
Abstract
Objective:
The present study seeks to find a way to quickly and correctly differentiate myocardial infarction from unstable angina by measuring the creatine kinase-MB/creatine phosphokinase ratio and comparing in non-ST elevation myocardial infarction patients with unstable angina at different time intervals, to improve the health quality of patients with coronary artery disease.
Methods:
The present study is a retrospective epidemiological analysis of 260 patients with non-ST elevation myocardial infarction and 260 patients with unstable angina, including age, sex, creatine kinase-MB, and creatine phosphokinase biomarkers at two-time intervals, including referral (4–8 h from the onset of pain) as the first interval, and 8 h after the first sampling was extracted as the second interval. Moreover, the delta of the creatine kinase-MB/creatine phosphokinase ratio during two interval times was measured.
Results:
In non-ST elevation myocardial infarction patients in the first and second intervals, creatine kinase-MB/creatine phosphokinase ratio was 32.7 and 33.8% higher than the normal laboratory cutoff (positive), respectively, and in the group of unstable angina patients, this index was positive in 31.9 and 30.4% of patients, respectively. There was no significant difference between the mean creatine kinase-MB to creatine phosphokinase index between the patients with non-ST elevation myocardial infarction and unstable angina (p = 0.507). In the first interval, the sensitivity and specificity of this index in differentiating non-ST elevation myocardial infarction from unstable angina were 51.5 and 57.3% (area under the curve = 0.518), respectively. While in the second interval, the sensitivity and specificity of this index were 17.7 and 87.8% (area under the curve = 0.519), respectively. The creatine kinase-MB/creatine phosphokinase delta in the non-ST elevation myocardial infarction group was significantly higher than in patients with unstable angina during different time intervals (p = 0.01).
Conclusion:
According to our results, creatine kinase-MB/creatine phosphokinase index cannot help differentiate the two groups of non-ST elevation myocardial infarction and unstable angina. However, the findings show that higher levels of creatine kinase-MB enzyme and creatine kinase-MB/creatine phosphokinase delta in the early hours, 4–16 h after the onset of pain in non-ST elevation myocardial infarction patients, can be used to differentiate between non-ST elevation myocardial infarction and unstable angina.
Keywords
Introduction
Coronary artery disease (CAD) is one of the leading causes of death worldwide, accounting for 17.8 million deaths annually. 1 Mortality attributed to CAD is declining in many developed countries but is increasing in developing countries due to increased life expectancy, urbanization, and lifestyle changes. 2 In Iran, CAD is one of the main causes of death, and according to recent studies, mortality from CAD has increased by about 20–45%. 3 In CVD, myocardial infarction (MI) is the most common cause of mortality and morbidity. 4 Reports from the world’s largest data center on patients with acute coronary syndromes (ACS) show that the percentage of patients diagnosed with non-ST elevation MI (NSTEMI) is increasing dramatically, which is probably due to the emergence of higher sensitivity assays for diagnosis of myocardial damages. 5 The spectrum of patients with ACS includes unstable angina (UA), NSTEMI, and STEMI. In the traditional method for their differential diagnosis, the presence of either clinical symptoms compatible with acute MI and typical ischemic electrocardiogram (ECG) changes or increased and decreased serum cardiac biomarkers was necessary. 6 Newer methods for diagnosing ACS include echocardiography, computed tomography angiography, magnetic resonance angiography, and myocardial perfusion imaging, 7 which due to limited emergency access to them, cardiac biomarkers are thus necessary to use. 7
NSTEM is an acute cardiac ischemic event that causes cardiomyocyte necrosis. The main symptom that initiates the diagnostic and therapeutic chain in patients with suspected ACS is chest pain 8 ; however, to complete the diagnosis of NSTEMI a significant criterion, the typical pattern increases and then gradually decreases in cardiac biomarkers (troponin and CK-MB) along with one or more symptoms compatible with acute MI, typical ischemic ECG changes, imaging evidence of myocardial disorder, cardiac wall motion abnormalities, intracardiac thrombosis found on angiography. 9 UA is a disorder in the ACS spectrum that is defined by myocardial ischemia without detectable necrosis with steadily increasing incidence (nearly 1 million patients admitted to the initial diagnosis each year). 10 The risk of MI, adverse events, and death in UA varies due to the wide range of clinical manifestations of the disease, but the average rate of cardiovascular events following UA over 12 months was 42.9% in patients with NSTEMI and 37.5% in patients with STEMI. 10 These indicate the need to correctly diagnose UA and choose an appropriate treatment to prevent subsequent accidents. Therefore, it is necessary to identify cardiac biomarkers that have diagnostic and therapeutic value as well as are cost benefit.
