
Abstract
Objectives:
The aim of the study was to determine the association between oral health–related quality-of-life domains and satisfaction with dental condition of school-age children with dental pain in Ibadan, Nigeria.
Methods:
This cross-sectional study was conducted among 1006 pupils aged 9–12 years who attended 18 randomly selected primary schools in Ibadan, Nigeria. An interviewer-administered questionnaire, Child Oral Impact on Daily Performances inventory in addition to oral examination was used to obtain data. Analysis was done with SPSS 23 and STATA 14 and p-value set at <0.05.
Results:
The prevalence of self-reported dental pain was 10.2%. The mean Child Oral Impact on Daily Performances inventory score was 2.6(±7.2) overall and 9.8(±12.4) for pupils with pain. There was a greater impact on oral health–related quality of life of respondents who reported dental pain than in others (mean rank = 749.54 vs 475.4, U = 21,162, p < 0.001) compared to those with clinically assessed pain (mean rank = 541.21 vs 502.97, U = 6416, p = 0.489). Those who reported dental pain were more dissatisfied with their dental condition (odds ratio = 7.7, 95% confidence interval = 5.0–12.0, p < 0.001) compared to those with clinically assessed dental pain (odds ratio = 1.3, 95% confidence interval = 0.4–4.9, p = 0.687). The direct effect of pain on satisfaction with dental condition and Child Oral Impact on Daily Performances inventory was β = 0.74 (standard error = 0.12, 95% confidence interval = 0.50–0.97, p < 0.001) and β = 0.53 (standard error = 0.05, 95% confidence interval = 0.44–0.63, p < 0.001), respectively. The indirect effect was β = 0.12 (standard error = 0.039, 95% confidence interval = 0.05–0.20, p = 0.001) and the total effect was β = 0.86 (standard error = 0.11, 95% confidence interval = 0.64–1.08, p < 0.001); R2 = 0.21.
Conclusion:
Self-reported dental pain significantly impacted the quality of life of the pupils to cause dissatisfaction with dental condition when compared to clinically assessed pain.
Introduction
Pain is commonly associated with many oral diseases in both children and adults. Dental pain is a sequela of oral diseases such as dental caries, traumatic dental injuries among others in children.1–3 The prevalence of dental pain among children varies across the globe with prevalence rates as high as 64.1% documented among children aged 8 to 12 years in Nigeria, 1 47.5% reported among 8 year olds in England 4 and 33.7% among Brazilian children aged 12–13 years. 2 The high prevalence of dental pain noted in Nigeria has been associated with lower socioeconomic classes and consequently high level of untreated dental condition among the children. 1 Factors such as demographic characteristics have been shown to influence the occurrence and perception of dental pain.1,5–8 Pain of dental origin has been reported as the predominant reason for accessing dental care services among children in low resource settings.9,10
Dental pain has been associated with impaired quality of life.2,11,12 It has negative impacts on physical, functional and psychosocial domains of oral health–related quality of life (OHRQoL) in children.4,11,12 Although the impact of dental pain on the OHRQoL of children has been investigated,1,11–15 little is known about how dental pain affects satisfaction with dental condition among them. In addition, the relationship between the satisfaction with dental condition of children and the domains of oral health quality of life of those with pain remains under researched. This research gap is noteworthy more because dental care–seeking behaviour is likely influenced by self-perception of dental pain9,16,17 and invariably self-assessment of oral health. We, therefore, hypothesized that there is a strong association between impacts on the OHRQoL and dissatisfaction with dental condition among school-aged children with dental pain. The second hypothesis is that dissatisfaction with dental condition among those with pain is mediated by impairment in OHRQoL.
