment scoring system have been devised which require further validation and future research.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231219420 – Supplemental material for Frequency and etiological denominators of alveolar osteitis at Northern Province of Kingdom of Saudi Arabia—An observational study
Supplemental material, sj-docx-1-smo-10.1177_20503121231219420 for Frequency and etiological denominators of alveolar osteitis at Northern Province of Kingdom of Saudi Arabia—An observational study by Zafar Ali Khan, Namdeo Prabhu, Afsheen Maqsood, Rakhi Issrani, Naseer Ahmed, Maria Shakoor Abbasi, Artak Heboyan and Anand Marya in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231219420 – Supplemental material for Frequency and etiological denominators of alveolar osteitis at Northern Province of Kingdom of Saudi Arabia—An observational study
Supplemental material, sj-docx-2-smo-10.1177_20503121231219420 for Frequency and etiological denominators of alveolar osteitis at Northern Province of Kingdom of Saudi Arabia—An observational study by Zafar Ali Khan, Namdeo Prabhu, Afsheen Maqsood, Rakhi Issrani, Naseer Ahmed, Maria Shakoor Abbasi, Artak Heboyan and Anand Marya in SAGE Open Medicine
Footnotes
Acknowledgements
The authors extend their appreciation to the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia, for funding this work through research grant no. #2130948162.
Authors’ contributions
ZAK, NP, AM, NA, MSA, AH, AM, and RI planned and designed the present work and AM, NA, and MSA were responsible for realizing the work. AM and ZAK were responsible for the data acquisition and analysis. ZAK, NP, and RI drafted the manuscript. MSA, NA, ZAK, AH and AM revised the manuscript. All authors read and approved the final manuscript. NA and AH contributed equally to this work and are corresponding authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia (Project no. #2130948162) in October 2020.
Trial registration
N/A.
Data availability
All data are included in the manuscript. The datasets used and/or analyzed in the present study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.