Previous studies on measuring cardiac biomarkers for diagnosing CAD have presented different and sometimes contradictory results. 11 Several recent experimental systems have been designed and implemented to find more sensitive and specific biomarkers, including CK-MB mass, hsTnT, and myoglobin. However, there have been limitations, such as a low statistical population or involvement of patients with STEMI.12–14 The present study seeks to find a way to quickly and correctly differentiate MI from UA by measuring the CK-MB/CPK ratio and comparing it in NSTEMI patients with UA at different time intervals, to improve the quality of health in patients with CAD.
Methods
The present retrospective analytical study was performed on hospital information about patients who were admitted to the cardiac care unit with a diagnosis of ACS (NSTEMI and UA) referred to the emergency department of a tertiary care hospital in the Southern region of Iran from January 2019 to December 2020. Since no similar comparative clinical research has been done regarding the investigated factor and other compared factors (such as LDH, LDL, HDL) between the two groups were not suitable for determining the sample size, so based on the prevalence of acute coronary syndrome patients. In the epidemiological study of cardiovascular patients hospitalized in Jahrom Hospitals in 2013, 15 the sample size is estimated to be 520 people, taking into account the power of 80 and the probability of type 1 error of 0.05.

Inclusion criteria
Patients without ST elevation on ECG with elevated troponin T biomarker level (as NSTEMI group), those without ST elevation without increasing troponin T biomarker (as UA group), and individuals with chest pain onset interval of 4–8 h to sampling were included. The first sample was determined for 8 h until the second sampling. Time intervals were adjusted according to the kinetics of biomarkers with the least amount of interference with the peak value of biomarkers among patients because of serum CPK and CK-MB increase within 3–6 h and peak in 16–30 h following the onset of MI symptoms.16,17
Exclusion criteria
Patients with pain onset time from sampling to less than 4 h and more than 8 h, lack of sufficient information in the file, increase in troponin T biomarker level at any time in UA patients, or ST elevation in patients ECG, no information about CK-MB and CPK enzymes measures in the patient’s files, and if the laboratory kit used by the patient did not match the rest of the patients, were excluded.
Data collection
Data from 520 patients consisting of 260 patients with NSTEMI and 260 patients with UA, including age, sex, and CK-MB and CPK biomarkers at intervals including referral (4–8 h from the onset of pain) were considered as the first sample. Then, 8 h after the first sampling, data were considered the second sample. CK-MB/CPK ratio was calculated at each sampling time, and the values of CK-MB and CPK biomarkers and CK-MB/CPK index alongside their normal cutoff were considered according to values mentioned in the laboratory kit instructions (Bionik co., Tehran, Iran). According to the normal cutoff provided in the laboratory kit brochure, each of the CPK and CK-MB enzymes and the CK-MB index were examined concerning their normal cutoff. These values were less than 24 IU/L for CK-MB, less than 195 IU/L for CPK in male patients, less than 175 IU/L in female patients, and more than 25% for CK-MB/CPK. In general, values of interest in patients and gender were calculated and compared during the two sampling times, and their changes were recorded. Also, by obtaining the delta of CK-MB/CPK index values during two sampling times in both disease groups, this variable between the two disease groups was examined.
Ethical consideration
Ethical approval for the study was obtained from the Institutional Ethics Committee of Golestan Hospital, Ahvaz, Southern region of Iran.
Statistical analysis
In quantitative variables, mean or median and standard deviation or interquartile range were used. In qualitative variables, frequency and percentage were used to describe data. The normality of the data was evaluated using the Kolmogorov–Smirnov test and Q–Q diagram. All analyses were performed using SPSS software version 20. The significance level was considered p < 0.05.
