
Abstract
Objective:
This study aimed at verifying the outbreak, preventing further transmission, and identifying the risk factors for the outbreak.
Method:
A case–control study design was conducted from March 4, 2020 to April 30, 2020, in Kasoshekumer kebele of Sinana district. Thirty-seven carer–patient pairs and 74 controls were recruited in a 1:2 case–control ratio. Patients were selected using a national standard case definition of the Ministry of Health. Controls were selected from neighbors of patients and interviewed after the second incubation period from the last patient of the outbreak by a structured questionnaire similar to patients. All cases were included while controls were selected purposively for their exposure status. Vaccine efficacy, attack rate, and case fatality rate were conducted as a descriptive epidemiology. Multivariate analysis was used to identify associated factors.
Result:
Out of 109 study participants, there were 37 cases and 72 controls. The mean age was 58.8 months with ±54 standard deviation. Thirty-one (83.8%) of the cases had a known contact history and 23 (62.2%) were unvaccinated. The age-specific attack rate was 36/1000 in <5 years and 53/100,000 in >15 years. The estimated vaccine efficacy was 73.7%. Having any type of socialization behavior (adjusted odds ratio = 6.8, confidence interval: 4.25, 11.4), maternal poor knowledge of measles prevention (adjusted odds ratio = 4.152, confidence interval: 1.226, 8.058), and being unvaccinated (adjusted odds ratio = 7.79, confidence interval: 2.281, 12.63) were associated factors for measles infection.
Conclusion:
Poor knowledge of the parents on vaccination and the less effort taken to deliver good attitude toward vaccination are resulting in measles outbreak. However, herd immunity can prevent the outbreak; if not, the community will continue to suffer from mortality and morbidity. A resilient immunization program with sustainable and equitable supply, delivery, monitoring, and evaluation is a fundamental action in prevention of measles outbreak. Increased awareness of vaccination and other prevention measures are also crucial to end the outbreaks.
Introduction
Measles is an acute viral respiratory illness characterized by fever (up to 105°F), malaise, the three “Cs”—rhinitis (runny nose), cough, and conjunctivitis (red and watery eyes)—and a pathognomonic enanthem (head lice) followed by a maculopapular rash lasting at least 3 days. 1 The virus that causes measles is the measles virus (MV), which belongs to the genus Morbillivirus and the family Paramyxoviridae. MV is transmitted primarily by droplet infection over short distances and, less commonly, by aerosols suspended in the air for prolonged periods (2 h). The incubation period is 8–12 days from exposure to the appearance of the first symptoms. The rash usually appears 14 days after exposure. The disease is contagious for 4 days before and after the rash appears.2,3
MV is highly contagious with a baseline replication number(R0) of (12–18) in susceptible hosts, which depends on vaccination status, housing conditions, social contact patterns, social age distribution, birth cohort, and climate or season or area. 4 Only 3%–7% of susceptible persons were required for a measles outbreak. The secondary infection rate among susceptible household contacts is reported to be 75%–90%. The mortality rate for measles was estimated at 3%–5%, which was 3%–6% in Ethiopia but could increase to 10%–30% during outbreaks and in high-risk populations.5 –7
Currently available measles vaccines internationally are safe and effective, with one dose providing 85% immunity. The remaining 15% require additional doses to develop antibodies to measles. To develop herd immunity, vaccination coverage should exceed 95% in developing countries and 80% in developed countries. Transmission differs between age groups because antibodies are not always the same, and age may also affect contact patterns because school age differs from infancy in contact patterns.8,9
Increased global dissemination of the first and second doses of measles vaccine, combined with improved case-based surveillance, has led to a significant decline in measles incidence and the elimination of measles in the Americas. This progress led World Health Organization (WHO) to adopt the goal of eliminating measles by 2015. Since then, tremendous action has been taken to eliminate measles and reduce mortality, including timely investigation of and response to measles outbreaks as one of the most important measures of elimination. Efforts have contributed to a 75% decrease in reported measles incidence, a 79% decrease in mortality, and an estimated 20.3 million deaths avoided between 2000 and 2015.5,6