Self-assessment or subjective assessment of oral health such as self-rating of oral health, and satisfaction with dental condition are useful for summarizing oral health status.18,19 They may complement clinical indices to provide holistic care in clinical and non-clinical settings. 20 There is, however, sparse information about satisfaction rating of oral condition in children both in clinical settings and the community making this study important. Investigating how dental pain affects satisfaction rating with dental condition among children and the overall role of OHRQoL will facilitate understanding the applicability of these subjective assessment tools in children. It will also provide insight into the effects of pain on the satisfaction of children with their oral condition. In addition, it will also shed light on the daily activities that must be impaired to cause dissatisfaction with oral condition among children with dental pain in clinical settings and in programme monitoring or evaluation. This study, therefore, assessed the association between OHRQoL domains using the Child Oral Impact on Daily Performances (C-OIDP) index and satisfaction with dental condition of 9- to 12-year-old pupils with and without dental pain in Ibadan, Nigeria.
Methods
Study design
A cross-sectional study was conducted among school pupils aged 9–12 years attending randomly selected public schools in Ibadan metropolis between February 2018 and July 2019.
Sample size
The sample size for the study was calculated using STATA; with an effect size of 1.738 obtained from a previous study 1 and an inflation of 20% (to account for non-response). This generated a minimum sample size of 979.
Sampling
The pupils recruited for the study were selected through multistage random sampling technique. The first stage involved the selection of 18 primary schools from the list of 338 schools obtained from the State Ministry of Education through the use of a table of random numbers. The second stage involved the selection of 9- to 12-year-old pupils within each selected school. The list of pupils in the fourth and fifth grades aged 9 to 12 years in each school was obtained from the school register from which the total number of pupils required in each school were randomly selected. The average number of pupils in each grade was found to be 28 at the time of the study. Therefore, 28 students were selected per grade per school making a total of 56 pupils. Thus, a total of 1008 pupils were approached for the study. The purpose of the study was explained to them and each pupil took home a consent form (in English Language and the translated form in the local language) through which information about the purpose of the study was explained to their parents. Written informed consent was obtained from the parents/legal guardians before recruitment into the study. Only pupils who were available at the time of the study and gave assent participated in the study. Those who were ill were excluded from the study.
Ethical consideration
Ethical approval for the study was obtained from the State Research Ethics Committee. Permission was also sought and obtained from the State Ministry of Education and from the head teachers of participating schools.
Data collection
Information on dental pain and its impact on the OHRQoL was assessed with the use of an interviewer-administered questionnaire (see supplemental material). The questionnaire was administered by two trained research assistants in an empty classroom provided by the school. A student was interviewed at a time by each research assistant. The interviewers were seated at distant ends of the classroom to minimize distraction that could arise when the other interviewer was asking questions or when the child being interviewed was responding.
The questionnaire contained items on the sociodemographic characteristics of the pupils.
Sociodemographic variables
The sociodemographic variables assessed included age at last birthday, gender and the occupation of the parents. Parent’s occupation was categorized into skilled, unskilled and dependents based on the classification by the Office of Population Census and Surveys (OPCS), which has been modified for this environment. 21
Self-reported dental pain
The questionnaire also contained questions adapted from a previously validated questionnaire,1,4 which enquired ‘if the children were experiencing pain from their teeth at the time of the study and in the preceding four weeks’. The single item self-reportage of pain question has been used previously in this environment. 1 The time frame was, however, modified to ensure the periodicity was as close as possible to clinically assessed pain, which was assessed at the time of the study. Self-reported pain was assessed on a graded pain severity scale of 1 to 10 with 10 as the worst pain.
Oral health–related quality of life
The impact of dental pain on the OHRQoL was assessed with the C-OIDP inventory that had been validated in the country. 22 The C-OIDP assesses the impact of oral conditions on eight daily activities (Figure 1). The daily activities are eating and enjoying food, speaking/pronouncing words, teeth cleaning, smiling, sleeping/relaxation, emotional stability, doing school work and enjoying social contact. 23 The C-OIDP is quantified on a response frequency scale and severity scale ranging from ‘0 to 3’. The total C-OIDP score was obtained, in the study, by multiplication of the frequency and severity scores for each pupil.
