
Abstract
Background:
Traditional birth attendant utilization has become a common malpractice and a leading cause of maternal morbidity and mortality in the developing world, such as Ethiopia. Therefore, this study was aimed at determining the geospatial variation and determinant factors of traditional birth attendant utilization among mothers of reproductive age in Ethiopia.
Methods:
The data were taken from the 2019 Ethiopian Demographic and Health Survey. Arc GIS, Excel, and STATA-14 software were used for the data analysis. The adjusted odds ratio with a 95% confidence interval was used to declare significant determinants of traditional birth attendance among mothers of reproductive age in Ethiopia.
Results:
Among 5,753 mothers of reproductive age, 34.59% of them utilized traditional birth attendants in Ethiopia during the 2019 Ethiopian Demographic and Health Survey. There was a geospatial variation of traditional birth attendants among mothers of reproductive age in Ethiopia; the Global Moran’s index value was 0.39 with a p-value <0.001. The significant factors associated with traditional birth attendant utilization were the age of mothers; higher odds were observed among older mothers aged 35–49 years (AOR = 1.31; 95% CI (1.04–1.63)); educational level of mothers (AOR = 3.04; 95% CI (2.13–4.33)); higher odds were observed in uneducated mothers, wealth index (AOR = 2.76; 95% CI (1.83–4.19)); higher odds were observed among the poorer and poorest households, place of residence (AOR = 5.69; 95% CI (3.35–9.67)); and the regions; the highest odds were observed in Somali (AOR = 12.1; 95% CI (4.99–25.68)) and Afar (AOR = 7.13; 95% CI (2.37–21.38)).
Conclusions:
The utilization of traditional birth attendants among reproductive-age mothers became a major public health concern, and the distribution showed geo-spatial variations among the regions of the country. We recommend taking appropriate measures to alleviate the current problem by improving access to maternal healthcare services.
Introduction
According to the World Health Organization (WHO), a traditional birth attendant (TBA) is defined as “a person who assists a mother during childbirth and who initially acquired her skills by delivering babies herself or through apprenticeship to other traditional birth attendants.” 1 TBAs are community-based health workers who assist women during childbirth. They often have cultural knowledge and experience, but they lack formal medical training. 2 TBA is also described as a person who assists the mother during childbirth, traditionally or culturally, without formal education or training about maternal care. The purpose of the interaction between TBAs and the women will be to provide traditional care during pregnancy, childbirth, and postpartum. TBAs have no formal training levels; their involvement is mostly confined to childbirth, providing community-based maternal and newborn care with an emphasis on cultural traditions. The interactions between women and TBAs have individual variations. 3 Maternal mortality remains one of the most common public health challenges in the developing world. 4 Previous studies indicated that about 99% of maternal deaths occur in low- and middle-income countries. The highest burden of maternal mortality was observed in sub-Saharan African countries, estimated at as high as 198 per 1,000 live births.5,6 One of the preventable causes of maternal mortality was problems related to birth attendants, as identified in the previous studies.6,7 TBA utilization is a harmful practice, and every mother should have skilled birth attendants at the health facility. During traditional birth assistance, mothers may be exposed to infection, unsafe abortion, newborn complications, obstetric emergencies, and postpartum hemorrhage. As a result, the mother may die at home because TBAs cannot manage such maternal and child cases. To some extent, TBAs may help with maternal health care during childbirth in rural communities in developing countries like Ethiopia, where they are considered birth attendants by the community.8–10 Previous studies showed that most mothers usually prefer TBAs to skilled birth attendants. TBAs assist the mother during birth and after childbirth. Their assistance depends on the cultural context, which varies from place to place and region to region across the country.9,11 According to previous studies, significant factors associated with pregnancy-related complications are friendly care from TBAs, the inability to get care from a skilled birth attendant, lower socioeconomic status, the number of children in the household, living in rural residences, mothers without formal education, an easily inaccessible delivery environment, and the cultural and spiritual beliefs of the mothers.12–14
