
Abstract
Objective:
The increased prevalence of leftover medicines in the community is currently a global concern due to the detrimental effects on the environment and health. However, several developing countries have failed to give sufficient consideration to the issue. The primary purpose of this study was to describe the prevalence of leftover medicines, disposal practices, and the factors affecting those in households in Arba Minch Town, Southern Ethiopia.
Methods:
A community-based, descriptive cross-sectional study was conducted among households in Bere Edigetber and Nech Sar of Arba Minch town, from June 25 to August 27, 2022. Data were gathered through face-to-face interviews with revalidated structured questionnaires. A multistage sampling technique was utilized to select each household.
Results:
Three hundred forty-eight households agreed to participate in a study, resulting in a 94.8% response rate. Of the study participant, 172 (49.4%) of the households had leftover medicines, with antibiotics being the most common (64% of 172). Subsidy of symptoms and saving for later use were two frequently cited reasons for the presence of leftover medicines in the house. Throwing leftover medicines in household garbage was the preferred method of disposal (>60%). Only 0.1% of respondents considered returning leftover medicines to healthcare facilities or professionals. A binary regression analysis identified four predictors for having leftover medicines. Medicines obtained without prescription were the strongest predictor (odds ratio = 3.7; p < 0.001), followed by higher family monthly income (odds ratio = 2.5; p = 0.005), those waived paying for medicine (odds ratio = 0.294; p = 0.049), and those used medications for acute diseases (p = 0.048; odds ratio = 0.450). Respondents who had prior information on safe medicine disposal were 2.3 (p = 0.04) more likely to dispose of possessed leftover medicines rather than keep them for future use.
Conclusions:
This study revealed a high prevalence of leftover medicines and their improper disposal in Arba Minch town. The preferred methods of leftover medicine disposal in this study deviate from conventional standards. Significant factor variables that predict having leftover medicines are attributed to purchasing medicine without a prescription, higher family monthly income, those waived paying for medicine, and those who used medications for acute diseases. Prior knowledge of proper disposal practices predicated the decision to dispose of on-hand leftover medicines or keep them for future use. These findings would be critical in developing strategies to reduce leftover medicines and promote proper disposal practices.
Introduction
A large number of pharmaceuticals and healthcare supplies are used each year to diagnose, treat, or prevent medical conditions. This exponentially augmented by the ever-expanding drug market, newer pharmaceuticals, and growing use of both prescription and over-the-counter (OTC) medications contribute to the existence of a wide range of pharmaceuticals in the community. However, not all pharmaceuticals provided to patients are utilized, and as a result, large amounts are wasted or expire.1,2 Thus, according to the World Health Organization (WHO) information, more than half of all medicines are improperly prescribed and supplied, resulting in unnecessary medicine storage and posing a significant environmental hazard. 3 Prolonged exposure to medicines found in the environment could be hazardous for humans (particularly vulnerable groups such as pregnant women, newborns, and children), the environment, and wildlife. 2 For example, the nonsteroidal anti-inflammatory drug diclofenac has been found to cause kidney failure in vultures after they consume carrion from pretreated cattle in Pakistan. 4 Furthermore, several studies have revealed that medicine in the environment causes antibiotic resistance, adverse effects, inadvertent poisoning, drug abuse, and increased healthcare cost.5,6 Patients may not take the full prescribed dose of medicine for various reasons, including side effects, dosage adjustments, feeling better quickly, approaching expiration dates, marketing, doctor’s advice, and suggestions from family or friends.7–9 Interestingly, the WHO reported that 50% of patients do not take their medicines appropriately. 3 Therefore, it is common for households and patients to possess leftover medicines (LOMs) such as unused or expired medicines, and the risks associated with this have gained attention globally. 9
Although there are international standards for disposing of pharmaceutical waste properly, they have not been adequately adopted for use by the general public. As a result, numerous studies have revealed that improper medicine disposal practices and a lack of awareness are widespread global issues. For example, in India, 70% of surveyed undergraduate students have had an average of five expired medicines at home and preferred to dispose of them through household trash. 10 Studies conducted in Ethiopia, Kenya, and Nigeria indicated that putting LOMs in a latrine and throwing them in the trash are the two most common methods of disposing of them.5,8,11
Most developed countries have a national program for managing medicine waste due to concerns about improper disposal practices. For instance, a project for managing pharmaceutical waste and a take-back system exists in Australia, Canada, Sweden, and the United Kingdom. 7 However, in developing countries such as Ethiopia, 8 inadequate pharmaceutical waste management is a result of a lack of resources and a failure to implement legislative policies and regulations. Policies governing medicine disposal must be strengthened, particularly in developing countries. Furthermore, awareness campaigns and various practical strategies are required to dispose of LOMs. Therefore, determining the public’s level of understanding and attitude about the disposal of LOMs is critical. Additionally, information on widely used medicine disposal techniques would help in raising awareness about the safe disposal of LOMs. However, limited comparable studies are carried out in Ethiopia, and to the best of our knowledge, no study has been conducted about the methods used by households to dispose of leftover (unused and expired) medicines in the Gamo Zone. Therefore, this study aimed to assess the current prevalence, public disposal practices, and associated factors toward LOMs in Arba Minch town, Southern Ethiopia.