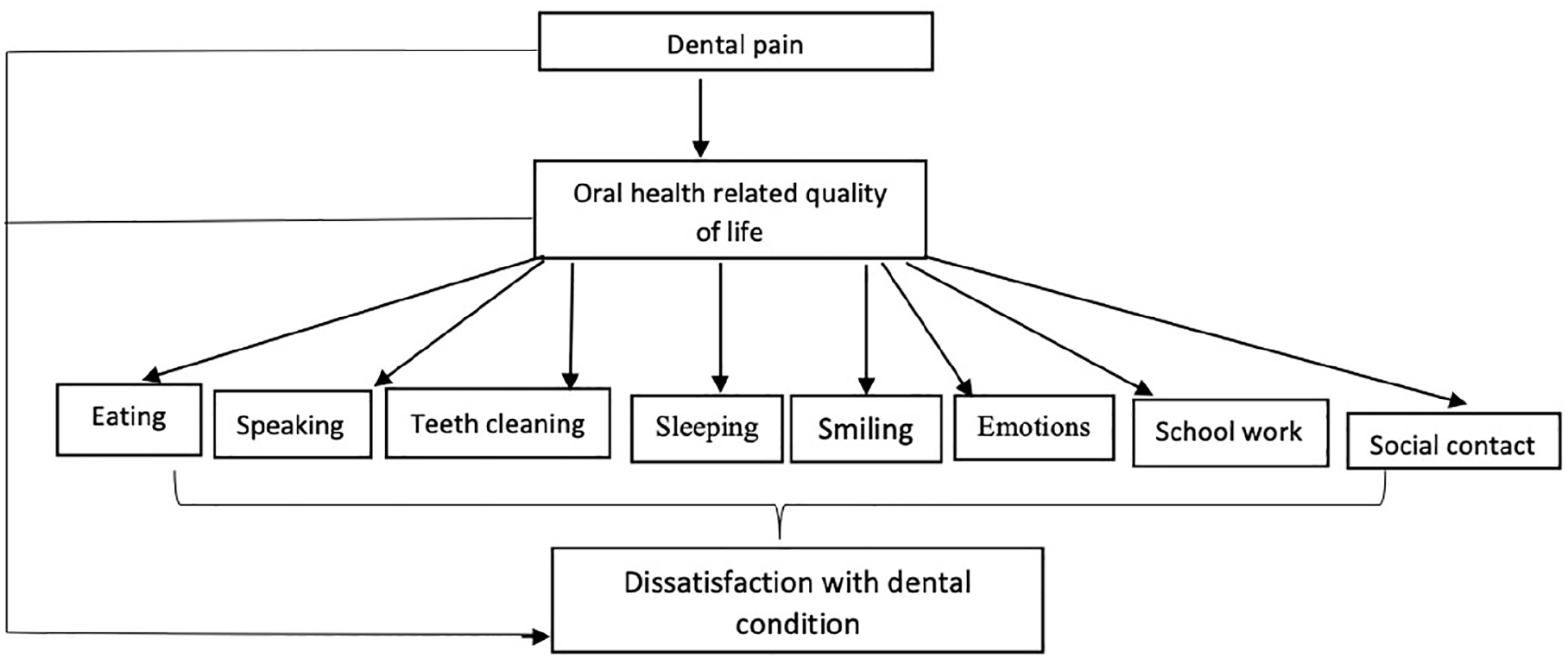
Theoretical model.
The theoretical framework for the study
The theoretical framework for the study was adapted from the World Health Organization (WHO) International Classification of Impairments, Disabilities and Handicaps that was modified for dentistry by Locker. 24 It forms the theoretical framework for C-OIDP. 23 For this study, the effect of the intermediate level, which dental pain falls into, was considered. The intermediate level recognizes the earliest negative effect of impairment of oral health status (first level). Dental pain was considered as exposure that could have negative impacts on satisfaction with dental condition as well as daily performances from the C-OIDP domains. The study investigated the relationship between satisfaction with dental condition, and daily performances among those with or without dental pain. The primary outcome was the overall quality of life and the daily performances. The secondary outcome was satisfaction with dental condition. Thus, the dependent variable was considered as satisfaction with dental condition. Pain was considered as the independent variable and C-OIDP was considered as the mediatory variable.
