
Abstract
Background and Objective:
Foodborne botulism is one of the potentially fatal forms of food poisoning, usually caused by ingestion of home-canned vegetables, fruits, and dairy and fish products. This study aimed to assess the frequency of signs and symptoms in patients with botulism following the ingestion of homemade Doogh, a traditional milk-based beverage, in Hamadan, Iran in 2023. We also examined the general characteristics of the recruited patients.
Methods:
During an outbreak, 21 patients were referred to the hospital because of food poisoning. All patients had a history of consumption of Doogh. After careful physical examination, all of them were hospitalized. Botulism was suspected in all patients except for the first patient.
Results:
The mean age of admitted patients was 33.09 ± 18.44 years, with 23.80% being males and 76.20% females. Incubation period in our patients was 68 ± 28.48 h. Notable symptoms included diplopia (95.23%), nausea and vomiting (85.71%), blurred vision (80.95%), and dizziness (61.90%). The laboratory results were within the normal range. No deaths occurred in this patient cohort. Furthermore, botulinum spores were detected in Doogh samples collected from the outbreak, confirming the presence of Clostridium botulinum spores as a source of the outbreak.
Conclusions:
This study highlights that the initial manifestations of botulism predominantly involved ophthalmologic abnormalities in most patients. Additionally, symptoms such as nausea, vomiting, and dizziness may manifest in cases of foodborne botulism. Timely diagnosis and treatment of botulism following the consumption of homemade Doogh played a crucial role in achieving positive outcomes, with no fatalities recorded in this patient cohort.

Introduction
The serious illness known as botulism, which can affect both humans and animals, is characterized by flaccid paralysis that can eventually lead to respiratory difficulties and, in the most severe cases, fatal results. The toxigenic Clostridium botulinum (C. botulinum) produces a strong neurotoxin that is the underlying cause of this illness. 1 C. botulinum is a gram-positive spore-forming anaerobic bacterium that generates a distinctive neurotoxin that may be identified immunologically by utilizing certain neutralizing antisera.2,3
The typical type of botulism, known as foodborne botulism, is produced when toxins from food enter the human body through the gastrointestinal tract. However, additional, rare types of botulism have been documented, including newborn botulism, adult intestinal colonization botulism, and wound botulism. 4 Double vision, dry mouth, dysphagia, dysphonia, paralysis of the limb muscles that may quickly spread to encompass the breathing muscles, respiratory failure, and death are among the clinical signs of botulism. 5
Small outbreaks mostly happen at the local level, and home-prepared foods are generally to blame for rare occurrences. Large epidemics involving several areas or nations may be brought about by commercially manufactured foods. These latter epidemics provide a problem for local and regional health systems since botulism can cause respiratory failure necessitating hospitalization in critical care units for weeks or months. 6
When compared to other forms of food poisoning, outbreaks of foodborne botulism may appear to be relatively uncommon, but they have substantial public health repercussions due to their severe clinical effects and expensive treatment options. 7 Dairy, meat, and vegetable items in cans are frequently linked to foodborne botulism. 8 Despite the fact that outbreaks of foodborne botulism have not commonly included milk and milk products, an increase in the incidence of outbreaks in dairy cattle has been recorded, alerting the public health community about the safety of milk and milk products.9,10 Notably, dairy products like cheese and yogurt have already been linked to a number of botulism outbreaks.11,12
Iran has seen many botulism outbreaks in the past 10 years, mostly in northern districts bordering the Caspian Sea and fish products were the main sources. 13 For every 100,000 Iranian men and women, there are 7.1 and 3.3 cases of foodborne botulism annually, respectively. 14 According to current national surveillance statistics, home-prepared traditional processed fish, commercially canned fish, fish spawn, dairy products, vegetables, and home-prepared legumes, cottage cheese, and canned fruits are common causes of foodborne botulism in Iran. 14
In the context of this study, we focus on a specific outbreak that occurred in Hamadan, Iran linked to the consumption of Doogh, a traditional Iranian beverage created by blending plain yogurt with water and salt, chilling it, and serving it alongside traditional Iranian dishes.
Understanding the unique circumstances and clinical presentations of this outbreak not only provides valuable insights into the dynamics of botulism but also highlights the need for proactive measures to prevent similar occurrences in the future. It also underscores the critical significance of early symptom recognition and immediate treatment in effectively managing such cases. Our research sheds light on the underexplored risk of homemade Doogh as a potential source of botulism, offering vital insights for public health measures and prevention strategies.
