
Abstract
Introduction:
In 2019, we investigated the profile of the cases and controls and the determinants of pertussis transmission in Kebbi State, Northwestern Nigeria, to inform better immunization and surveillance strategies.
Methods:
Community-based unmatched case–control study and review of the 2019 pertussis routine surveillance data in the affected settlements in the state were conducted. A total of 52 suspected cases of pertussis and 107 control from two local government areas in Kebbi State were recruited. Data were analyzed using descriptive and inferential statistics.
Results:
The highest attack rate was observed among between 1- and 4-year age group followed by children less than 1-year old, and the least attack rate was among those above 15 years. The overall attack rate and the case fatality rate were 2.10% and 0.10%, respectively. A higher attack rate was observed among women, whereas the case fatality rate was more among males. From the community survey, we observed that the cases were less likely to have pertussis vaccination history (adjusted odds ratio = 0.28, 95% confidence interval = 0.11–0.74) compared with the controls. Knowing pertussis prevention methods were found protective for pertussis transmission (adjusted odds ratio = 0.14, 95% confidence interval = 0.04–0.45).
Conclusion:
This study showed the vulnerability of children under 5 years, especially under 1 year, to vaccine-preventable diseases in rural populations, where “real” immunization coverage is sub-optimal, and the dominant socio-demographic factors are supportive of disease transmission. We found immunization and knowledge of the preventive measures to be protective against pertussis outbreaks. Therefore, routine immunization services must be intensified to improve coverage and prevent future pertussis outbreak(s).
Introduction
Pertussis, also called whooping cough, is an acute, distressing, infectious disease caused by a gram-negative toxin-producing pleomorphic bacillus: Bordetella pertussis; and less commonly B. parapertussis. 1 This bacterial infection spreads from infected to susceptible hosts via airborne droplets and respiratory secretions. It runs a mild to a severe course through three stages: a catarrhal, a paroxysmal, and finally, a convalescent phase. As a hallmark of the disease, pertussis patients during the paroxysmal phase usually present with sudden and intense episodes of cough with or without a terminal whoop. Other symptoms and signs are post-tussive vomiting and cyanosis. 2
Despite having humans as the sole reservoir, this fastidious and highly contagious organism has caused outbreaks from the 17th century to date. Historically, pertussis showed a very high incidence rate, attack, and case fatality ratio with a preponderant affectation of under 5-year-old children. 1 In recent times, the advent of modern medicine has ushered in tremendous improvements in the indices mentioned above and an overall improvement in disease control. The public health strategies for the control of pertussis (whooping cough) are vaccination of susceptible individuals—especially children, enhanced surveillance, and case management following the detection of outbreaks. 2
With the support of the World Health Organization, the Nigerian Government launched the Expanded Program on Immunization (EPI) in 1974 to institutionalize the control of childhood killer diseases, including pertussis.3,4 Studies revealed that the introduction of the pertussis vaccine has contributed to a reduction in the incidence of the disease in modern times. However, the worldwide pertussis disease burden continues to be huge. Globally, estimates showed a cumulative of 24.1 million cases and 160,700 deaths in under 5-year-old children in the year 2014. 5 Sadly, the Nigerian pertussis data may not be reliable. 6
One of the major challenges in pertussis control, especially in developing countries, is the sub-optimal immunization coverage. The causes of the persistent sub-optimal immunization coverage are weak demand creation, vaccine hesitancy, poor microplanning, inadequate staffing, infrastructural gaps, difficult terrains, adverse events following immunization, and data quality errors.7–10 For instance, the national coverage for the pentavalent 3 vaccine (which offers protection against pertussis among others) in Nigeria was 33% in the year 2017 with differentially lower indices in many parts of the northern region. 11 The immunization gap was worsened by sub-optimal pertussis surveillance systems, surveillance data quality issues, and the shortage of diagnostic tools. 12 Furthermore, pertussis-protective antibody levels wane over time resulting in secondary vaccination failure.