Satisfaction with dental condition
In addition, satisfaction with the dental condition of each participant was assessed and the response was recorded as ‘very satisfied’, ‘satisfied’, ‘indifferent/don’t know’, ‘very dissatisfied’ or ‘dissatisfied’. Satisfaction with dental condition is a single-item tool for subjective assessment based on the same theoretical model as the self-rating of oral health that has been used widely. 24
Translation of questionnaire
For ease of communication and standardized interviews, the questionnaire was translated to Yoruba, the local language by an expert linguist and back translated to English language by another independent linguist. The two English versions of the questionnaire were compared and differences were found to be minor.
Clinical assessment of dental pain
Presence or absence of tenderness to gentle percussion of tooth/teeth was evaluated by a trained and calibrated dentist with a wooden spatula. 25 The intra-examiner’s kappa score was 0.9.
A pilot study was conducted prior to the study among children aged 9 to 12 years in a school that was not included in the study to determine the feasibility of the study and comprehensiveness of the questionnaire. The convergent validity of satisfaction with dental condition was evaluated by comparing with self-rating of oral health. 26 The correlation coefficient was rs = 0.811, p < 0.001, signifying good convergence and both measures being on the same construct, since the recommended correlation value is about 0.7. 26 Also, the convergent validity of tenderness to gentle percussion and the modified pain question was assessed (rs = 0.072, p = 0.023). This indicated significant association but low correlation; confirming that the two measures are not based on the same construct but are related. 26 A preprint from the research project has been published online. 27
Data analysis
Data obtained were collated and subjected to statistical analysis using SPSS version 23 and STATA version 14. Normality test for C-OIDP score was assessed using Shapiro–Wilk statistics, a significant value indicated non-normality. Therefore, a non-parametric test, Mann–Whitney statistics, was used to test for association between C-OIDP scores and categorical variables. For other analysis, C-OIDP was recoded into ‘C-OIDP = 0’ (no impact on quality of life) and ‘C-OIDP ⩾ 1’ (impact on quality of life). Bivariate association between independent variables and dichotomized C-OIDP score was evaluated using chi-square statistics. Association between dichotomized C-OIDP score and pain assessment types (self-reported and clinically assessed) was evaluated using binary logistic regression. For ease of analysis, satisfaction rating of dental condition was collapsed into a binary variable as ‘satisfied’, which included the responses ‘very satisfied’, ‘satisfied’ and ‘dissatisfied’, which included ‘indifferent/don’t know’, ‘dissatisfied’ and ‘very dissatisfied’. Binary logistic regression was used to obtain crude odds ratio (OR) and adjusted OR, while controlling for sociodemographic variables; age, gender and parent occupational class to assess the association between the C-OIDP items, pain and satisfaction rating of dental condition. The mediatory role of OHRQoL and C-OIDP items on satisfaction with dental condition among those with and without pain was assessed with mediation analysis using STATA 14. The model fit was assessed using Comparative Fit Index (CFI), Tucker Lewis Index (TLI), Standardized Root Mean Square Residual (SRMR) and Root Mean Square Error of Approximation (RMSEA). A value of ⩽ 0.06 was considered acceptable for RMSEA, ⩽ 0.08 for SRMR and ⩾ 0.95 for CFI and TLI. 28 Bootstrapping of the standard error (SE) estimates and confidence intervals (CIs) was also conducted. 29 Non-inclusion of 0 in the CI as well as a p-value < 0.05 was considered to be statistically significant and an indication of presence of mediation. 29
Results
A total of 1006 pupils participated in the study out of the 1008 approached for recruitment, that is, a response rate of 99.8%. The mean age of the participants was 10.5 (SD = 1.1) years and 478 (47.5%) were females (Table 1). One hundred and three (10.2%) reported dental pain, while 14 (1.4%) had at least a tooth that was tender to percussion on oral examination. The majority (83.0%) were satisfied and 10 (1.0%) were very satisfied, 10 (1.0%) could not say/indifferent, 138 (13.7%) were dissatisfied and 23 (2.3%) were very dissatisfied with the condition of their mouth.