Method
Patient selection
From 3 to 10 January 2023, all patients referred to Sina and Besat Hospitals in Hamadan, Iran, with gastrointestinal problems, respiratory discomfort, or descending paralysis following the consumption of traditional Doogh during a family meal were admitted for evaluation and treatment. Inclusion criteria encompassed patients of all ages and both genders who presented with symptoms of gastrointestinal distress, respiratory discomfort, or descending paralysis within 72 h of consuming homemade Doogh. Exclusion criteria included individuals with pre-existing neurological conditions, a history of allergies to any Doogh ingredients, or those who did not consume Doogh during the family meal.
Ethical considerations
Ethics approval for this study was waived by the Ethics Committee of Hamadan University of Medical Sciences, as case series and case reports at our institution are classified as exempt or non-regulated research categories. Nonetheless, this study was conducted in full compliance with ethical principles as outlined in the Declaration of Helsinki and international guidelines, with strict adherence to ethical considerations, patient confidentiality, and data protection.
In our investigation of the botulism outbreak, at first, we obtained verbal consent from patients. The process of obtaining verbal consent was thoroughly documented in patient records to maintain transparency and ethical standards. Additionally, after the initial treatment, we promptly obtained written consent from the patients for publication of their data on scientific journals in order to ensure full compliance with ethical standards and to provide a comprehensive record of their informed consent. This two-step approach allowed us to prioritize patient care while still upholding ethical standards, patient confidentiality, and data protection.
Description of Doogh
Doogh is a popular cooling beverage commonly prepared with yogurt, water, and salt, often served cold or with ice.
Initial diagnosis
With the exception of the first patient, all patients were initially diagnosed as suspected cases of botulism based on their clinical presentations and history of Doogh consumption.
Criteria for likely case of botulism
In this study, a patient was considered a likely case of botulism if they exhibited signs of bilateral cranial nerve neuropathy, such as diplopia, impaired vision, dysphagia, bulbar paresthesia, and/or symmetrical weakness in peripheral muscles.
Sample collection
Biologic samples, including gastrointestinal contents, and feces, were collected from each patient for laboratory analysis within a timeframe ranging from 12 to 120 h after the ingestion of Doogh. Additionally, samples of every meal that ingested were collected and sent to the reference laboratory at the Pasteur Institute of Tehran to test for C. botulinum toxins. 15
Blood samples were drawn for laboratory analysis, encompassing white blood cell count, neutrophils percentage, lymphocytes percentage, hemoglobin levels, platelet count, urea levels, creatinine levels, blood gas analysis, and serum bicarbonate levels. 16 These samples were collected to assess various aspects of the patients’ health status and to aid in the diagnosis and management of botulism following the consumption of homemade Doogh.
Treatment
All patients, except the first case, received trivalent botulism antitoxin immediately after sample collection and on the same day as their admission. For the first case, treatment was initiated 12 h after admission due to clinical assessment and diagnostic confirmation.
Data collection
Data collection was conducted by a team of healthcare professionals specializing in infectious diseases, including physicians, nurses, and our clinical researchers. The process involved clinical interviews and physical examinations of the patients. Each patient was individually interviewed and examined by a designated healthcare provider responsible for collecting comprehensive clinical data. The interviews and examinations were carried out upon admission to the hospital and throughout the patients’ hospital stay, allowing for the continuous assessment of symptoms and clinical progress.
Assessment of consciousness
The level of consciousness in the patients was evaluated using the Glasgow Coma Scale (GCS), a standardized clinical tool widely recognized for neurological assessment. 17 Trained healthcare providers conducted GCS assessments upon admission and during the patients’ hospital stay to monitor changes in consciousness.
Outcome assessment
In our study, the assessment of outcomes was conducted at specific time points following the onset of symptoms and signs. The outcomes were evaluated at regular intervals, with the first assessment occurring 24 h after the initial appearance of symptoms and subsequent assessments at 48 h and 7 days post-onset.18 –20
Statistical analysis
Descriptive statistical analysis was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) software to summarize the demographic and clinical data of the patients. Data were presented as means ± standard deviations (SD) for continuous variables and as percentages for categorical variables.