Results
Of 520 patients with ACS symptoms, 260 patients had UA with an average age of 51 ± 11 years (122 women (46.92%) and 138 men (53.08%)), and 260 patients diagnosed with NSTEMI had an average age of 55.11 ± 12 years (108 women (41.54%) and 152 men (58.46%)) (Table 1). The average CK-MB in the NSTEMI group (4–8 h from the onset of symptoms) and 8 h after the visit were 43.70 and 55.31 IU/L, which significantly increased over time (Table 2, p < 0.001). Also, the mean CK-MB in the group of patients with UA at the referral time and 8 h after the visit were 17.26 and 21.34 IU/L, which increased over time (Table 2, p < 0.001). In comparison between the two groups of NSTEMI and UA, the mean CK-MB in the NSTEMI group was significantly higher in both time intervals (Table 2, p < 0.001). Besides, the average CK-MB rate in both time intervals in male patients with NSTEMI was higher than that in women (Table 2, p < 0.001).
Comparison of the average CK-MB/CPK ratio in patients with NSTEMI and UA.

UA: unstable angina; NSTEMI: non-ST elevation myocardial infarction; SD: standard deviation; CK-MB: creatine kinase-MB; CPK: creatine phosphokinase.
Comparison of the average CK-MB/CPK ratio in patients with NSTEMI and UA.

First, 4–8 h from the onset of symptoms; second, 8 h after the visit. UA: unstable angina; NSTEMI: non-ST elevation myocardial infarction; SD: standard deviation; CK-MB: creatine kinase-MB; CPK: creatine phosphokinase.
By examining the CPK enzyme at both time intervals, the mean concentration in patients with NSTEMI at the first and second intervals was reported as 268.75 and 345.43 IU/L, respectively. The average concentration of this enzyme in UA patients during these intervals was 104.06 and 122.34 IU/L, respectively, which indicated its uptrend over time (Table 3, p < 0.001). A comparison of CPK values between the two study groups shows that CPK levels are higher in patients with NSTEMI than those in UA (Table 3, p < 0.001). Moreover, CPK levels reported in the first interval in the male patients with UA were higher than those in female patients (Table 3, p = 0.05).
Comparison of the average CK-MB/CPK ratio in patients with NSTEMI and UA.

First, 4–8 h from the onset of symptoms; second, 8 h after the visit. UA: unstable angina; NSTEMI: non-ST elevation myocardial infarction; SD: standard deviation; CK-MB: creatine kinase-MB; CPK: creatine phosphokinase.
By measuring the CK-MB/CPK ratio, the analysis shows that its average in the NSTEMI group at the first and second intervals was 0.2242 and 0.2200, respectively. In comparison, this value in UA patients was 0.2195 and 0.223, respectively, with no statistically significant difference between the two study groups (Table 4, p = 0.506). However, a significant ascending pattern has been shown in patients with NSTEMI (Table 4, p = 0.014). Also, considering different gender groups in data analysis, it was found that a significant ascending pattern has been shown in male patients with NSTEMI (Table 3, p = 0.014), while the nonsignificant association between gender and other subgroups of study with the amount of CPK enzyme was found (Table 4, p > 0.05).
Comparison of the average CK-MB/CPK ratio in patients with NSTEMI and UA.

First, 4–8 h from the onset of symptoms; second, 8 h after the visit. UA: unstable angina; NSTEMI: non-ST elevation myocardial infarction; SD: standard deviation; CK-MB: creatine kinase-MB; CPK: creatine phosphokinase.
In patients with NSTEMI, the percentage of positive cases of CK-MB values at first and second intervals was 55.5 and 77.7%, respectively; hence, in patients with UA, it was 18.1 and 29.2%, respectively. The increasing number of cases above the normal cutoff was statistically significant in both study groups. Also, comparing the two study groups shows positive cases in NSTEMI patients than in the UA group (Table 5, p < 0.001). Nevertheless, the results show no significant difference between the number of CK-MB positive cases among various gender subgroups in both study groups (Table 4, p > 0.05). The number of cases with CPK positive values in the group of patients with NSTEMI at the first and second intervals was 40.8 and 50.4%, respectively (Table 4, p = 0.035); while in the group of patients with UA, 11.5 and 17.3% of patients had positive CPK values, respectively (Table 5, p = 0.081). Finally, no significant relationship was observed between gender and positive cases of CPK (Table 5, p > 0.05). The results showed that the mean CK-MB/CPL ratio in NSTEMI patients at the first and second intervals was 85 and 88%, respectively (Table 5, p = 0.852); also, in patients with UA, these values were 83 and 79%, respectively (Table 5, p = 0.776). Thus, there was no significant difference in the mean CK-MB/CPL ratio between the two groups of patients (Table 5, p = 0.507). Also, the difference in values between women and men in both groups was not statistically significant (Table 5).