However, the effort had public health success; the elimination target by 2015 was not attained and America was the only WHO region to celebrate measles eradication by 2016. The celebration for the eradication was no more henceforth due to the reintroduction of measles transmission and massive outbreaks in America, Europe, Eastern Mediterranean, and South East Asia in 2017. The global measles case count increased by 48.1% between 2017 and 2018 again, and the number of reporting countries increased. In 2018, WHO estimated that there were approximately 10 million cases and 140,000 deaths worldwide due to measles outbreak. The number of measles cases reported in 2019 was the highest since 1992, with 89% of measles patients in America being unvaccinated or having no vaccination history.6,10
No vaccination and a tight community, such as the Jewish Orthodox Church in New York, accounted for 86% of the outbreaks. The other factor was stagnation of measles vaccination at 85%, which contributed to 20.8 million infants not receiving measles vaccine as part of routine immunizations and slowed progress toward elimination since 2010.11–15 From 2013 to 2018, there were 899,800 reported measles cases: 57% occurred in unvaccinated or inadequately vaccinated individuals and 30% had an unknown vaccination history. Low- and middle-income countries accounted for 66% of all cases. MCV1 vaccination coverage in Africa and the Eastern Mediterranean was estimated to be less than 60%, thus meeting the WHO target for measles elimination in 2019. 6
Ethiopia aims to achieve 80% basic immunization in the district, including measles vaccination through a primary health care unit consisting of five health posts and one health center for 25,000 inhabitants. Each health post serves 5000 residents. In addition to the fixed sites, the Ethiopian government has established a strategy for vaccination through outreach immunization sites, especially for hard-to-reach areas. Kasoshekumer is a rural kebele where life depends on agriculture. This rural kebele is accessible by car year-round and has a health center and health post. 16
According to the EDHS mini-report, in Ethiopia in 2019, only 44% of children aged 12–24 months received all basic vaccines, and 59% were vaccinated against measles despite the strategy. In Oromia region, where the study area is located, the primary immunization coverage including measles vaccine was 29.2%, which could be one of the factors contributing to the measles outbreak in different parts of the country. 17 The district’s official report on full vaccination coverage shows that the coverage rate in our study area was 100%, which was sufficient for the development of herd immunity to the MV. Therefore, information on vaccination coverage is limited because the official report on measles vaccination was made suspicious because of the outbreak. Therefore, we are interested in investigating the measles outbreak and determining the actual vaccination coverage and other risk factors that led to the outbreak.
This measles outbreak investigation is important to the district because it identifies risk factors for the outbreak so that the district can take steps to prevent it in the future. The results are also important in determining the vaccination coverage and impact of measles vaccination in the kebele, which provides a baseline for measuring vaccination coverage in the district and the kebele. Our goal was to verify the measles outbreak, prevent and contain further transmission and complications, and identify risk factors for the outbreak.
Methods and materials
Study area and period
Sinana is one of the districts of the Bale Zone in the regional state of Oromia in south-eastern Ethiopia. It is located about 450 km from Addis Ababa. There are 2 urban and 25 rural kebele in the district. Kasoshekumer is a rural kebele. According to the Central Statistical Authority, the population of the kebele is expected to be 8270 in 2020: 4053 (49%) are female, 1723 are households, 270 are under 1 year old (3.216%), and 3938 are under 15 years old (46.61%). Currently, there is one health post and two health extension workers in kebele. The study was conducted from March 4, 2020, to April 30, 2020.
Study design
To investigate the measles outbreak, we conducted a case–control study.
Population
Source population
All residents of Kasoshekumer kebele, Sinana district
Study population
Cases: All cases that met the standard case definition for measles cases at the beginning or onset of the outbreak, that is, from February 1 to the end of the study period on April 30, 2020, in Kasoshekumer, Sinana district.
Control group: All children under 15 years of age who did not meet the standard case definition for measles cases between February 1 and April 30, 2020, in Kasoshekumer, Sinana district.
Inclusion criteria
Cases: All cases that met the case definition of measles during the outbreak were included.
Controls: Children in the neighborhood who were younger than 15 years and had not developed measles symptoms during the period from February 1 to the second incubation period (42 days) after the last case.