Methods
Study design, period, and area
A community-based, descriptive cross-sectional study was conducted in Arba Minch town, the capital of Gamo Zone, through face-to-face interviews using revalidated structured questionnaires from June 25 to August 27, 2022. Arba Minch is located in the southern nation nationalities and people regional state of Ethiopia, which is 505 km far from Addis Ababa. According to 2021 estimates, the total population of the town was 192,043, with six kebele administrations. 12 During the study period, the town has one general hospital, primary hospital, and health center that provide healthcare services to the population.
Study population
The study population was all households of selected kebele-land and comprised one participant from each house in the selected kebele who was available during the study period.
Eligibility
Residents of Bere Edigetber and Nech Sar Kebeles who were at least 18 years old, capable of communicating, free of cognitive disorders, willing to participate, and who had lived in Arba Minch town for at least 6 months were included in the study.
Sample size determination and sampling technique
The sample size was calculated using the single proportion population formula, with a p-value of 50%, a margin of error of 5%, and a confidence interval (CI) of 95%. Moreover, a multistage sampling technique was used to select households. First, Bere Edigetber and Nech Sar were selected from all kebeles (six kebeles) of Arba Minch town using a simple random sampling technique. Only two of the kebeles in the town were included because of financial constraints. According to the two selected administrative offices of the kebeles, there were 1253 and 1,197 households in Bere Edigetber and Nech Sar Kebele, respectively, for a total of 2450 households, which is <10,000. Therefore, considering the correction formula and non-respondents, a total of 365 households were surveyed. The total sample size was proportionally split to each kebele based on the total number of households of each kebele. Hence, 187 and 178 households in Bere Edigetber and Nech Sar Kebele were surveyed, respectively. Secondly, the study subjects (households) were selected using a systematic sampling technique. The sampling interval was calculated by dividing 2450 by 365; hence, every seven households were selected for the survey. The nearest household to the kebele administration office served as the reference household for the sampling interval.
Participants in the study were purposefully chosen based on their presence during data gathering, role, and responsibility. Thus, considering that mothers in Ethiopia are typically in charge of household management, mothers in each household were prioritized as study samples. The father would take precedence if the mother was not eligible. However, if neither is qualified, any household member who satisfies the requirements of the study was included.
If a household or an individual was not qualified or willing to volunteer, the next closest household or individual has been considered.
Data collection instrument and procedure
Data was collected through face-to-face interviews using revalidated structured questionnaires that were adapted from previously published studies (Supplemental file 1) and modified to suit the study purpose.5,8,13 The questionnaire was also uploaded to the Kobo Toolbox, which collects field data on mobile devices, tablets, and any browsers. 14 This tool was used to ensure data quality and track the global positioning system (GPS) of each surveyed household and capture images of LOMs during data collection. The questionnaires were developed in the English language and included all pertinent variables under the study objectives. It was divided into four subclasses intended to cover the sociodemographic characteristics, knowledge, attitude, and practice of respondents regarding the disposal of unused and expired medicines. The interview was translated to and conducted in Amharic language. We have discussed with the health extension workers, who have detailed information about each household in their respective kebeles, particularly, about the days when the majority of household members are available at home. The weekend (Saturday all day and Sunday afternoon) was then chosen as a convenient time for data collection. Four well-trained graduating class pharmacy students collected data on both hardcopy and smartphone.
Data quality control
The data collectors received 1 day of training on data collection tools, how to approach respondents, and other specific procedures. After the questionnaire was prepared, verification was done for checking the accuracy and validity of the questionnaire. The final English version of the questionnaires was translated by the research team, all of whom are fluent Amharic language speakers. The translation was performed by considering the conceptual comparability of each query and local context. It was then back-translated by purposefully invited independent translators to ensure consistency. Additionally, a pretest was performed on 5% of the sample size, and necessary modifications were made. GPS was recorded for each surveyed household. The data were verified for completeness and crosschecked with the data on the kobo toolbox before data processing and analysis. The data was password-protected on the computer and was only shared with the research team.