Sociodemographic characteristics of study participants and association with pain.

The standardized Cronbach’s alpha value of the C-OIDP scale was 0.94. The Cronbach’s alpha value was reduced when each of the items of the scale was deleted, suggestive of the importance of each item of the C-OIDP scale. Inter-item correlation coefficient ranged from 0.2 to 0.9.
A total of 212 (21.1%) pupils had at least an impact of oral health on their quality of life. The C-OIDP score ranged from 0 to 63. The mean C-OIDP score was 2.6 (±7.2) overall, 9.8 (±12.4) for pupils with self-reported dental pain and 3.6 (±7.8), for those with clinically assessed dental pain. (Shapiro–Wilk statistics = 0.425, p < 0.001). The median C-OIDP value was 0 overall and equally 0 for pupils with clinically assessed dental pain. The median C-OIDP value was 6.0 for those with self-reported dental pain.
There was no difference in the proportion of the pupils by age, gender and occupational class of the parents with respect to self-reported dental pain (Table 1). However, clinically assessed pain was influenced by the occupational class of the parents (Table 1). Seventy-one (68.9%) pupils with self-reported dental pain reported at least an impact on quality of life compared with 141 (15.6%) pupils without dental pain (χ2 = 158.07, p < 0.001).
Respondents who reported dental pain had higher impairment of OHRQoL with higher OIDP mean ranks compared to those who did not (Table 2).
Self-reported, clinically assessed pain and impacts on the oral health–related quality of life with C-OIDP items.

C-OIDP: Child Oral Impact on Daily Performances inventory.
Statistically significant Mann–Whitney U test value.
Furthermore, all the OIDP items were affected by self-reportage of dental pain (Table 2). Respondents with clinically assessed dental pain also had higher impairment of OHRQoL than those who did not have dental pain on clinical evaluation. All the C-OIDP items were negatively affected except for speaking where those with pain had lower mean ranks (Table 2). Eating and enjoying food was the most frequently reported activity that was affected by pain (Table 2).
A total of 835 (83.0%) respondents were very satisfied or satisfied with their dental condition and 171 (17.0%) were very dissatisfied or dissatisfied. A higher proportion (53.4%) of respondents with self-reported pain were dissatisfied with their dental condition than those without pain (12.8%), p < 0.001. Children who reported dental pain were more dissatisfied with their dental condition (OR = 7.7, 95% CI = 5.0–12.0, p < 0.001) compared to those with clinically assessed dental pain (OR = 1.3, 95% CI = 0.4–4.9, p = 0.687).
Bivariate analysis of self-reported dental pain and dissatisfaction with dental condition revealed that among children who reported dental pain, a higher proportion of those who were dissatisfied with their dental condition had impacts on eating and enjoying food, cleaning teeth, sleeping/relaxing, social contacts and overall quality of life (Table 3).
Satisfaction rating of dental condition and impairment of the C-OIDP items of pupils with self-reported dental pain (n = 103).

C-OIDP: Child Oral Impact on Daily Performances inventory.
Statistically significant.
Multivariate analysis showed that among children with dental pain; those who were dissatisfied with their dental conditions were more likely to report impairment in maintaining social contact (OR = 10.4, 95% CI = 1.3–85.0, p = 0.028), teeth cleaning (OR = 3.4, 95% CI = 1.5–7.8, p = 0.003), eating and enjoying food (OR = 3.0, 95% CI = 1.3–6.9, p = 0.011) and in overall quality of life (OR = 2.6, 95% CI = 1.1–6.0, p = 0.032), (Table 4). The C-OIDP items were still significantly affected when age, gender and parental occupational class were controlled for in the analysis. The odds of impairment of sleeping and relaxation was significantly increased when sociodemographic characteristics were controlled for (Table 4).