Exclusion criteria
Cases that could not be reached by repeated visits and controls who were not in the area during the active outbreak were excluded.
Sample size
Of 42 cases, 37 cases and controls were included in a 1:2 ratio. Thus, 37 cases and 74 controls were considered the sample size, resulting in a total sample size of 111. This sample size was calculated using all cases, and for the controls, we applied the national public health emergency management (PHEM)guidelines and took two controls per case, since the study was an investigation of the outbreak. 18
Sampling technique
All cases were included as study subjects. Typical purposive control selection was used depending on similarity of exposure status. For each case, two controls were selected from the same household, neighboring households, and the school. Controls were generally non-randomly selected based on similarity of exposure status. Children with a high probability of being exposed had a greater chance of being selected as a control group. Thus, for school-aged children, we selected classmates if there were no children under 15 years of age in the family. If there were more than two susceptible control subjects in the family, sleepovers, and play situations were considered. Close family members, friends, and schoolmates were also considered in the selection of controls.
Data collection procedures and tools
The study was not a planned study, but an outbreak investigation study. We were part of the rapid response team (RRT) in the zonal health department of Bale and responded to this outbreak. In Ethiopia, every suspected case and confirmed surveillance case must be reported by a health facility or community to the district health office, then to the zonal office, then to the region, and finally to the Ministry of Health. After the Sinana Hospital notification was verified, the Sinana District Health Office and the Bale Zone Health Office declared the outbreak. Therefore, we started investigating the outbreak after the initial notification from the Sinana Hospital.
We used a structured questionnaire based on literature and guidelines for investigating measles outbreaks. Data were collected from the child’s parent during an active case that met the standard case definition of measles. Active surveillance was carried out to identify further cases in the residential home, school, and hospital, where isolation and treatment were carried out. The vast majority of cases were interviewed at an isolation center, while others were interviewed at home. The data collection tools for control were the same except that the clinical presentation and treatment sections were specific to each case. Control data were collected 42 days after the incubation period of the last case.
Quality assurance
The validated tools were revised following a review of various WHO articles and guidelines for investigating measles outbreak. 19 The field manager and mentor of the PHEM department reviewed the tools. Data collectors were trained in data collection and the use of data collection tools prior to the collection. Daily monitoring was performed during data collection by the principal investigator. The interview was conducted after parents were reassured of the purpose of the study, which was to minimize respondents’ bias of information; and to reduce interviewer bias, case and control interviews were conducted in the same manner and with the same tools. The completeness and integrity of the data were checked daily by the principal investigator during data collection.
Statistical analysis
Data were entered into a computer using Epidata software and checked for errors. For data exploration and analysis, data were exposed to SPSS version 21 statistical software. Before the analysis, data were checked for outliers, and missing values were displayed. A descriptive analysis was performed to describe the impact of the epidemic in terms of death rate, morbidity rate, and vaccine efficacy (VE = unvaccinated − vaccinated)/(unvaccinated). For calculating the infection rate, unvaccinated children under the age of 15 years who have never had measles are considered at risk. Since there has been no measles outbreak in kebele for a long time, active immunity is assumed to be zero. Vaccination was estimated from vaccinated controls: 38 of 72 controls (52%) were vaccinated. The population at risk was estimated by subtracting 52% of the not-at-risk target population (Table 2) from the total population of 8270 residents of Kasoshekumer kebele. Individual variables were described separately and summarized using univariate analysis. At p = 0.25, two-tailed logistic regression analysis was used to identify candidate variables for multivariate analysis. To control for confounding variables, multivariate binary logistic regression was used to obtain independent factors associated with measles cases. We used Wald’s inverse method to introduce the candidate variable. Significant outcome variables were selected as independent variables related to measles cases. The overall quality of the model was also tested using the Hosemer and Lemeshow model performance test. The adjusted odds ratio at a significant level of p < 0.05 was used as the association measure.