The preference for TBAs was strongly related to cultural and religious beliefs, a culture of shyness, and the need for privacy during pregnancy and childbirth, TBAs close proximity at the time of childbirth, and adherence to their traditional practices.15,16 These cultural barriers interplay with geographical, transportation, and financial factors, challenging pregnant women to deliver in the health facility. 17
Conducting spatial studies has practical implications for maternal health services. Understanding spatial patterns of TBA utilization helps identify disparities in access to maternal care services. By pinpointing areas with high TBA utilization, health authorities can allocate resources more equitably and improve access for underserved communities. Spatial data allows for targeted interventions. For instance, if certain villages predominantly rely on TBAs, health programs can collaborate with these practitioners to enhance their skills, ensure safe maternal healthcare practices, and provide necessary supplies. Spatial analysis of TBA utilization provides actionable insights for improving maternal health services, promoting equity, and ensuring timely care for pregnant women to prevent maternal morbidity and mortality.18,19
WHO and other international organizations have focused on maternal mortality reduction efforts on the availability of skilled birth attendance, which excludes traditional birth attendance as providers of maternal care during childbirth. 2 However, the utilization of traditional birth attendance during birth remains a common practice in low- and middle-income countries, including Ethiopia. The previous studies mainly focused on antenatal care and skilled birth attendance. Even if there are few studies related to our study, there is a lack of adequate, updated, and comprehensive evidence on TBA utilization in Ethiopia. Therefore, this study was conducted to determine the geospatial variation and determinant factors of TBA utilization among mothers of reproductive age in Ethiopia.
Methods
Study design and setting
This study was a spatial distribution and multilevel analysis study conducted in Ethiopia using data from EDH. The country is located in the Horn of Africa between 3° and 15 degrees North latitude and 33 and 48 degrees East longitude (3°–15° N and 33°–48° E). Ethiopia has nine regional states: Tigray, Amhara, Afar, Somalia, Oromiya, Benishangul-Gumuz, Gambela, Southern Nation Nationalities and People (SNNP), and Harari, as well as two city administrations: Addis Ababa and Dire Dawa, which make up its administrative system. The regions are further subdivided into 68 zones, 817 districts, and 16,253 Kebeles, the lowest level of administrative entities in the nation.
Data source, extraction, sampling procedure, and study participants
The source of data for this study was the Ethiopian Demographic and Health Survey (EDHS) 2019 national survey. The EDHS data was collected by the Central Statistics Agency of Ethiopia. Permission was obtained to download the EDHS data sets in STATA format from the DHS website. Two stages of cluster sampling were used to gather and stratify the EDHS samples. After stratifying each region into urban and rural areas, 305 cluster areas (212 rural and 93 urban) were chosen for the first step.
The newly constructed household listing was used to choose a fixed number of 30 households per cluster, with an equal likelihood of systematic selection, for the second step of the selection process. All women aged 15–49 who were either permanent residents of the selected households or visitors before the survey, were eligible to be interviewed. All women of reproductive age during the surveys in Ethiopia were the source of the population for this study, whereas all women of reproductive age in the selected enumeration areas during the survey were the study population. Ultimately, a total representative sample of 5,753 reproductive-aged women was included in the 2019 survey.
Study population and eligibility criteria
Reproductive-age women who are 15–49 years old in Ethiopia were the source population. The study population was all the reproductive-age women who were in the selected enumeration areas included in the analysis. A total of 5,753 participants were included in this study. Women who are not within the reproductive age range as defined by the study, survey responses that are incomplete or missing crucial data for the multilevel logistic regression analysis, and data from women who did not consent to the use of their information for research purposes were excluded from this study.
Variables of study
Dependent variable
The dependent variable in this study was the utilization of TBAs, which was derived from the DHS question on assistance to TBAs during birth, dichotomized into “yes” if the reproductive-aged women were assisted by TBAs during birth and “no” if the reproductive-aged women were not assisted by TBAs during birth.