Study variables
The dependent variables in this study were “having LOM,” “planning on the existing LOMs,” and “presence of LOM-specific storage place in the house.” The second and third variables are purposely selected to identify associated factors concerning disposal practice.5,8,11 According to the current study context, having LOM was defined as possessing all medicines (prescription and OTC) that have not been completely consumed, have expired, or are no longer needed for the original medical condition.9,15 Since all dependent variables were binary, we coded them as follows: status of LOM was coded 0 = “No” and 1 = “Yes,” plan on existing LOM was coded 0 = “To store with/no reason” and 1 = “To dispose,” and presence of storage place in the house was coded 0 = “No” and 1 = “Yes” responses.
The independent variables that determine the prevalence of LOMs were selected on the theoretical basis of similar studies.5,8,9,11 Sociodemographic characteristics such as age, marital status, educational level, employment status, number of family members, and monthly income level were identified as independent variables. Furthermore, household health status and medicine use patterns, such as how medicine is obtained, the information provided on disposal methods, length of prescribing on a single visit, and the existence of chronic diseases, were covariates. Lastly, variables assessing knowledge and attitude toward LOM disposal were also included as covariates.
Statistical analysis
All returned questionnaires were checked for accuracy. Then the cleaned data was transferred to and analyzed by statistical package for social science software. Participant sociodemographic characteristics, knowledge, attitude, and disposal practice for the LOM were summarized by simple descriptive statistics (such as frequency and percentages presented by tables and figures). A binary logistic regression model was also used to examine the relationship between the prevalence of LOMs and the explanatory variables. A statistically significant association was declared when the p-value was 0.05 at a 95% CI. The 95% CIs and odds ratio (OR) were also calculated for selected variables. The Hosmer–Lemeshow goodness-of-fit test was performed for the regression model.
Results
Sociodemographic characteristics
Among the approached 367 individuals, 348 agreed to participate in the study giving a 94.8% response rate. Of the total respondents, 224 (64.4%) were female, 278 (80%) were above the age of 24, and 262 (75.3%) were married. The average household size was five people with a range of 1–25. Thus, 89 (25.5%) of the participants had completed primary school or less, 168 (48.3%) had completed tertiary education, and the majority (n = 152; 43.7%) were government employees. The average monthly income of respondents was 7568.94 Ethiopian Birrs (ETB) (144.5 US Dollars (USD)), ranging from 62,000 to 100 ETB (1183.2 to 1.9 USD) (Table 1).
Sociodemographic characteristics of the respondents; N = 348.

The exchange rate of USD to ETB in August 2022 was 1 USD = 52.4 ETB. ETB: Ethiopian Birr; USD: US Dollar.
World Health Organization’s scale classification of income level for developing countries.
Household health status and medicine use pattern
One hundred ninety-four (55.8%) of the households stated that they could receive a prescription for medicine more than four times per year (Table 2). A family member with a chronic illness who required regular medication was present in 82 (23.6%) of the households, and the two most prevalent conditions were diabetes mellitus (30.7%) and hypertension (23.4%). The majority of respondents (n = 67; 81.9%) stated that their/patient’s doctor prescribes medications for chronic conditions for no more than a month per visit. Out-of-pocket (OOP) payment is the main method of obtaining medicines for 276 (79.3%) households. 210 (60.3%) of households had a history of purchasing medicines without a prescription (physician order), with painkillers (55.5%) being the most commonly purchased medicine group, followed by other OTC medicines (17.5%). Likewise, 23 (6.6%) households have obtained medication for chronic disease without a prescription.
Health status and medicine use pattern among households in Arba Minch Town, 2022.