Result
Socio-demographic characteristics of participants
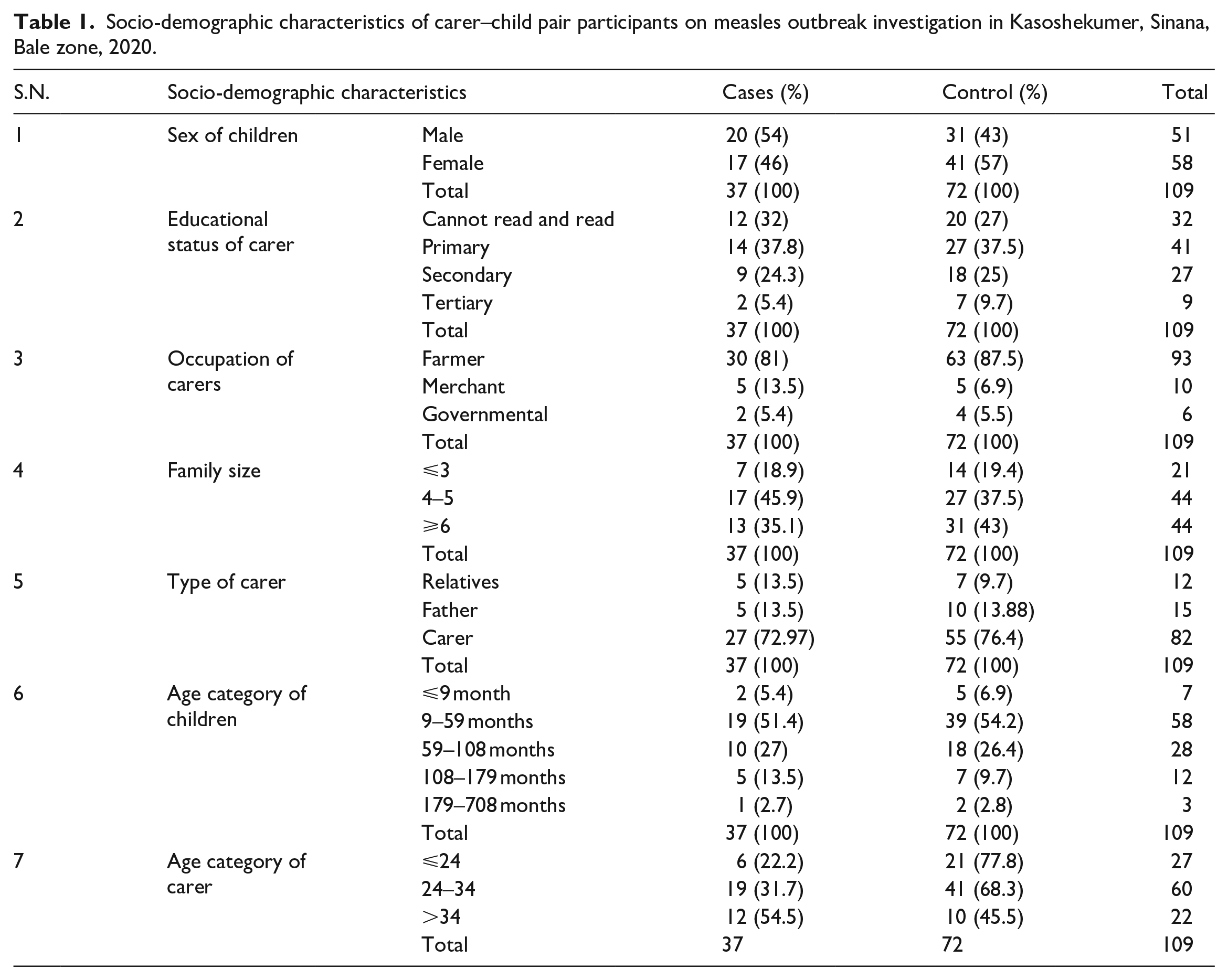
Of a sample size of 111, a total of 109 study participants were examined. The response rate was 98.2 %: 37 served as cases (20 men, 17 women) and 72 (31 men and 41 women) served as controls. The overall response rate was 98%. The mean age of the children was 58.8 with ±54 standard deviation (SD) (63.84, ±74 SD for cases) and (56.21, ±41 SD for controls) in months (Table 1). The mean age of parents was 29 years with ±6 SD. All respondents, 109 (100%), lived in rural areas; most of them, 93 (85%), were farmers, 10 (9%) were merchants, and 6 (5.5%) were government employees. Forty-one (37%) of our respondents or parents attended elementary school, 32 (29%) had never attended school or could not read and write, 27 (25%) attended secondary school, and only 9 (8%) had a diploma or higher education status. Forty-one (37.6%) had no vaccination status, 55 (50.4%) were vaccinated, and 13 (11.9%) had unknown measles vaccination status.