Independent variables
The independent variables included sociodemographic and economic factors at the individual and community levels. Age of the mother, maternal education, religion, household size, wealth index, number of under-5 children in the house, antenatal care visits, place of delivery, and geographical factors like region and place of residence were the independent factors of TBAs among reproductive-age women. The explanatory variables included as independent variables in this study were derived from literature and previous studies.20–23 They were not chosen arbitrarily.
Data management
To restore the survey’s representativeness, the sample weights were applied to compensate for the unequal probability of selection between the strata. The STATA version 14 software was used to conduct descriptive statistics and multilevel analysis. A spatial map was also produced for a visual presentation of the utilization of TBAs at the regional and district levels using ArcGIS version 10.8.
Spatial autocorrelation analysis
The spatial autocorrelation (Global Moran’s Index) statistic measure was used24,25 to assess whether the utilization of TBAs among reproductive-age women was dispersed, clustered, or randomly distributed in the study area. Moran’s index was used to detect the spatial autocorrelation of the utilization of TBAs. The calculated Moran’s index values close to −1 indicate utilization of TBAs among reproductive age women was dispersed, whereas Moran’s index close to +1 indicates utilization of TBAs was clustered, and Moran’s index value zero indicates utilization of TBAs among reproductive age women was distributed randomly. A statistically significant p-value <0.05 indicates the presence of spatial autocorrelation.
Hotspot analysis
Hotspot analysis was conducted to determine how the spatial distribution of utilization of TBA varies across the regions of Ethiopia. The statistical significance is determined by a p-value <0.05. A “hotspot” area indicates a high prevalence of TBAs, while a “coldspot” area indicates a low prevalence of TBAs.
Spatial interpolation analysis
To anticipate the areas not included in the sample from the sampled values, the spatial interpolation approach was used. For predicting and producing smooth surfaces for TBAs, the Kriging interpolation approach was utilized. Kriging interpolation analysis was applied in this study to evaluate the burden of TBAs among reproductive-age women.
Multilevel binary logistic regression
A multilevel logistic regression model was fitted to determine factors associated with the utilization of TBAs among reproductive-age women at the individual/household, and community levels. Four models were fitted. The first (null) model contains only the outcome variable to assess the degree of the intra-cluster variations of TBAs. The second model contains individual-level variables. The third model contains only community-level variables. The fourth model contains both individual-level and community-level variables. A p-value of <0.05 was used to declare statistical significance. Adjusted odds ratios (AOR) with a 95% confidence interval (CI) were calculated to identify the factors associated with TBAs. For examining the cluster-level variability of TBA utilization, we have employed random effect analysis. The intra-class correlation coefficient (ICC), deviance, proportional change in variance (PCV), median odds ratio (MOR), and log likelihood ratio (LLR) were used as indicators of heterogeneity. The degree of heterogeneity of TBA utilization between clusters was quantified by ICC, calculated as ICC = Vc/(Vc + 3.29 × 100%), where; Vc = cluster level variance. The MOR quantifies the variation in TBA utilization between clusters in terms of the odds ratio scale and is calculated as MOR = e0.95 √variance. Moreover, PCV demonstrates the variation in TBA utilization explained by the determinants computed as PCV = (Vnull − Vc)/Vnull × 100%, where Vnull = variance of the null model and Vc = cluster level variance. Due to the nested nature of the models, deviance and LLR were used for model comparison. The model with the lowest deviance and highest LLR was considered the best fit.
Results
Sociodemographic characteristics of the study participants
A total of 5,753 mothers of reproductive age were included in this study. Among the total, more than three-fourths (76.92%) of the mothers lived in rural areas, and more than half (53.83%) of the mothers were in the age category of 25–34 years. More than half (54.74%) of the mothers have no formal education, and more than one-third (34.14%) of the mothers live in the poorest households. Almost half (50.08%) of the mothers of reproductive age had delivered their child in their home. More than one-fourth (26.24%) of the mothers of reproductive age had no antenatal care visits in the health facility (Table 1).