Results
Demographic data
Based on our study, the mean age of admitted patients was 33.09 ± 18.44 (range: 6–87) years. Furthermore, 23.80% of patients were males while 76.20% were females. The medical history was taken from all participants, and most of the patients (87.6%) had no history of chronic diseases. All the included cases presented to the hospital from 12 to 120 h after Doogh ingestion with a mean value of 68 ± 28.48 h (Figure 1).

Twenty-one cases of botulism, by interval between eating in the party and onset of first symptoms (incubation period).
Assessment of the cases
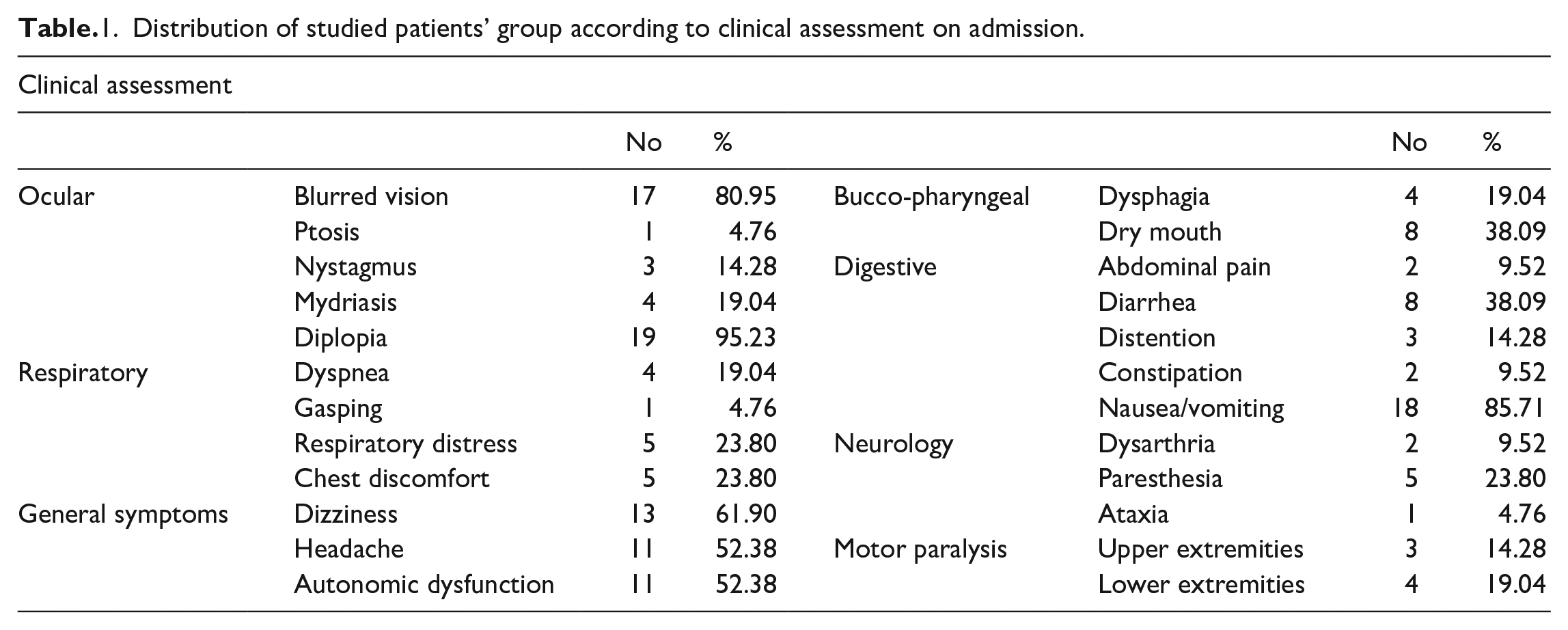
In the initial evaluation, 76.20% of the patients had a GCS score of 15, indicating full alertness and consciousness, whereas 23.80% of them had a GCS score less than 15, indicating a decreased level of consciousness. The most common findings observed in admitted patients were diplopia (95.23%), nausea and vomiting (85.71%), blurred vision (80.95%), and dizziness (61.90%) (Table 1).
Distribution of studied patients’ group according to clinical assessment on admission.
Laboratory results of patients
The laboratory finding of the included patient showed in Table 2. As demonstrated in Table 2, all laboratory parameters were in normal range.
The laboratory results of patients.

Detection of botulinum spores in samples
In our study, biological samples, such as gastrointestinal contents and feces, tested positive for the presence of botulinum toxin and C. botulinum spores in all of our patients, thereby confirming the diagnosis of botulism.