Socio-demographic characteristics of carer–child pair participants on measles outbreak investigation in Kasoshekumer, Sinana, Bale zone, 2020.
Descriptive epidemiology
Review of the outbreak
On March 2, 2020, a suspected case of measles was reported to the Sinana District Health Department by Robe Hospital. Through active case finding and community mobilization, additional cases were identified in the community and at the hospital. At that time, the index case was found and identified at the community level through intensified search. He had visited Dello Mena district 5 days before the onset of the rash. The zonal health department already had laboratory-confirmed case reports from Dollo Mena district. This index case was in contact with the confirmed case in Dollo Mena district. Therefore, the RRT verified the outbreak as epidemiologically linked to the confirmed case.
Description of measles cases by time
During the dry season from February 1, 2020, to March 14, 2020, 42 measles cases were detected in Kasoshekumera kebele in Sinana district. The last case was reported on March 14, 2020. The details of case description by time are shown in the measles epicurve (Figure 1).

Epicurve of measles outbreak.
Description of measles cases by location
The outbreak occurred in Kasoshekumer kebele in Sinana district. The area is 11 km from the city of Robe, and the population uses the hospital and health center in Robe for medical care. There is a health post in the kebele. The map shows the location of the kebele in Sinana district, Bale zone (Figure 2).

Map of Kasoshekumer kebele, Sinana district, Bale zone.
Description of measles cases by person
Of the total 37 cases studied, 31 (83.8%) had a history of contact with measles patients. Most of them at home and in the neighborhood (69%). Twenty (54%) of the cases were male. Children under the age of five were the most affected by this measles outbreak. Children aged 5–9 years were the second age group affected. Most cases, 23 (62.2%), had no vaccination history, while only 7 (18.9%) had a vaccination history, and the rest were unknown (Figure 3).

Vaccination status of measles outbreak cases in Kasoshekumer, Sinana, Bale, 2020.
Analytical epidemiology
Of the 16 variables recorded and analyzed by bivariate logistic regression to select candidate variables for multivariate analysis, only 6 were significant (p < 0.25) (Table 2).
Variables entered to bivariate logistic regression to select candidate variables.

Multivariate logistic regression analysis. CI: confidence interval; COR: crude odds ratio.
Candidate variables selected to be entered to multivariate analysis.
When the identified significant variables were entered into the multivariate logistic regression analysis, only three variables were found to be independently associated with the occurrence of measles. Thus, the odds of contracting measles were 11.9 times higher among children who had some socialization (time spent with other children outside the home, such as enrollment in school and playing with other children) than among children who had no socialization (adjusted odds ratio (AOR): 11.9, 95% confidence interval (CI) 3.5, 41.4). Children with parents who had poor prevention knowledge of measles were 3.69 times more likely to have measles than children with parents who had good prevention knowledge of measles (AOR: 3.69, 95% CI 1.156, 11.8). In addition, unvaccinated children were 6.8 times more likely to have a case of measles than vaccinated children (AOR: 6.8, 95% CI 2.281, 21.63) (Table 3).
Independently associated variables with measles case outbreak in Kasoshekumer kebele, Sinana district, Bale Zone, 2020.

AOR: adjusted odds ratio; CI: confidence interval.
Significantly associated variables.