Logistic regression analysis of association between satisfaction rating of dental condition and C-OIDP items among children who reported dental pain (n = 103).
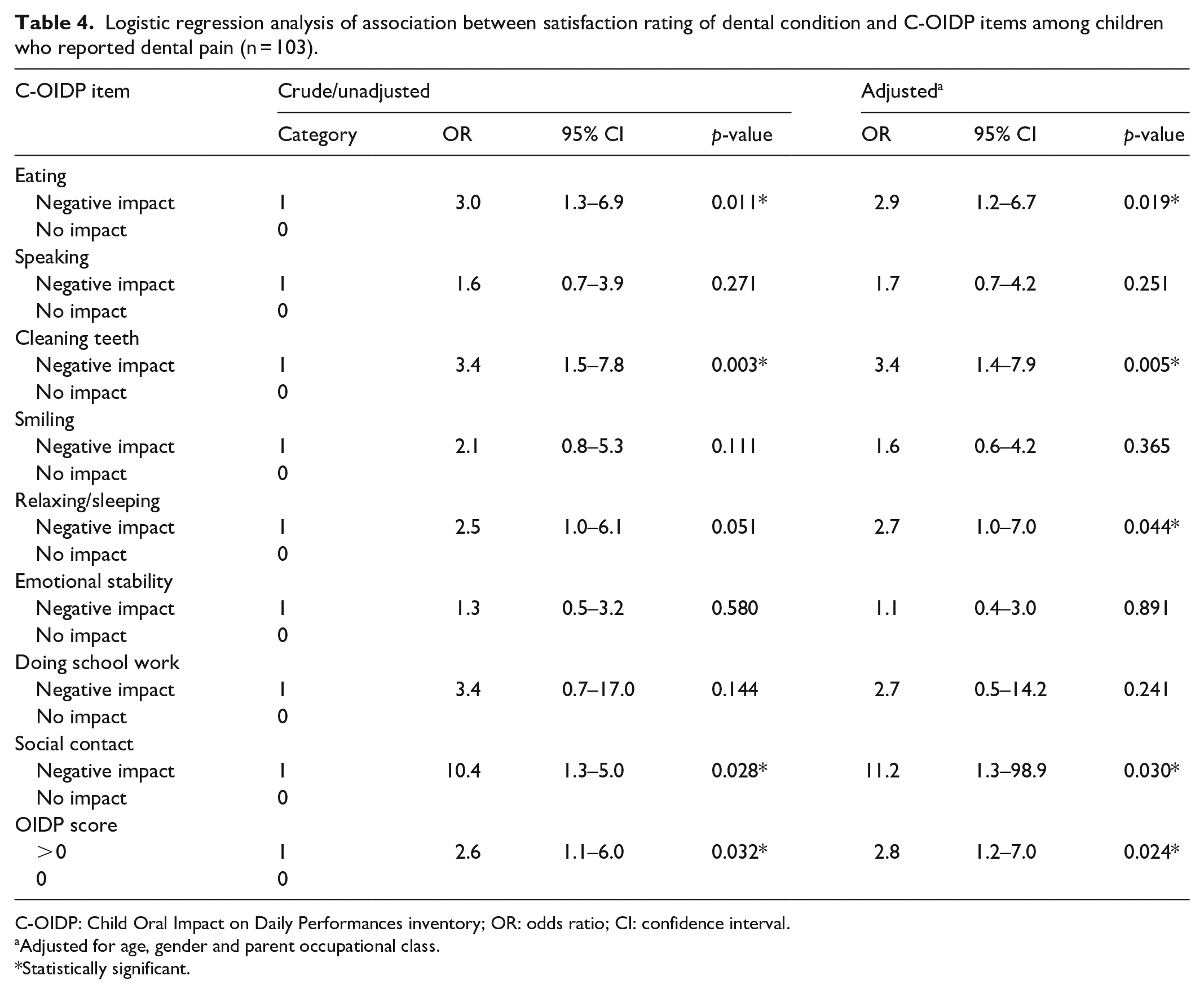
C-OIDP: Child Oral Impact on Daily Performances inventory; OR: odds ratio; CI: confidence interval.