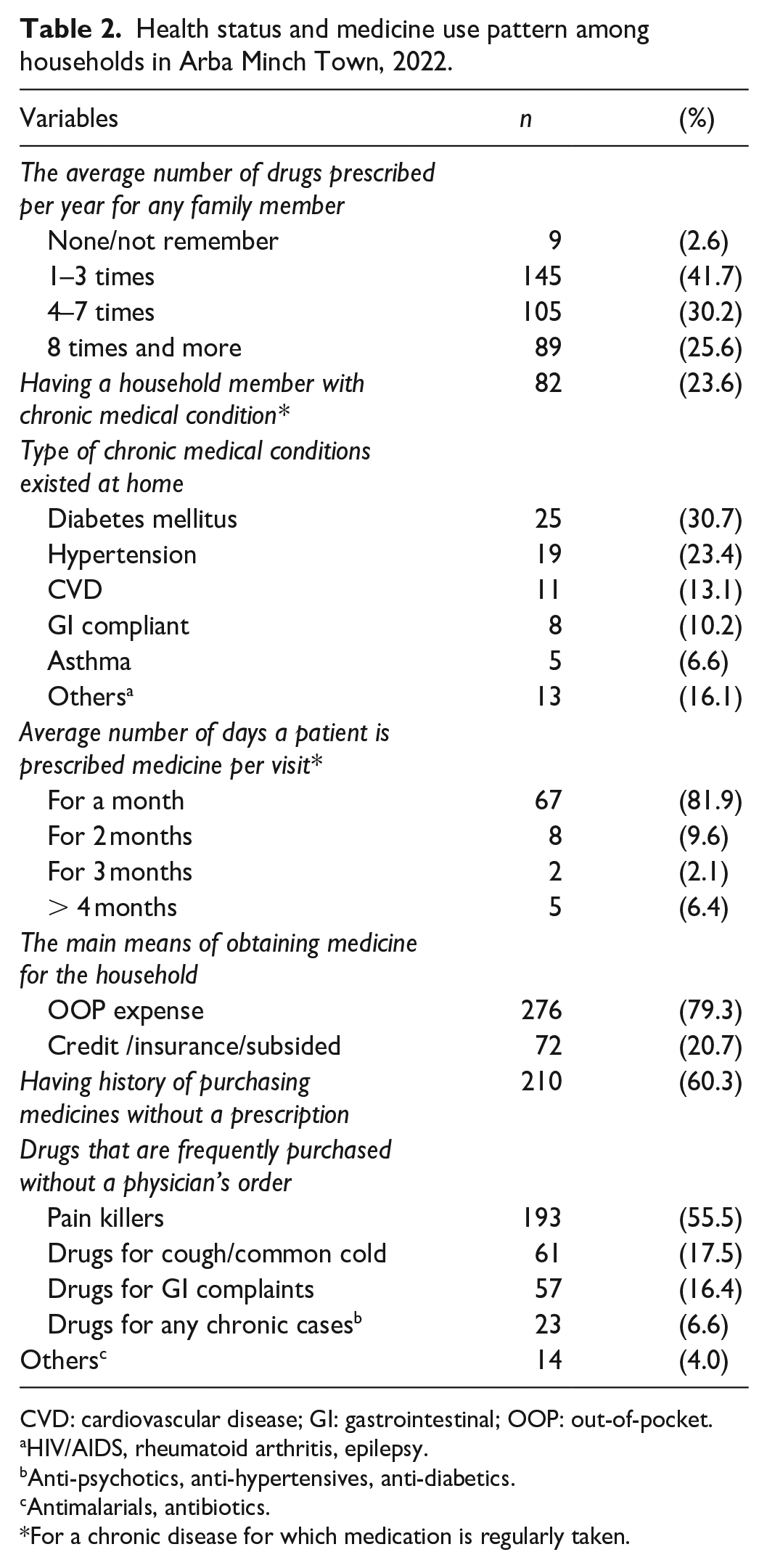
CVD: cardiovascular disease; GI: gastrointestinal; OOP: out-of-pocket.
HIV/AIDS, rheumatoid arthritis, epilepsy.
Anti-psychotics, anti-hypertensives, anti-diabetics.
Antimalarials, antibiotics.
For a chronic disease for which medication is regularly taken.
Prevalence and disposal practice of LOMs
As presented in Table 3 and Figure 1(a), 172 (49.4%) of the households had LOMs during data collection, with antibiotics (64% of 172) as the most prevalent class, respectively. The majority of (n = 91; 26.1%) observed LOMs were obtained without a prescription. The two frequent reasons given by the respondent for the presence of current LOM were “because symptoms had subsided (feeling better)” and “saving for later use” (Figure 1(b)). The most common practice of disposing of LOMs (expired and unused) was to throw them in the garbage (n = 240; 69% for expired; and n = 213; 61.2% for unused) followed by putting them in a latrine (n = 148; 42.5% for expired; and n = 116; 33.3% for unused). Only 0.1% of respondents considered to have returned it to any medical center or healthcare professionals. The majority of households (n = 298; 85.6%) had specified where the LOM was stored. The majority (95/172) of the households with LOMs planned to store it for various reasons, such as to share, reuse, or to be uncertain but store it.
Disposal practice of LOMs among households in Arba Minch Town, 2022.

HCF: healthcare facility; HH: household; LOM: leftover medicine.
Cupboard, drawer, table, and plastic bag.
Burn, landfill.
Share, store for future use, store but left undecided.