Severity
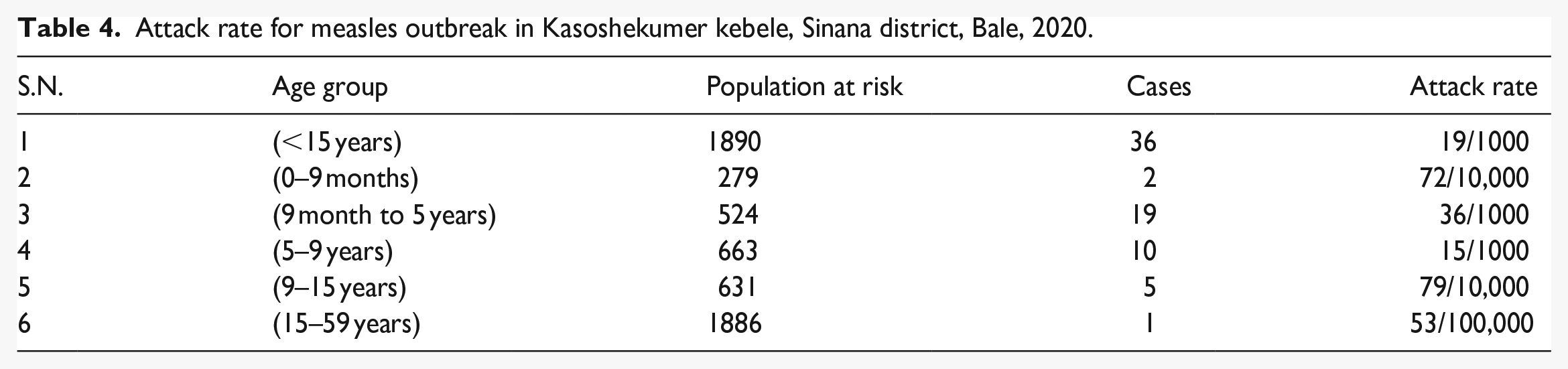
Almost all cases had the clinical picture of measles disease, mainly with rash and to a less extent conjunctivitis, as indicated (Figure 4). Of the 37 cases, 22 (59%) developed at least one complication, including diarrhea 17 (77%), ear infection 6 (27%), and seizures 5 (22%). Of the total number of cases, two died and the others recovered. Total case fatality rate (CFR) = 2/37 × 100 = 5.4%. Age-specific mortality rate can only be calculated for the age group of 9 months to 5 years and over 15 years, because there were only two deaths in each of these age groups. CFR (9 months to 5 years) = 1/23 × 100 = 4.3% and CFR (>15 years) = 1/1 × 100 = 100% (Table 4).

Percentage of clinical presentations manifested on total measles case of Kasoshekumer kebele, Sinana district, Bale zone, 2020.
Attack rate for measles outbreak in Kasoshekumer kebele, Sinana district, Bale, 2020.
Vaccine efficacy
The calculated efficacy of the vaccine was 73.7%. The coverage rate for the vaccinated at-risk population was calculated by reducing the percentage of unvaccinated children in the controls and extrapolating to the total number of children under 15 years of age in the 1890 kebele.
Responses and surveillance
Of the total cases studied, 29 (78.4%) visited a health facility on their own initiative, and a total of 31 (83.8%) received treatment at the health facility and outreach center. In the isolation ward of Robe Hospital, 16 (48.5%), 17 (51.1%), 21 (63.6%), and 26 (78.8%) were treated with ORS, antibiotics, vitamin A, TTC ointment, and antipyretic agents, respectively. During the mini-campaign, 235 (41.1%) of the at-risk kebele population were vaccinated and provided with vitamin A. Daily active surveillance was conducted by health extension workers and community leaders, as well as daily updates and analysis until 42 days after the last case was reported.
Discussion
As far as we know, cases occurred infrequently in persons over 15 years of age, with only one case resulting in death in our finding. Children under 9 months of age were also less frequently affected than persons over fifteen years of age. Of the 37 total cases, 22 (59%) had at least one common complication of measles. An overall mortality rate of 5.4% was found, 4.3% in those under 5 years of age and 100% in those over 15 years of age. The vaccine efficacy for a single measles vaccine dose was 73.7%, with the majority of cases (62.2%) having no vaccination history. Infection rates were high among children 9 months to 5 years of age (36/1000 infection rate), followed by children 5–9 years of age (15/10,000 infection rate). Variables independently associated with disease included lack of vaccination, socialization behaviors, and low parent knowledge of measles prevention.