Adjusted for age, gender and parent occupational class.
Statistically significant.
The model of fit indices for the mediation analysis (Figure 2) showed that RMSEA and SRMR were both 0, and CFI and TLI were both 1 indicating a good fit. The direct effect of pain on satisfaction on dental condition was β = 0.74 (CI = 0.50–0. 97, SE = 0.12, Z = 6.43, p < 0.001). The direct effect of pain on quality of life was β = 0.53 (CI = 0.44–0.63, SE = 0.05, Z = 11.30, p < 0.001). The direct effect of quality of life on satisfaction with dental condition was β = 0.23 (CI = 0.09–0.37, SE = 0.07, Z = 3.27, p = 0.001). The indirect effect was β = 0.12 (CI = 0.05–0.20, SE = 0.039, Z = 3.18, p = 0.001) and the total effect was β = 0.86 (CI = 0.64–1.08, SE = 0.11, Z = 7.70, p < 0.001); R 2 = 0.21.

Mediation analysis of relationship between pain, C-OIP and satisfaction rating of dental condition.
Discussion
The study showed that self-reported dental pain negatively impacted on the OHRQoL of children aged 9 to 12 years and caused dissatisfaction with dental condition among them. Children who reported dental pain had sixfold negative impact on their quality of life when compared to other participants. This is a reflection of the magnitude that dental pain has on affected children and a need to institute prevention strategies among school-age children to limit the impact of pain on their OHRQoL. The negative impact of self-reported pain on the OHRQoL has been reported by other authors.1,4,11,14 In addition, the high burden of untreated oral conditions such as dental caries among children from low resource settings may have contributed to this finding. 1
The daily activity that was most frequently affected by dental pain was ‘eating and enjoying food’. The role of food in everyday living may be partially responsible for this finding. It is not surprising as the major role of the mouth reported by school-aged children in a similar setting was eating. 30 Importantly, the negative effect of pain from the mouth on eating is in line with what had been documented by other authors.31,32 The next ranked activity affected by pain was ‘cleaning the teeth’. Cleaning of the teeth requires touching of the teeth with tooth cleaning aid and as such a potential aggravating factor to elicit pain during the act of tooth cleaning. Other activities of the C-OIDP were also affected and included ‘speaking and pronouncing words’, ‘sleeping and relaxing’, ‘maintaining social contact’, ‘maintaining emotional stability’, ‘smiling’ and the last being ‘doing school work’. The finding of ‘doing schoolwork’ as the least-reported activity affected by pain may be alluded to the fact that school work is given priority by pupils, parents and teachers. In addition, missing school is usually not taken lightly by all concerned except the child is obviously ill, which often does not take into cognisance dental conditions.
There was little impact of clinically assessed dental pain on OHRQoL of respondents in the study compared to self-reported dental pain. This may be attributed to the different causes of pain evaluated by percussion of the tooth, which could be periapical pathology as is the case of vertical percussion and periodontal pathology with lateral percussion of the teeth. 25 Therefore, the causes of dental pain affecting these children may not be associated with any of the above-listed pathologies. In addition, it is a pointer to the importance of individual assessment or perception of pain, which may differ significantly from that of the clinician’s assessment.
Furthermore, the weak correlation between clinical assessment of dental pain and self-report of dental pain corroborates previous documentation about the weak association between subjective assessment of oral condition and clinical measures.20,33 This low correlation, however, does not invalidate the single-item self-report of pain. 33 More so, the two forms of dental pain assessment belong to different constructs of health assessment. 20 Further investigations into the association between clinically assessed dental pain and OHRQoL using other objective methods will be worthwhile.