Relationship between CK-MB, CPK variables, CK-MB/CPK ratio, and normal cutoff in two sampling sessions in patients with NSTEMI and UA (number (%)).

AN: abnormal values; N: normal values; UA: unstable angina; NSTEMI: non-ST elevation myocardial infarction; SD: standard deviation; CK-MB: creatine kinase-MB; CPK: creatine phosphokinase.
Based on the area under the curve ratio, the accuracy of the index obtained from the first and second samples to differentiate the two study groups, including patients with NSTEMI and UA, was 51.8 and 51.9%, respectively. Moreover, based on statistical calculations, the recommended cutoff for differentiating NSTEMI from UA within 4–8 h from the onset of pain was higher than 0.19, and at 8 h after the first sampling it was higher than 0.33 (Figure 1). The mean delta index during sampling times in NSTEMI patients was 0.0058, and in UA patients was −0.0062. Also, the CK-MB/CPK delta index was significantly higher in NSTEMI patients than in patients with UA (p = 0.01).
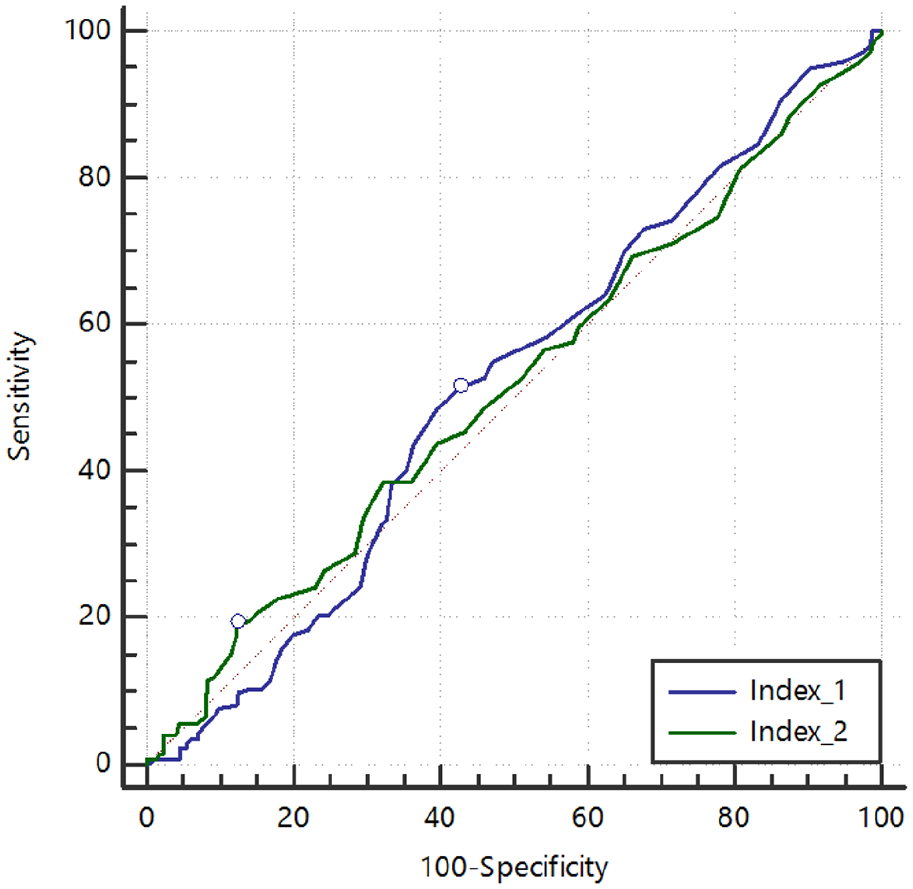
Sensitivity and specificity of CK-MB/CPK ratio in both time intervals.