Kasoshekumer kebele has dega weather and is located about 10 km from the city of Robe, which has a total population of 8270 people and 3938 (47.6%) children under 15. There is only one health post staffed by two health extension workers. The health post that included this kebele was more than 17 km away and passed through the town of Robe, making close monitoring and supervision difficult. In addition, the population in this kebele is very large compared to the number of health workers. There is only one health post with two health workers per population. This can result in insufficient health services for the entire population and missed vaccinations and other health services. However, transmission outbreaks were too slow and were stopped relatively quickly before spreading beyond these cases despite the inaccessibility of health facilities. This is most likely due to the relatively sparse population in this kebele compared to other kebele in Sinana district due to the uneven land surface, or the timely rigorous response of the district, health center, and health post most likely contributed to stopping the outbreak before it could spread beyond these cases.
The outbreak occurred during the dry season, a high-risk time of year as people increasingly move from the lowlands to the highlands in search of pasture. According to reports, measles outbreaks in tropical regions occur seasonally and peak during the dry season. This may be due to increased contact of schoolchildren with measles during the dry season. Increased contact in a crowded environment such as a school can lead to outbreaks of infectious diseases such as measles in endemic areas. Another reason for measles outbreaks during the dry season is population migration, especially in pastoral areas in search of grazing land. This is most likely true in our area, as the index case was from Dollo Mena district, where this type of migration is common during the dry season.20,21
The epidemiologic transition from measles in children younger than 5 years to measles in children older than 5 years has been reported in highly vaccinated areas as a result of vaccination of new birth cohorts. This is not supported by our results, which show a high age-specific rate of disease in children aged 9 months to 5 years. Studies such as ours have found a high prevalence of measles cases in children younger than 5 years, particularly in children aged 1–4 years. This suggests that the children in our study area had not been vaccinated for many years.15,22–25
CFR may vary from place to place depending on the underlying disease. For example, mortality rates for measles outbreaks in Konso, Southern Nations, Nationalities, and Peoples’ Region (SNNPR), and Somali region of Ethiopia were 7.8% and 1.2%, respectively, which is not consistent with our results.26,27 The higher mortality rate in Konso could be due to inaccessibility of health services or underlying disasters such as malnutrition and others. On the other hand, there were few outbreak deaths in Somali region, which could be due to better health care and timely outbreak response. Vaccination effectiveness was only 73.7%, while the standard vaccination coverage for measles is 85%. This deviation from the norm was also found in other studies.7,28,29 This is most likely due to inaccurate information about vaccination status, such as unknown vaccination status in our case.
Unvaccinated status, socialization behavior, and insufficient knowledge of parents about measles prevention were independently associated factors with measles infection. This was also demonstrated analytically, as the odds of contracting measles were 6.8 times higher in unvaccinated children than in vaccinated children (p = 0.001). The odds of contracting measles increased 11.9-fold (p = 0.001) if children had social contacts outside their homes compared with children who had no social contacts outside their homes. The odds of contracting measles were 3.69 times higher among children with poor knowledge of measles prevention than among children with good knowledge of prevention.
Recent studies of global trends in measles outbreaks show that even developed countries such as the United States are affected by a resurgence of measles. Several factors have been associated with the fatal outbreak; however, inadequate vaccination has been identified as the major risk factor.30,31 Many studies comparable to our study have found an association between measles cases and inadequate vaccination.32 –34 This suggests that one of the main risk factors for measles outbreak is inadequate vaccination coverage, which is an indicator of low vaccination coverage and inadequate herd immunity in the community.
Parents’ knowledge of how measles spreads and how to protect themselves might increase the likelihood that they will have their children vaccinated, or it might help to isolate and reduce contact and cover the mouth when coughing. Consistent with our findings, inadequate knowledge about transmission and prevention, particularly vaccination, has been associated with outbreaks in southeastern and southwestern Ethiopia.24,32,34 The U.S. study found that parents who knew about or were familiar with the outbreaks were more concerned about taking up vaccination and other preventive measures. This may be because sharing information and discussing vaccination with parents and other community members at meetings and at home is likely to result in more children receiving more vaccine doses.30,35
Socialization also increases the possibility of contact at play, school, or religious institutions. The number of contact and measles cases increases with socialization. Children younger than 9 months are less likely to get measles, according to our findings. This could be because infants experience little or no socialization outside the home and are not exposed in school, play, and other possible contact environments.