Furthermore, we forwarded samples of the suspected food items to the Pasteur Institute for a detailed analysis. The results confirmed the presence of botulinum spores in the Doogh sample, establishing a direct link between the contaminated food and the outbreak. To enhance clarity, we have included a dedicated figure in this subsection to visually depict the detection of botulinum spores (Figure 2). These Doogh samples underwent laboratory culturing and were subjected to staining using the Malachite Green staining method, 21 which enabled us to visualize the presence of botulinum spores.

Visualization of botulinum spores in Doogh samples using malachite green staining.
Duration of hospitalization, ICU admission, and need for mechanical ventilation support
The range of hospitalization was 1–5 ± days with a mean of 2.33 ± 1.79 days. Moreover, six patients (28.57%) were admitted to ICU and among them two patients were needed mechanical ventilation for a period of 1–3 days.
The outcome
Become symptomless was the most prevalent outcome (85.71%), whereas neurological sequelae were persisted in 14.28% of patients in the form of persistent constipation, distention, and dry mouth with very mild dysphagia at 7 days post-onset. Death did not occur in this series of patients.
Discussion
Botulism from food is a very uncommon but potentially lethal illness. Most instances are isolated or brief outbreaks. Several outbreaks have been observed in Iran during the past 20 years. Most epidemics in the northern and western areas affected rural populations. The most popular sources were fish products, conventional cheese and whey, and home-canned vegetables. An unusual botulism epidemic linked to the ingestion of home-made Doogh was the subject of our report. Doogh is a popular Persian yogurt beverage that is created by combining yogurt with salt and water. It could be made in a rural region under risky circumstances.
The first confirmed cases of foodborne botulism with Doogh in Iran are described in this case series. The outbreak was caused by type A of botulinum toxin. The most crucial step in diagnosis and directing therapeutic therapy quickly is to first investigate botulism based on clinical presentation and clustering of cases. To rule out neurological diseases, previous strokes, and other gastrointestinal issues, previous medical and surgical histories were obtained. In the current study, 87.6% of the patients had no prior surgical or medical history and after consuming the Doogh, the patients’ symptoms began to manifest in full.
With a mean of 68 ± 28.48 h, all the included patients arrived at the hospital between 12 h and 5 days after Doogh ingestion. According to Fleck-Derderian et al.’s 22 systematic review, the median time between exposure and the onset of symptoms is about 1 day. This discrepancy is anticipated given that foodborne botulism can take up 16 days to incubate. After ingesting the produced toxin, symptoms of foodborne botulism often appear 12 to 36 h later. 23 The incubation time in our patients ranged from 12 h to 5 days. When the volume of the produced toxin inoculation is minimal, incubation periods as long as 1 week are seen.
In terms of laboratory assessment of included patients in this outbreak, mean of each item were in normal range. Thus, it can be concluded that laboratory markers are not suitable options for diagnosis of botulism and physician must rely on clinical findings in suspected patients.
Botulism has a specific clinical symptom, but its diagnosing requires a high level of suspicion. Diplopia (95.23%), nausea and vomiting (85.71%), blurred vision (80.95%), and dizziness (61.90%) were also reported by patients in the current research. This is consistent with the findings of Gaware et al. 24 who claimed that these symptoms are typical of botulism. The gastrointestinal tract and central nervous systems are mostly involved in the symptoms, and in this way this case series is comparable to others that have been published elsewhere.25 –28
The attack rate is not 100%, as was established during the past epidemics of foodborne botulism.29,30 In our study, out of 30 people present at the party who drank Doogh, only 21 people presented symptoms of botulism toxicity. Unequal distribution of the toxin in the meal, a dose-response relationship, or unidentified host variables that impart resistance to the poison can all be used to explain the attack rate of 70% among those who consumed it. The diagnosis of foodborne botulism is aided by the clinical presentation and the presence of toxins in the blood, feces, vomitus, or food of a suspected case. 27
Nausea/vomiting and diarrhea were typical early symptoms in this outbreak, as it is in cases of foodborne botulism. 31 In addition to botulinum toxins, bacteria and/or viruses that contaminate the same food source can also induce diarrhea. Furthermore, Because the parasympathetic fibers in the oculomotor nerve were unaffected, pupils might be reactive without mydriasis, as in the examples that were documented. Botulism-related altered mental state may result from inadequate oxygenation, infection, or other metabolic problems. 32 Clinical indications and symptoms as well as epidemiologic case investigation are crucial, particularly in situations when laboratory test findings may be unavailable or delayed. Myasthenia gravis, tick paralysis, Guillain–Barre syndrome, poliomyelitis, stroke, and heavy metal toxicity are among the conditions in the differential diagnosis for foodborne botulism.33,34