Discussion
Risk assessment in patients with ACS, especially those with NSTEMI and UA, should be performed immediately at the time of admission so that treatment decisions can be made at the first contact with the patient. This is a critical point in starting the treatment approach because patients require different treatments depending on the mortality or ischemic risks. Patients with chest pain but no clear diagnostic findings on the ECG pose a significant challenge for the diagnosis, requiring us to use other diagnostic methods in addition to the ECG, including biomarkers such as CK-MB and CPK.18,19 In a healthy adult, serum CPK levels vary depending on a number of factors, including gender, race, and activity level. Very high serum CPK levels can indicate muscle damage due to chronic diseases. Serum CPK and CK-MB levels increase within 3–6 h from the onset of symptoms of MI and reach the highest values within 16–30 h. 20 Consequently, CK-MB levels in the blood return to normal after 24–36 h. 21
In contrast, increased cardiac troponin can be measured in the blood for 10–14 days. 21 According to the results of the present study, the mean values of CK-MB and CPK increased in both NSTEMI and UA patients. Elevated CK-MB and relative CK-MB to CPK index in ACS patients and for the diagnosis of acute MI have been studied in several studies, but few have compared the two groups, NSTEMI and UA patients.
Gibler et al., in a study on 69 patients with a definitive diagnosis of AMI who did not have an ECG at the time of their initial visit (NSTEMI), with a serial sampling of CK-MB at zero hours (at the time of referral), 1, 2, and 3 h of the patients referred, showed the sensitivity of CK-MB increases from 43.8 to 79.7% at the time of patient arrival in the third hour of referral and the overall accuracy of CK-MB in diagnosing AMI in the emergency was 92%. This study showed that the sensitivity of CK-MB is highly dependent on the sampling time from the onset of pain. 22 Another study by Kleiman et al. compared troponin and CK-MB to predict risk in NSTEMI patients and found that out of 668 patients with positive CK-MB, 94% were troponin positive, and of 1157 patients with negative CK-MB, 32% were positive for troponin, which showed a significant correlation between troponin and CK-MB. 12 Fesmier et al. performed a study on 975 patients with NSTEMI and troponin-negative (UA) that underwent two rounds of sampling of patients at the beginning of the visit (with the average onset of symptoms up to 4.5 h of sampling) and 2 h after the visit. The measurement of CK-MB showed that it imposed a sensitivity of 66% at the baseline, which increased to 89% 2 h later. CK-MB shows a better sensitivity that was consistent with the results of the present study. 13 Young et al. also studied the serial measurement of CK-MB in patients with chest pain and nondiagnostic ECG by sampling 1043 patients several times from the onset of symptoms (less than 3 h, 3–6 h, 6–12 h, and more than 12 h), where CK-MB diagnostic sensitivity was reported as 38, 75, 92, and 100%. They concluded that serum CK-MB sensitivity increases during the measurement time, especially during 3 h of patient observation, and is suitable for diagnosing NSTEMI. 23 Jernberg et al. conducted a comparative study of troponin, CK-MB, and myoglobin for the rapid diagnosis or rejection of AMI in patients with nondiagnostic chest pain at baseline, 3, 6, and 12 h after referral. Data analysis showed that at the beginning of the visit, CK-MB had high sensitivity (80%) and specificity (89%) compared to troponin, which had a sensitivity of 59% and a specificity of 91%. Six hours after referral, CK-MB had an increase in sensitivity (100%) and a slight decrease in specificity (80%). Troponin showed 91% sensitivity and 93% specificity. In this study, CK-MB in the sixth hour after patient referral showed high sensitivity and negative predictive value, but its specificity and positive predictive value were relatively low. 24
Based on the results of the present study, CK-MB, CPK, and CK-MB/CPK ratios were reported to be higher than the normal (positive) cutoff in the NSTEMI patient group, which indicates that CK-MB seems to be a more appropriate indicator for the diagnosis of NSTEMI. Also, in UA patients, CK-MB, CPK, and CK-MB/CPK ratios were higher than the normal (positive) cutoff, indicating that the CK-MB/CPK ratio seems more valuable for better UA differential diagnosis. A retrospective study on the clinical utility of CK-MB measurement in patients with suspected ACS concluded that 1214 patients with conflicting biomarker values were not sufficient evidence to support a diagnosis. Thus, CK-MB has limited clinical utility, and using this biomarker to diagnose AMI may not be appropriate once contemporary troponin values are available. 25 Hedges et al. measured CK-MB in a prospective cohort study on the effect of CK-MB on clinical decision-making in patients with chest pain over 25 years of age with nondiagnostic ECG (NSTE-ACS) values at baseline and 3 h later. In patients with the final diagnosis of UA at the baseline, 99% had negative CK-MB values, and in the second time interval, 95% of patients had negative values of this biomarker. While in 67 patients diagnosed with NSTEMI in the first interval, 57% and in the second interval, 88% had negative CK-MB values. They concluded that CK-MB biomarkers might not help UA patients’ diagnosis and clinical decisions. 