More than half of the respondents who reported dental pain were dissatisfied with their dental condition. Parents have been documented to report their children’s dissatisfaction with oral conditions on account of pain. 34 This is suggestive of the crucial role that dental pain plays in the perception of dental condition as being satisfactory or otherwise in children. It is thus worthy of note to clinicians as well as caregivers to place children’s satisfaction with their dental conditions at the frontiers of management for a better treatment outcome. Importantly, it may explain the reason why pain is the main motivator for children who seek dental care in low resource settings.9,10 The impact of dental pain on the OHRQoL affected all the domains; physical, psychological and social. This is another likely explanation for the aforementioned dental care–seeking behaviour as observed among children. 32 Furthermore, the relevance of satisfaction ratings of dental condition among children in the monitoring and evaluation of population-based interventions and dental care programme cannot be over-emphasized. These findings highlight the importance of dental pain as a negative factor that impacts the OHRQoL of children and is also strong enough to cause dissatisfaction with their oral health condition.
‘Eating and enjoying food’, ‘tooth cleaning’, ‘sleeping and relaxing’ and ‘enjoying contact with other children’ were the C-OIDP items that were most often negatively impacted upon by pain and associated with dissatisfaction with dental condition. These findings suggest that the pupils rate the aforementioned activities highly. In addition, any negative impact or inability to engage in these activities, as in this case dental pain, may influence their perception and result in eventual dissatisfaction with the state of their oral conditions. These activities should be checked both in the clinic and field settings as the case may be to ascertain the success of treatments and interventions implemented. In addition, reporting dental pain by children resulted in almost eight folds of dissatisfaction with dental condition. This finding supports the application of the satisfaction rating of dental condition, a useful complementary tool, in the monitoring and evaluation of dental pain both at the clinic level and in population-based interventions. This fact was further elucidated by dissatisfaction with dental condition among children with pain being mediated by negative effects on OHRQoL. In addition, it brings to the forefront that dissatisfaction with dental condition from pain is as a result of some form of impaired OHRQoL.
A limitation of the study was not evaluating the association of major oral diseases in children aged 9–12 years, such as dental caries, with pain and quality of life. This was not considered an objective of this study because it had been reported by other studies. Thus, we investigated the early effects of the disease (pain), a major complaint among this age group as well as the driving force for them to seek dental treatment. Another limitation of the study is recall bias of self-reported pain by the study participants, which was, however, minimized by reducing the duration of self-reported pain to the four weeks preceding the study.
Conclusion
Self-reported dental pain significantly impacted the quality of life of the pupils and caused dissatisfaction with dental condition when compared to clinically assessed pain.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211025944 – Supplemental material for Satisfaction with dental condition and oral health–related quality of life of school-age children with dental pain in Ibadan, Nigeria
Supplemental material, sj-pdf-1-smo-10.1177_20503121211025944 for Satisfaction with dental condition and oral health–related quality of life of school-age children with dental pain in Ibadan, Nigeria by Folake Barakat Lawal and Gbemisola Aderemi Oke in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge all the pupils who participated in the study and the teachers who assisted in the conduct of the study. Special thanks to Dr T.A. Lawal who assisted with statistical input and proof reading of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Publication of the research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No: B 8606.R02), Sida (Grant No: 54100113), the DELTAS Africa Initiative (Grant No: 107768/Z/15/Z) and Deutscher Akademischer Austauschdienst (DAAD). The DELTAS Africa Initiative is an independent funding scheme of the African Academy of Sciences (AAS)’s Alliance for Accelerating Excellence in Science in Africa (AESA) and supported by the New Partnership for Africa’s Development Planning and Coordinating Agency (NEPAD Agency) with funding from the Wellcome Trust (United Kingdom) and the UK government. The statements made and views expressed are solely the responsibility of the Fellow.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.