In Kebbi State, there had been sporadic suspected outbreaks of pertussis, which were hitherto not thoroughly investigated either due to less prioritization of pertussis surveillance or due to numerous competing demands. Consequently, the authors conducted a full investigation into the suspected outbreaks of pertussis between the 14th and 42nd epidemiological weeks of 2019. Hence, this study reviewed pertussis outbreak data and assessed the factors associated with pertussis outbreaks to support better immunization and surveillance strategies in Kebbi State, Nigeria.
Methods
Study design
We conducted a community-based unmatched case–control study and reviewed the 2019 pertussis surveillance data in the affected settlements in Kebbi State.
Study setting
This study was carried out in Kebbi State of Northwest Nigeria. The State internationally borders with Niger and Benin Republics, and locally with Zamfara, Sokoto, and Niger States. Kebbi State consists of 21 local government areas (LGAs) that comprise 225 administrative wards, which are organized into four traditional emirates. This study was conducted in Tungan Noma and Gayi settlements of Kalgo LGA and Jelani and Kaiwa settlements of Argungu LGA. These settlements are essentially rural populations. There are 36 health facilities (HFs) in Kalgo LGA, where 28 HFs were providing routine immunization (RI) services. Likewise, among 46 HFs in Argungu LGA, 43 of them were offering RI services. From the 2019 RI report, the Penta 3 coverage was 124% and 94.6% in Argungu and Kalgo LGAs, respectively.
Regarding disease surveillance at the LGA level, all the HFs in the LGAs are expected to report notifiable disease via the integrated disease surveillance and response (IDSR) strategy every month. In Kalgo LGA, the timeliness and completeness of IDSR monthly reporting for the year 2019 were 72% and 78%, respectively, while Argungu LGA had the timeliness of 74% and completeness of 91%. These key performance indicators affect disease outbreak detection and response.
Figure 1 shows the map of Kebbi State indicating in red the LGAs where there were suspected outbreaks and those in green were without suspected pertussis outbreak in 2019.

Map of Kebbi State indicating in red the LGAs where there were suspected outbreaks and those in green were without suspected pertussis outbreak in 2019.
Case definitions
Suspected case: any person who has cough illness lasting at least 2 weeks with either paroxysm of coughing, inspiratory whoop, or post-tussive vomiting, without any other apparent cause. In this study, we do not have laboratory-confirmed pertussis, but we relied on the standard case definition as defined by the World Health Orgainzation (WHO). 5
Epidemics of pertussis: an increase of pertussis incidence or number of cases over the reported baseline in a specific geographic area.
Study sample and sampling
The sample size calculation was based on the two-population difference formula. With the assumption of at least 25% difference of exposure between the case and controls, 95% confidence interval, power of 80%, and ratio 1:2 were used in the formula, leading to 52 among the cases and 104 in the control group. During the study, the investigators selected 52 cases and 107 controls. The cases were selected from 277 suspected cases on the surveillance record (line list) using the lottery method. To select controls, the investigators obtained the list of households from an appropriate government agency, and the households were randomly selected. From each household selected, the youngest person was chosen as a control.
Data collection
This study had two parts: surveillance document review and community-based survey. The investigators reviewed the line list of all pertussis cases in the State. Three pertussis outbreaks were reported, one in Argungu LGA, and two in Kalgo LGA. The line list had the list of all suspected pertussis cases based on the WHO case definition. It also consisted of Epid number, name, settlement, ward, LGA, sex, age, date of onset, date of seen at HFs, date of specimen collection (if possible), laboratory result, admission status, and outcome of the disease (i.e. dead or alive). The LGA Disease Surveillance and Notification Officer generated the line list and transmitted to the State level (Epidemiology Unit) before the inception of the research.
The research questionnaire was adapted from a study conducted in Ethiopia. 13 The questionnaire was pre-tested and validated to fit the local context. Research Assistants were trained for 2 days on how to administer the questionnaire. The village head identified the cases and controls, and the head of each household was approached for verbal consent before being interviewed by the research assistants. The research assistant collected data face to face at a convenient time and place for the interviewee in November 2019. The confidentiality of the information collected was maintained. The principal investigator and co-investigator regularly checked the completeness and consistency of information gathered. The completed questionnaires were kept in a secure place for subsequent data entry.