In our study, we did not initiate treatment for the first patient until we received the laboratory results confirming the presence of botulinum spores. However, for the remaining patients who exhibited suspicious symptoms and had participated in the same event, we immediately initiated treatment as a precautionary measure to ensure their well-being. This approach allowed us to prioritize patient care and provide timely treatment to those at risk. In cases of suspected botulism, timely intervention is crucial. While awaiting laboratory confirmation, immediate treatment initiation is recommended based on clinical presentation. This approach aims to prevent potential complications and reduce the risk of mortality. Initiation of antitoxin treatment should not be delayed, especially when patients exhibit classic botulism symptoms, such as cranial nerve neuropathy and descending paralysis.34,35
In our study, 9.52% of patients was needed mechanical ventilation, as a supportive therapy.22,36 Early treatment with botulism antitoxin can neutralize circulating botulinum toxin and prevent the disease development. Regrettably, antitoxin cannot repair the damage that has already been created. 37 This was in agreement with Anderson et al. 38 and Barker et al. 39 who started the botulism antitoxin treatment after the appearance of the confirmed signs of intoxication. Following the beginning of the botulism antitoxin after certainly proven indicators, full recovery happened in 85.71% of the participants and 14.28% of patients who had complications in the current research. They reported having a constant dry mouth and very moderate dysphagia that did not prevent them from ingesting liquid, solid, or semisolid meals. Some people reported having constipation, which became better after they used laxatives. 40 This is comparable to the findings of the study by Gottlieb et al., 41 who came to the conclusion that earlier signs of a cholinergic autonomic blockade, such as dry mouth, which are conspicuous during botulism, would continue for a long time after that.
Public health teams may use this outbreak study as a point for future detection and response to similar epidemics. To determine the scope of botulism and create preventative plans for this recently diagnosed disease in Iran, the Ministry of Health and Regional Health Bureau must come up with a coordinated approach to disease monitoring, detection, confirmation, and treatment. Clinicians and public health authorities should work closely together at all levels to identify potential clusters of botulism quickly and conduct thorough investigations to determine the primary source of infection and the precise method of the bacilli's risk introduction into the involved food. 42
Botulism from food is a rare yet severe illness, and our study provides valuable insights into a specific outbreak linked to the consumption of homemade Doogh in Hamadan, Iran. However, it is essential to acknowledge the limitations of our study, which can help contextualize the findings. First, our investigation did not involve a formal sample size calculation based on statistical power analysis. The sample size of 21 participants was primarily determined by the number of cases available during the outbreak and the feasibility of conducting a comprehensive clinical study within the given timeframe. This limitation may affect the generalizability of our findings to a broader population. Future research endeavors in this field should prioritize power analysis for sample size calculation to enhance the robustness of study outcomes and improve the precision of results. Second, the cases presented in our study may not fully represent the diversity of botulism cases that could occur in different settings. The exact timing of symptom onset in relation to Doogh consumption varied among patients and was not uniform. This variability could introduce confounding factors in the analysis. Moreover, the foodborne botulism is a complex and rare condition, and there is still much to learn about its long-term outcomes. We acknowledge the need for further research to investigate the extended outcomes and potential complications that may arise beyond the scope of our study.
Conclusion
This study highlights that the initial manifestations of botulism predominantly involved ophthalmologic abnormalities in most patients. Additionally, symptoms such as nausea, vomiting, and dizziness may manifest in cases of foodborne botulism, typically associated with the consumption of improperly fermented, preserved, or home-canned foods. Timely diagnosis and treatment of botulism following the consumption of homemade Doogh played a crucial role in achieving positive outcomes, with no fatalities recorded in this patient cohort.
Footnotes
Acknowledgements
The authors thank Dr. Mohammadmahdi Sabahi, our clinical researcher for his help in collection of data.
Author contributions
Zohre Sadeghian: Data curation, Methodology, Software, Writing-Original draft, preparation.
Fatemeh Torkaman Asadi: Conceptualization, Visualization, Methodology, Editing, Supervision.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Trial registration
Not applicable. Our project is not a trial.