26 Vols et al. also measured troponin, CK-MB, and CPK in patients with ACS symptoms at baseline and 11 h later, of whom a small fraction was CK-MB/CPK positive, but none of them were eventually admitted with a diagnosis of AMI; so, they concluded that despite the negative troponin, measurement of CK-MB was not necessary for the diagnosis of AMI. 27 However, in this study, the positive value of the CK-MB index was considered above 6%, which, compared to the value considered in the present study (25%), naturally includes more positive values and will probably affect the false positives of this biomarker. Capellan et al. also compared the predictive properties of the first absolute CK-MB and the relative CK-MB index for the diagnosis of AMI, ACS, and major cardiac events (SCE), examining patients over 24 years of age with chest pain. They concluded that the absolute value of CK-MB, compared to the relative index of CK-MB, has higher sensitivity, similar negative predictive value, specificity, and lower positive predictive value for AMI, ACS, and SCE diagnosis. 28
Also, according to the present study, the mean CK-MB in NSTEMI patients is significantly higher in men than women; however, no significant relationship was found between sex and other enzymes index. Diagnosis of CAD in women is more difficult due to factors such as nonspecific symptoms and the accuracy of noninvasive tests. Wiviott et al., on the difference between the incidence of cardiac biomarkers in patients with UA and gender-appropriate NSTEMI, showed that women had significantly lower positive CK-MB than men. 29 Motiwala et al., in a clinical trial study of biomarkers in ACS and heart failure, found that 42% of men and 29% of women had higher CK-MB levels than the standard cutoff. Men were also significantly more likely to have elevated CK-MB and troponin levels than women at the time of referral. 30 Culić et al. studied the symptoms of AMI under the influence of sex, age, and risk factors and found that mean CK-MB was 105 in men and 94 in women, and there was a significant difference between men and women. 31
Influencing biomarkers by various factors and underlying disorders is one of the significant challenges that should be considered in interpretation. The severity of CK-MB in cardiac disorders in patients with metabolic diseases is significantly higher than in normal subjects. 32 In addition to the pathologic situations, the increasing CK-MB influences such normal statuses, including exercising. 33 Evaluating the other ratios can improve the accuracy of these biomarkers. Neutrophil to lymphocyte ratio (NLR) in UA is lower than in acute MI, so besides, the CK-MB/CPK assessment of NLR can indicate the extent of injury. 34 In this regard, investigating both ratios in a homogeneous population is highly recommended.
Our main limitation in the present survey is the heterogeneous population. Further studies to compare increasing CK-MB/CPK in normal subjects to patients with underlying disorders are highly suggested.
Conclusion
High CVD-related mortality and healthcare-related financial costs have led to several researchers developing novel methods for timely and early diagnosis, decision-making, accurate treatments, and assessing disease prognosis. According to the present study’s findings, it can be said that due to the specificity and low sensitivity of the CK-MB/CPK index in differentiating the two groups of NSTEMI and UA, this index does not help much to differentiate between these two groups of diseases. However, the findings show higher levels of CK-MB enzyme and CK-MB/CPK delta in the early hours after the onset of chest pain (4–16 h after the onset of pain) in NSTEMI patients can be used to differentiate between NSTEMI and UA.
Footnotes
Acknowledgements
We thank all our colleagues at Allied Health Sciences School, Ahvaz Jundishapur University of Medical Sciences.
Author contributions
ARN, MM, and HM designed the study, analyzed the original survey data, and created the first draft manuscript. HM, ZT, and ARN reviewed the data interpretation from the original studies and contributed to manuscript revisions .
Availability of data and materials
The current study’s generated and/or analyzed datasets are available in the (PubMed, Web of Science, Scopus, EM Base) repository.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This article is based on MD this thesis and research project no IR.AJUMS. GOLESTAN.REC.1398.040 at Ahvaz Jundishapur University of Medical Sciences and approved by the Ethics committee affiliated with Ahvaz Jundishapur University of Medical Science.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human participants
All procedures performed in studies involving human participants followed the ethical standards of the institution and/or national research committee and with the 1964 Helsinki declaration and its later amendments or compare ethical strands.
Informed consent
Written informed consent was obtained from all subjects before the study.