Data management
All gathered information from the line list and questionnaires were converted into a soft copy on EpiData 3.1 using double entry. The data processing and analyses were done using R version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). Epicalc package was used for data management and analysis. 14
The date of onset and date seen by healthcare providers were obtained from the line list and presented in a graph. All reported pertussis cases from the line list were grouped according to the epidemiological calendar, counted as Week 1 in the first week of the year and continued chronologically. Specific attack rates by age and sex were calculated by dividing the number of pertussis cases by the total population exposed in specific settlements per 100. The case fatality rate was calculated by dividing the number of death due to pertussis outbreak by the total population exposed to the outbreak in specific settlements per 100.
Using community survey data, socio-demographic, immunization history, clinical features, and exposure status were illustrated in frequency and percentage. Bivariate analysis was done to select candidate variables with a cut point of p value < 0.25. Prototype-independent variables were put in multiple logistic regression, and then a backward stepwise technique was used to select the best-fitted model. Chi-square test was used for categorical variables, Fisher’s exact test was used for the categorical variables with small count. In contrast, Wilcoxon rank-sum test was used for the continuous variables to determine the association between dependent and independent variables. The effect size was presented in terms of the adjusted odds ratio (adj. OR) and 95% confidence interval (CI).
Ethical approval
Indeed, the field survey was conducted while investigating the pertussis outbreaks in the two affected LGAs. The investigators obtained a waiver from the State Research Ethics Committee with reference number—MOH/KSREC/VOL.I/56. The investigators adhered to the ethical principles of research as enshrined in the Helsinki declaration.
Results
There was a total of 277 suspected pertussis cases reported in 2019, 185 from Jelani and Kaiwa settlements of Argungu LGA and 92 from Gayi and Tungan Noma settlements of Kalgo LGA. There were 13 dead cases reported, all from Argungu LGA.
Of the total 159 study participants, the median age (interquantile range (IQR)) for cases was 36 months (24,53.8), and control was 27 months (15, 38.5). More than half of the study participants were female. The study participants were mostly farmers and Muslims by religion. More than half of the study participants’ parents attended Quranic school. The median (IQR) number of family member in the households for cases were 7 (4,13.2) and controls were 6 (4,10). The distance to the nearest HF from the households ranged from 1 to 5 km with a median of 3 (2,4) and 2 (1,3) for cases and control, respectively. The travel time to reach the nearest HF ranged from 5 to 35 minutes, with a median of 20 (15,22.8) for cases and 15 (10,20) for controls (Supplementary Table).
Two pertussis outbreaks were reported in Kalgo LGA in April and October 2019. Figure 2 showed that the date of onset and date seen by health professionals in Kalgo LGA were short, and the outbreak ceased within a short period. However, in Argungu LGA, the pertussis outbreak occurred between July and September 2019, characterized by late notification and higher number of cases.

Date of onset and date of pertussis cases seen by a health professional in the two LGAs of Kebbi State, Northwest Nigeria.
Figure 3 presents the breakdown of pertussis cases according to the epidemiological calendar of 2019. However, the graph showed weeks that there was at least a reported case. The highest number of pertussis cases were reported in weeks 35 and 36.

Number of pertussis cases reported by epidemiological calendar of 2019 in two LGA of Kebbi State, Northwest Nigeria.
The attack rate and case fatality rate of pertussis according to different age groups and sex can be seen in Table 1. As can be seen from the table, the highest attack rate was observed among the 1–4 years age group, followed by children <1 year. The least attack rate was noted in the age group above 15 years. The overall attack rate in the four settlements of the two LGAs studied was 2.10%, and the case fatality rate was 0.10%. All the deaths were recorded among age group of 1–4 years. Our finding showed that higher attack was observed among females, whereas the case fatality rate was more among males.
Attack rate and case fatality rate of pertussis outbreaks by age and sex in two LGAs of Kebbi State, Northwest Nigeria.

LGA: local government areas.
Note: The population is only for affected settlements not for the whole population of LGAs.
Data source: State pertussis surveillance data.