Strength
This survey provided information on the actual measles vaccination status of children. The survey was conducted in conjunction with the response, and all public health actions taken to interdict this outbreak were included in the report. Consideration of similar exposure status in cases and controls revealed a strong association between risk factors and cases. Other strengths included case management and follow-up, use of validated instruments, rigorous statistical analysis, and data collection by well-trained healthcare providers.
Limitation
To calculate the effectiveness of vaccines, the vaccine coverage of the area representing the population at risk is necessary, but we did not take the coverage because the full vaccine coverage of the district is 100%. Vaccine efficacy calculated in discovery was based on control coverage. The other limitation was that we used the measles investigation guideline to calculate sample size, and power for sample size was not analyzed as well as no sample size formula was used. Another limitation was that we used measles guidelines to calculate the sample size, and the power of the sample size calculation was not analyzed. Another limitation is that the vaccination status of the second primary vaccine was not considered and hence the need for another study. Recall bias may be also the limitation of this study as the study depends on retrospectively collected data of a case–control study.
The epidemic was also not laboratory confirmed; rather, it refers to epidemiologically linked to confirmed cases. In addition, a wide confidence interval was observed due to the small sample size and less analyzed sample power, which may also be due to a lack of resources to increase the sample size.
Conclusion
Ethiopia’s measles elimination strategy is not being implemented because efforts to maintain primary vaccination coverage above 80% are hampered by parents’ lack of vaccination and inadequate efforts by health providers to change vaccination attitudes. However, herd immunity is the first option to stop this deadly outbreak; if it is not achieved locally, the community will continue to suffer from mortality and morbidity.
Recommendation
A sustainable vaccination program is a key measure to prevent the outbreak of such a deadly disease through sustainable and equitable supply, delivery and program monitoring, and evaluation such as district, health center, and health station. Every effort should be made to increase awareness of vaccination and other preventive measures. Identification of missed vaccination opportunities should be done in collaboration with community leaders and health workers, and routine vaccination should be strengthened. It is also important to do more research on the basic status of childhood vaccination and related factors in the region rather than relying on the official vaccination report.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231169182 – Supplemental material for Measles outbreak investigation in Kasoshekumer kebele, Sinana district, South-Eastern Oromia, Ethiopia: A case–control study
Supplemental material, sj-docx-1-smo-10.1177_20503121231169182 for Measles outbreak investigation in Kasoshekumer kebele, Sinana district, South-Eastern Oromia, Ethiopia: A case–control study by Milkessa Mebrate, Cherinet Hailu and Soresa Alemu in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to extend our thanks to the Ethiopian Ministry of Health, ETFETP, and Jimma University for providing a conducive environment. Our thanks go to Mr. Naod Birhanu for his contribution in facilitation and supervising us during the study on the behalf of Ministry of Health.
Author contributions
MM is the principal investigator who was involved in idea generation, design, planning, and data analysis and interpretation. CH is the academic advisor who also participated in the design, analysis, and interpretation, participating in all stages of scientific writing. SA is a co-author who involved in the design, analysis, and editing of the article and critically reviewed it and gave final approval of the version to be published. All authors agree to be responsible for all aspects of the work.
Availability of data and materials
Data will be available upon the request of the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was conducted according to the Helsinki Slowdown Principles. Ethical approval was obtained from the Ethical Review Committee of Mettu Health Science College with reference number RF: 6675/ 21/2013. A letter of support was written by the Bale Zone Health Department to the Sinana district hospital, Sinana district, and Kasoshekumer rural kebele. We interviewed both case and control after obtaining verbal and written consent from the children’s legally authorized representatives. The consent was read to those who could not read, and both the subject and the representative signed it with a witness.
Informed consent
We interviewed after verbal and written consent was obtained from legally authorized representatives of the children among both cases and controls.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.