Based on experience.
Pearson chi-square.

LOM types and reasons for their existence in the household in Arba Minch Town, 2022. (a) LOMs observed at hospital and (b) respondent reasons for LOMs in the household.
Knowledge and attitude toward LOM disposal
Of the total, 279 (80.2%) of the respondents had no prior knowledge of how to dispose of medicines. For those with prior knowledge, pharmacy personnel was the most informative about safe medicine disposal. More than half of (n = 208; 59.7%) respondents consider expired medicines to be waste. The majority of participants (n = 262; 75.3%) stated that they always check the expiry date of medicines before buying or taking them. The majority of respondents (n = 337; 96.8%) believe that improper unused/expired medicine disposal can be harmful. Thus, 239 (68.7%), 150 (43.1%), and 341 (97.9%) of the participants noted that improper medicine disposal might harm the environment, kill wildlife, and result in children accidentally swallowing medication, respectively. 82 (24.3%) and 80 (23.7%) of respondents suggested that pharmacy staff and health extension workers should be the responsible bodies to create awareness about the proper disposal of unused medications, respectively. The majority of 225 (64.7%) respondents believe that their current disposal practice was appropriate (Table 4).
Knowledge and attitudes of respondents on the disposal of LOMs in Arba Minch Town, 2022.

LOM: leftover medicine.
Pharmacist, druggist, and pharmacy technician.
Health extension workers.
Factors associated with having LOM and its disposal practice
Tables 5 and 6 summarized the estimated effect of covariates on the prevalence of LOMs and disposal practices among households. The binary logistic regression model explained 11.2% of the variance of confidence (Cox and Snell R2) and 17.7% (Nagelkerke R2), with an overall percentage of cases correctly predicted of 80.7%.
Binary logistic regression analysis on the factors associated with prevalence of currently LOMs among households in Arba Minch Town, 2022; N = 348.
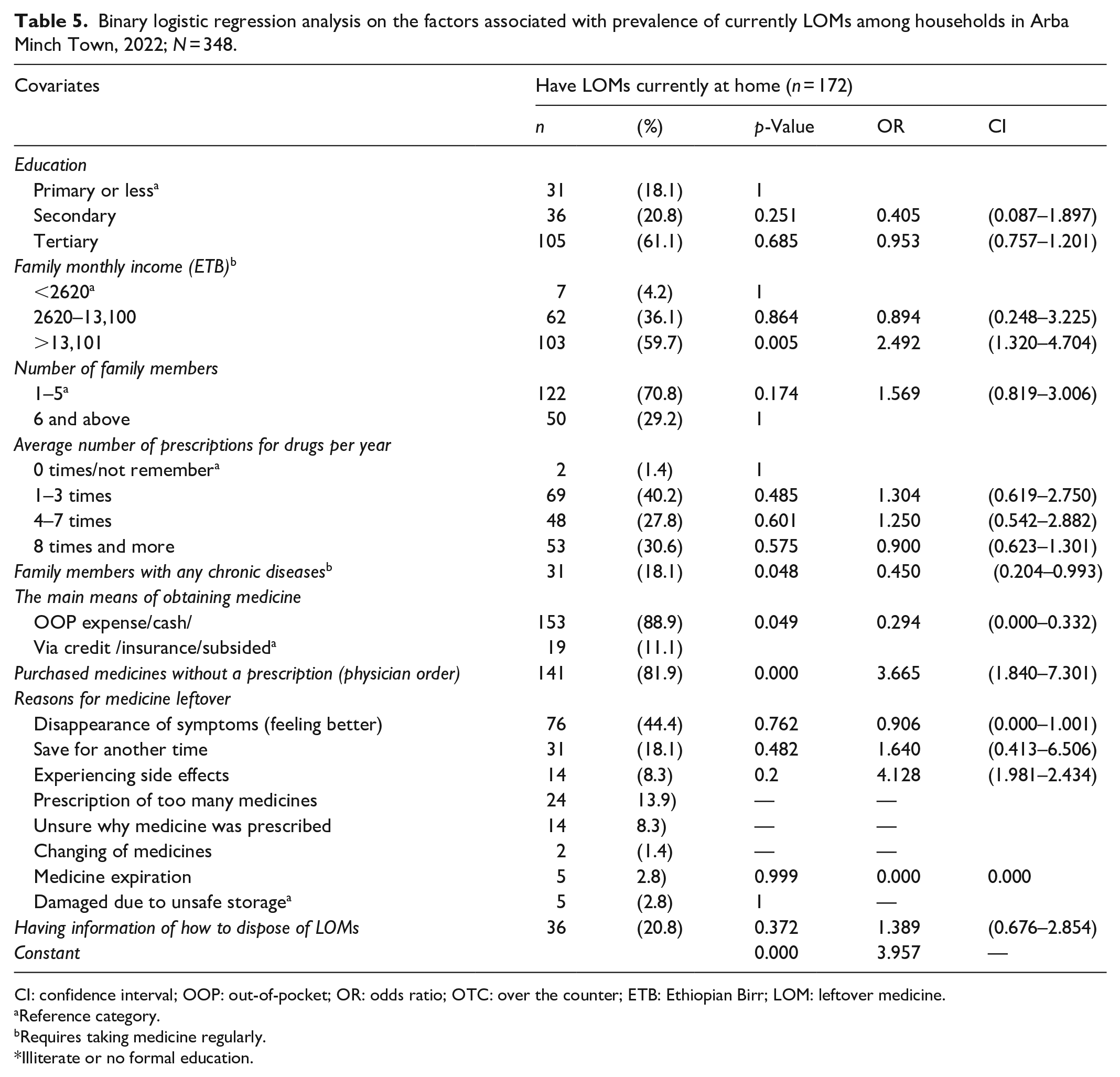
CI: confidence interval; OOP: out-of-pocket; OR: odds ratio; OTC: over the counter; ETB: Ethiopian Birr; LOM: leftover medicine.
Reference category.
Requires taking medicine regularly.
Illiterate or no formal education.
Binary logistic regression analysis on factors associated with the disposal practice of LOMs among households in Arba Minch Town, 2022.

CI: confidence interval; OR: odds ratio; OOP: out-of-pocket; SE: standard error; LOM: leftover medicine.
Reference category for education: none; ever purchased medicine without prescription: no; informed about medicine disposal: no; consider safe disposal: no; perceived risk to environment or health: no; type of current LOM: both.
Having LOM at home had a statistically significant association with four independent covariates in the regression model (Table 5). The strongest variable that predicted whether a household has LOMs was purchasing medicine without a prescription. The odds of having LOMs purchased without a prescription were 3.7 (p < 0.001) times higher than LOM obtained on a prescription. The other significant predictor was the family’s monthly income. The odds of having LOMs for households whose average monthly income of >13,100 ETB (240 USD) were 2.5 (p = 0.005) times higher than in households with an income of <2620 ETB (50 USD). The