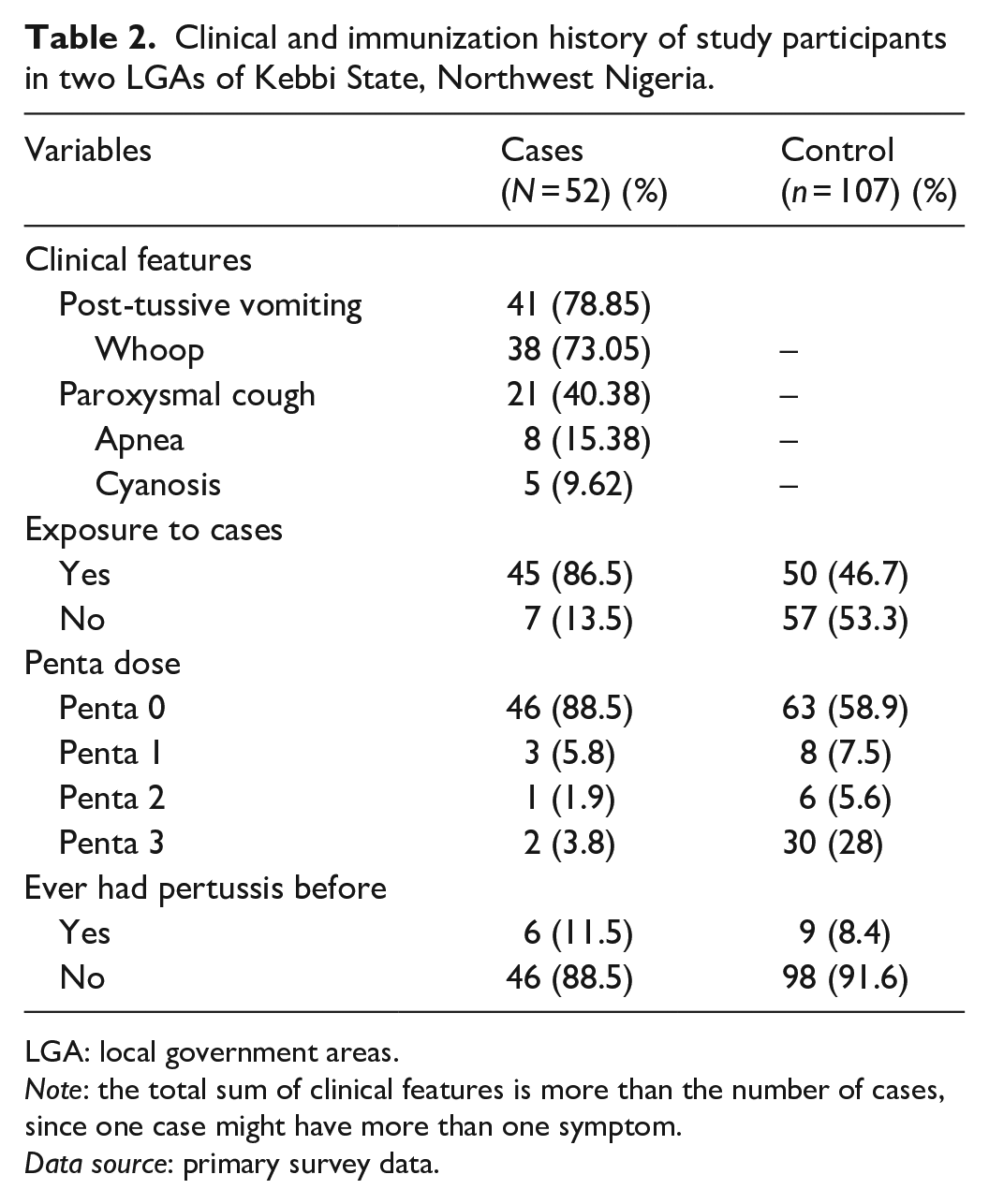
The clinical features, exposure status, and immunization history of study participants were presented in Table 2. Post-tussive vomiting was the most typical clinical feature of pertussis among cases, followed by whoop. Most of the cases and 46.7% of the controls had exposure to someone who has signs and symptoms of pertussis. Nearly 1 in 10 cases did not take the pentavalent vaccine, while 58.9% of controls did not receive vaccination for the pentavalent vaccine. Most of the cases and controls never had pertussis before.
Clinical and immunization history of study participants in two LGAs of Kebbi State, Northwest Nigeria.