need of paying OOP for getting medicine was another significant variable. Households that waived paying for medicine were 70.6% more likely to have LOM than OOP payers (p = 0.049; OR = 0.294). The fourth significant variable was whether the household had a member with chronic illness or not. Households with no person who requires regular medication were 55% more likely to have LOM than households with such chronic illness (p = 0.048; OR = 0.450). The odds of having LOM were 1.4 (p = 0.372) higher for respondents who had no information about proper LOM disposal than for those who did.
Concerning the factors associated with the disposal practice of LOMs, independent variables “planning on the existing LOMs,” and “presence of LOM-specific storage place in the house” were statistically associated with prior information on safe medicine disposal and educational status, respectively (Table 6). The odds of planning to dispose of the existing LOMs for a respondent who had information regarding proper deposing LOM were 2.3 (p = 0.04) times higher than those planned to store for future use. The odds of having a designated place of storage for LOM at home for a respondent who completed tertiary education were 3.7 (p = 0.048) times higher than for those with primary education or less. Interestingly, even though significance was not detected, perceiving the environmental risk of LOMs strongly predicted whether the LOM has to be disposed of or stored for any reason. Those who perceived the environmental risk of LOMs were 38.2 times more likely to plan to dispose of them than those who did not recognize the harm.
Discussion
This study demonstrates the prevalence, disposal practices, and associated factors of LOMs, which may assist in providing its significance and raising awareness among the Arba Minch town public to reduce medication waste and harm.
The present study revealed that almost half (49.4%) of surveyed households had LOM in their house. Studies in Ethiopia revealed, 89 and 66% of participants had LOMs in Gondar and Harar, respectively.8,16 The higher prevalence in Ethiopia could be attributed to the absence of an established drug-take-back system in Ethiopia, including the current study area. 8 In comparison to the current study, the prevalence was higher in Ghana (98%), China (86%), Gujarat-India (68%), and Afghanistan (95%).13,15,17, 18 However, our figure was slightly higher than the Servian study (44.4%). 19 This disparity could be attributed to differences in information about rational prescription and medication adherence, as well as levels of concern and implemented measurements across countries. However, the overall report of a high prevalence of LOM among households should be emphasized due to its potential source of increased irrational medicine use and environmental harm. 9 In this study, antibiotics (64%) and analgesics (21%) were the two most commonly observed drug classes. However, analgesics were more prevalent than antibiotics in studies conducted in Ethiopia and elsewhere in Nigeria, India, and the United States.8,15,20,21 Interestingly, the share of antibiotics in this study is significantly higher than those studies (in Ethiopia (24%), Nigeria (16%), India (21.5%), and the United States (21%)). The increased existence of leftover antibiotics at home in this study needs more attention since it could worsen the issue of antimicrobial resistance.