LGA: local government areas.
Note: the total sum of clinical features is more than the number of cases, since one case might have more than one symptom.
Data source: primary survey data.
Table 3 shows factors associated with having pertussis during an outbreak. Having pertussis vaccination and knowing prevention methods of pertussis were found to be preventive against pertussis disease. The cases were less likely to have pertussis vaccination history (adj. OR = 0.28, 95% CI = 0.11–0.74) compared with the controls. Knowing pertussis prevention methods were found protective for pertussis transmission (adj. OR = 0.14, 95% CI = 0.04–0.45).
Factors associated with pertussis in two LGAs of Kebbi State, Northwest Nigeria.

LGA: local government areas; OR: odds ratio; Adj. OR: adjusted odds ration.
Statistical significance.
Data source: primary survey data.
Discussion
We investigated pertussis outbreaks in two LGAs in Kebbi State in 2019. In this study, we reported two waves of pertussis outbreaks in Kalgo LGA in different settlements but in the same political wards. In Argungu LGA, there was a single wave of the outbreak of pertussis in the two settlements, which spanned from July to September 2019. The key difference between the two LGAs was the long interval between onset of cases and notification of health services (intervention by primary health care authority). The delay in notification and response in Argungu LGA explained the longer duration of the epidemic and a higher number of clinical cases of pertussis.
We found that children between 1 and 4 years of age were most affected and had the highest attack rate, followed by <1 year. Individuals who were more than 15 years were the least affected. Our study finding was similar to the report from Kaltungo, Gombe State in the northeastern part of Nigeria, where the most affected age group was 1–4 years. 15 Kebbi State has a persistently low immunization uptake and coverage evident by survey data,11,16,17 and this could explain the recurrent outbreak of pertussis. The 2019 administrative coverage for the third dose of pentavalent vaccine in the two LGAs was more than 90%. The figures are, however, not reliable due to an underestimated denominator and data quality issues.7,8 The poor immunization data quality increasingly makes the use of survey data more valuable for critical decision-making and immunization performance review.
In this study, the female children were more affected and had a slightly higher attack rate than the males. In contrast, we found a higher case fatality rate in males than females. Similar to our study finding, studies from Ethiopia and Senegal showed a higher attack rate of pertussis among female children than male.12,13,18 The survey conducted in Gombe State, Nigeria, also found a higher incidence of pertussis among females. 15 Our study reported an overall higher attack rate of 2.1% compared to previous studies conducted in Ethiopia and northeastern Nigeria. The relatively higher attack rate may be related to the immunization uptake and coverage at household and community levels in Kebbi State and northwestern Nigeria. Regarding the overall case fatality rate, our study found a much lower case fatality rate than the previous studies conducted in Gombe State, Northeastern Nigeria, and Ethiopia.12,13,15 However, our study finding is comparable to a study published in 2009 from Argentina where case fatality rate was 0.17% based on analyzed outbreaks data. 19 Furthermore, we found a sex difference in case fatality rate, suggesting that males are more likely to die of pertussis when infected than females. However, this finding was different from a higher case fatality rate among females in Ethiopia. 13 The overall lower case fatality rate found in our study may be related to relatively early detection, investigation, and response to the outbreaks, wherein case management practices were instituted by local and state government health authorities to limit morbidity and mortality.
Regarding the symptomatology of pertussis during the investigated outbreak, the most common presentations were post-tussive vomiting (78.85%) and inspiratory whoop (73.05%). The least common symptoms in our study were apnoea and cyanosis. Almaw and Bizuneh, 2019, found a similar frequency of presentation of post-tussive vomiting and whoop. 12 Contrastingly, cyanosis was a relatively common presentation in Ethiopia compared to finding from our study. However, our result was somewhat like the Gombe study in the northeastern part of Nigeria, where 2% of the case had cyanosis. 15 The apparent difference in finding between the Nigerian studies and that of Ethiopia may be explained by a varying capacity to elicit the sign due to skin pigmentation and the health workers’ observational skills.