In this study, the majority of observed LOMs were obtained without a prescription. This practice might be responsible for the high prevalence of antibiotics in the current study. 1 It is critical since purchasing medicine on prescription is one of the indicators of rational medicine use. 22 The most frequent reasons given by the respondents for the presence of LOM were subsided symptoms or feeling better. This finding is consistent with previous studies in Ethiopia,8,11 New Zealand, 23 and Ghana. 18 However, keeping for future use, change, or discontinuation by prescribers were the major reasons reported by findings from Kenya and Kuwait, respectively.24,25 The difference in the reasons mentioned could be due to a difference in the type of illness. For example, a Malaysian study found a difference in the reasons given for LOMs among patients with chronic and acute diseases. 26 In the study, chronic patients gave “forgot to take medicines or did not utilize them as directed by the prescriber” as their rationale. Whereas, patients with acute illnesses gave “subsided symptoms or feeling better” as their reason for having LOM in their homes.
According to a recent study on disposal practices, throwing LOMs in the trash or putting them in a latrine was the most preferred method. This finding is consistent with several previous studies.8,11,18,24 This finding could be explained by the lack of proper disposal procedures at the household level, as well as a lack of awareness among the study participants. In this study, only 0.1% of respondents considered returning it to the medical center or healthcare professionals. This figure is consistent with the findings of previous studies in Ethiopia 8 and Sweden. 27 Furthermore, the majority of respondents in this study stated that they always check the expiry date of medicines before purchasing or consuming them. However, this figure was lower than that of a study conducted in Afghanistan, where almost all study participants checked it. 18 This suggests that it is essential to improve the habit of checking the expiration date of medicines before use as it prevents detrimental effects. 1
In the present study, the majority of respondents accept that improper disposal of unused and expired medicine harms the environment and health. Our estimate is higher than that of a study conducted in Mekelle, Ethiopia. 28 However, it is lower than the study done in Kabul, where nearly all of the study subjects believed that improper LOM disposal practices would have a detrimental effect. 9 This could be due to a lack of awareness-raising programs about the environmental and health consequences of improper disposal of unused and expired medicines in our study area. In this study, for example, 80% of respondents had no prior information on the safe disposal of unused and expired medicines. As a result, survey respondents suggested that health extension workers, physicians, pharmacists, and the government are responsible for raising public awareness about the proper disposal of unused and expired medicines. Similar suggestions were raised from a study done in Harar, 8 and certain studies conducted elsewhere.9,18,24 Additionally, our findings revealed that healthcare professionals were not advising their patients enough about the proper disposal of LOMs. This gap emphasizes the importance of implementing a system that raises public awareness of safe and appropriate medicine disposal practices.