Examining the vaccination history of cases in our study, we found that 89% (roughly 9 out of 10) of cases did not receive any pentavalent vaccine dose. In comparison, only 4% of the cases received full dose (Penta 3) of pentavalent vaccine. The vaccination uptake among cases in our study is much lower than reported vaccination status in studies from Gombe State, Nigeria, where 42% of the cases received the third pentavalent vaccine. 15 This study from Ethiopia by Almaw et al. 13 2017 also reported 51% uptake among cases for the three doses of the pentavalent vaccine. The common denominator in all these studies is the sub-optimal RI against pertussis, which explained the occurrence of outbreaks in the study settings.
Concerning disease transmission and control strategy, we found a higher percentage of cases who had exposure to the infected individual(s), suggesting the high infectivity of pertussis and possibly the effectiveness of human-to-human transmission. We found that positive vaccination history and knowledge of the preventive measures were protective against pertussis even after statistical adjustment. In other words, cases are less likely to have pertussis if they were vaccinated and knew the preventive measures, such as vaccination, isolation treatment (case management) of infected individuals. Our result is not different from previous studies that reported the protective effect of full vaccination against pertussis.13,15
The socio-demographic data provided information about the possible root causes of poor vaccination coverage within our study setting. Vaccination uptake was differentially lower among the cases who are in the lower socio-economic class. As reported from the survey finding, the low level of education of both parents, rural sociology, including large family (household) size and modestly far distance to the HF might explain the poor health-protective behaviors (i.e. uptake of immunization services) and quality of parental care. Consequently, the unfavorable social circumstances could increase the children’s vulnerability to vaccine-preventable diseases. Similar findings have been documented by other authors who found maternal education, age, wealth, ethnicity, and distance to HF positively associated with vaccination uptake. 16
Our study might have benefited from a much larger sample size. However, we generated the data from a modestly representative sample from the communities that experienced pertussis outbreaks in Kebbi State. We were limited by the number of variables as captured in the State routine surveillance data for pertussis. Despite this limitation, the available data was able to answer our research questions. The study could have also benefited from laboratory support for the confirmation of pertussis but there was no state or a regional laboratory designated to confirm pertussis cases. Instead, we made use of clinical and standard case definition as recommended by WHO for field investigation and review of records. Finally, recall bias may also be a limitation to our study as the community survey took place 2 months after the onset of the index case.
Conclusion
Our study showed the vulnerability of children under 5 years, especially the under 1 year, to vaccine-preventable diseases in rural population and disadvantaged populations, where real immunization coverage remains sub-optimal, and the dominant socio-demographic factors are supportive of disease transmission. We also concluded that immunization uptake and knowledge of the preventive measures are protective against pertussis outbreak. Therefore, RI services must be intensified to effectively improve coverage and prevent future pertussis outbreak(s). Our study finding reinforced the imperative of a prompt case detection, reporting, investigation, and response in reducing the magnitude of the infectious diseases outbreak.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211008344 – Supplemental material for An epidemiological investigation of the 2019 suspected pertussis outbreak in northwestern Nigeria
Supplemental material, sj-pdf-1-smo-10.1177_20503121211008344 for An epidemiological investigation of the 2019 suspected pertussis outbreak in northwestern Nigeria by Omoleke Semeeh, Biniam Getachew, Yusuf Taofik, Lukman Surajudeen, Assad Hassan and Bello Nagudale in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121211008344 – Supplemental material for An epidemiological investigation of the 2019 suspected pertussis outbreak in northwestern Nigeria
Supplemental material, sj-pdf-2-smo-10.1177_20503121211008344 for An epidemiological investigation of the 2019 suspected pertussis outbreak in northwestern Nigeria by Omoleke Semeeh, Biniam Getachew, Yusuf Taofik, Lukman Surajudeen, Assad Hassan and Bello Nagudale in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledged the local government area disease surveillance officers, health workers, and the community leaders who supported the reactive vaccination in the two local government areas.
Authors contributions
S.A.O. conceptualized the study, participated in the study design, participated in manuscript writing, and critically reviewed all the drafts. B.G. designed the study, supervised data collection, conducted data analysis, and participated in the manuscript writing. T.A.Y. supported data collection and participated in the writing of the study. L.A.S. supported collation and analyses. B.N. and H.A. supported data collection and resource mobilization. All authors read and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.