The binary logistic regression analysis revealed four variables to be statistically significant predictors of households having LOMs. The strongest variable that predicted whether a household has LOMs was purchasing medicine without a prescription. Medicines purchased without a prescription are 3.7 (p < 0.001) times more likely to be left unused than those obtained on prescription. This finding might indicate the widespread improper dispensing practices among the community pharmacies in the town. This circumstance may encourage public self-medication. Purchasing medications based on self-diagnosis leads to mistreatment and incorrect therapy selection, increasing the risk of non-adherence and medication wastage. 29 Interestingly, in this study, higher-income households are twice as likely as lower-income households to have LOM (p = 0.005). As a result, this could increase the possibility of obtaining medications without a prescription, thereby contributing to an increase in self-medication practices. Furthermore, households that waived paying for medication were 70.6% more likely than OOP payers to have LOM. This figure is consistent with the findings of an Afghan study. 9 In contrast, one Malaysian study revealed that participants who paid for medicine were six times more likely to have LOM in their homes than non-payers. According to the study, the main reason was a lack of advice on rational medicine use and proper disposal of leftover medications in the private healthcare sector. So, our findings could imply that public healthcare facilities are not educating people about proper medication use and disposal practices. Thus, public healthcare institutions are in charge of providing free or insured medicines in Ethiopia. 30 Therefore, the Ethiopian government and concerned stakeholders should be concerned about free provided medicines to reduce the wastage of medications. In addition, households with no person having a chronic illness (requiring regular medication) had a 55% higher likelihood of possessing leftover medications than households with such an illness. A consistent finding was observed from a Malaysian study. 30 It has been reported that there is a significant possibility of an oversupply of medicines for acute illnesses that are typically stored for future use in developing countries. 23
Concerning the predictors of disposal practices, respondents who were aware of proper disposal practices were more likely to decide to dispose of rather than keep them for future use. Likewise, the improper disposal of LOMs was more likely to be observed in uniformed households 20 and Malaysia. 26 These findings could indicate that the more people are educated about proper LOM disposal, the more likely it is that public disposal practices will improve. However, novel approaches to raising awareness are required. For example, in this study, the majority of (80%) respondents who considered their current LOMs disposal was appropriate preferred to dispose of it in the garbage or latrine, and almost none claimed to return it to the medical center. Similarly, a Malaysian study revealed that healthcare professionals’ advice and proper disposal of medicine were not significantly associated. 26 Therefore, initiatives such as a campaign or other novel approaches involving the public and private health institutions, healthcare professionals, patients, and other concerned parties should be implemented to increase awareness of proper disposal practices and the impact of LOM on the environment and health. The government and decision-makers should also consider implementing a drug take-back program and setting up facilities for it. Moreover, in the present study, respondents with tertiary education have designated places of storage for LOM than those with primary education or less. This finding is inconsistent with a previous study in Adigrat, Ethiopia. 31 In the study, having a level of education did not show an association with the awareness of the proper disposal of LMOs. This disparity could be attributed to sociodemographic differences between participants from different regions of the country. As a result, this finding is tentative, and further research is required to justify this finding.
Limitations of the study
This study had several limitations. First, we conducted the study using a smaller sample size and a sample of the urban residents of Arba Minch town. As a result, we cannot generalize the finding to the entire Gamo Zone population, which includes the rural community. The sampling method and technology used could help to reduce the generalizability limitation. Future studies should cover rural areas to cover this limitation. Second, the survey is based on the participants’ recall and is likely to be biased by public acceptance. However, these limitations could not invalidate the study findings. For example, a door-to-door interview allows the investigator to observe the type and quantity of LOMs, allowing them to address recall and public acceptance bias. Additionally, the household visit could also help to find more representative respondents using a better sampling technique and technology. It is also appropriate for subsequent follow-up surveys and for measuring improvements in proper medicine use and disposal practices.
Conclusions
The present study revealed a high prevalence of LOMs and their improper disposal practices in Arba Minch town. Significant factor variables that predict having LOMs are attributed to purchasing medicine without a prescription, higher family monthly income, those waived paying for medicine, and those who used medications for acute diseases. In this study, the preferred method of LOM disposal deviates from conventional standards such as WHO recommendations. Prior knowledge of proper disposal practices predicated the decision to dispose of current LOMs or keep them for future use. The level of education determined whether the possessed LOM had a designated or random location in the house. This study found a lack of knowledge about proper disposal practices. The findings would be critical in developing strategies to reduce LOMs in the public and promote their proper disposal practices. Furthermore, the method used and findings of this study can be used as a foundation for future investigation in the area of the topic.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231158214 – Supplemental material for Prevalence of leftover medicines, disposal practices, and associated factors in Arba Minch Town, Southern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121231158214 for Prevalence of leftover medicines, disposal practices, and associated factors in Arba Minch Town, Southern Ethiopia by Getahun Asmamaw, Tewodros Agedew, Besrat Tesfaye, Samrawit Sasamo, Saude Gena, Melkamu Argeta and Aynoshe Adio in SAGE Open Medicine
Footnotes
Acknowledgements
We appreciate all who voluntarily agreed to participate in the interviews and provided data in the study.
Author contributions
GA and BA conceived and designed the study. GA and TA performed analysis and interpreted the data. BA, TA, and BE executed the data collection and research work. GA drafted the manuscript. TA and AA reviewed the statistical analysis, and reviewed and edited the draft manuscript. All authors reviewed and approved the final version of the manuscript.
Availability of data and material
The research data set is available upon request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and informed consent
Ethical approval was obtained from the Ethics Review Committee of the department of Pharmacy, Arba Minch University (approval reference number: IRB/1299/2022). Then a formal letter was written from the Department of Pharmacy to Bere Ediget Bere and Nech Sar Kebele administration and other concerned bodies to get permission for conducting the study. All methods were carried out following the Declaration of Helsinki's ethical guidelines. All subjects provided written informed consent.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.