Sociodemographic characteristics of mothers of reproductive age in Ethiopia, data from EDHS 2019 (n = 5,753).

EDHS: Ethiopian Demographic and Health Survey; TBA: traditional birth attendant; SNNP: Southern Nation Nationalities and People.
Utilization of TBAs among mothers of reproductive age in Ethiopia
This study revealed that the prevalence of utilization of TBAs among mothers of reproductive age in Ethiopia was 34.59% with a 95% CI (33.35%– 35.83%) (Figure 1).

Prevalence of utilization of traditional birth attendants among mothers of reproductive age in Ethiopia, EDHS 2019 (n = 5,753).
Spatial autocorrelation of TBA utilization in Ethiopia
The spatial distribution of utilization of TBAs among reproductive age varied across the regions of Ethiopia. The result of the Global Moran’s index value was 0.39, which indicated that there was a significant clustering variation in the utilization of TBAs, with a p-value <0.001. Besides, the Z-scores of 8.66 also indicated a clustered variation in the utilization of TBAs among reproductive-age mothers across the regions of Ethiopia (Figure 2).

Spatial autocorrelation of traditional birth attendants among mothers of reproductive age in Ethiopia, EDHS 2019 (n = 5,753).
Spatial distribution of TBA utilization in Ethiopia, hotspot analysis
The highest number of TBAs was observed in the Somali, Afar, and Eastern parts of the Amhara and Oromia regions of the country. Furthermore, the spatial variation shows the hotspot areas of TBAs among mothers of reproductive age in Ethiopia. In this study, the utilization of TBAs observed among mothers of reproductive age was worse in the Somali and Afar regions, which were identified as hotspot areas of the country. However, Addis Ababa, Benshanul Gumuz, the central parts of Oromia, and Tiray regions were identified as cold spots in the country (Figure 3).

Spatial distribution hotspot analysis of traditional birth attendants among mothers of reproductive age in Ethiopia (n = 5,753).
Spatial interpolation of TBA utilization in Ethiopia
The ordinary Kriging interpolation analysis estimated and mapped the distributions of TBA utilization, interpolating the available data to the areas where data were not collected. The red-colored areas showed highly prevalent areas of TBAs among mothers of reproductive age, whereas the green-colored areas showed a low prevalence of utilization of TBAs among mothers of reproductive age in Ethiopia. The interpolation analysis predicted that TBAs were detected in the Somali, Afar, southeastern Oromia, and eastern parts of the Amhara regions (Figure 4).

Spatial interpolation of traditional birth attendants among mothers of reproductive age in Ethiopia (n = 5,753).
Spatial SAT scan statistical analysis of TBAs utilization in Ethiopia
The spatial SAT scan analysis identified 57 significant clusters, of which 27 were primary clusters/the most likely clusters, and 15 were secondary clusters. The primary SAT scan window was detected in eastern parts of Ethiopia at 6.639662 N, 44.465855 E, with a radius of 390.28 km.
In the primary cluster window, 695 people and 556 cases were included with a relative risk of 2.82 and a log-likelihood ratio of 346.4 at a p-value <0.0001. This indicates mothers of reproductive age in this spatial SAT scan window were 2.82 times at a higher risk of utilizing TBAs than mothers outside of the window. The secondary cluster window was detected at 9.720204 N, 40.270550 E, with a radius of 129.60 km. In this SAT scan window, a total of 332 populations and 246 cases were observed, with a relative risk of 2.3 and a log-likelihood ratio of 114.8 at a p-value of <0.001, which indicates reproductive mothers in this window were 2.3 times at a higher risk of utilizing TBAs as compared to mothers outside of this window (Table 2 and Figure 5).
Spatial SAT scan analysis of traditional birth attendants among mothers of reproductive age in Ethiopia, EDHS 2019 (n = 5,753).
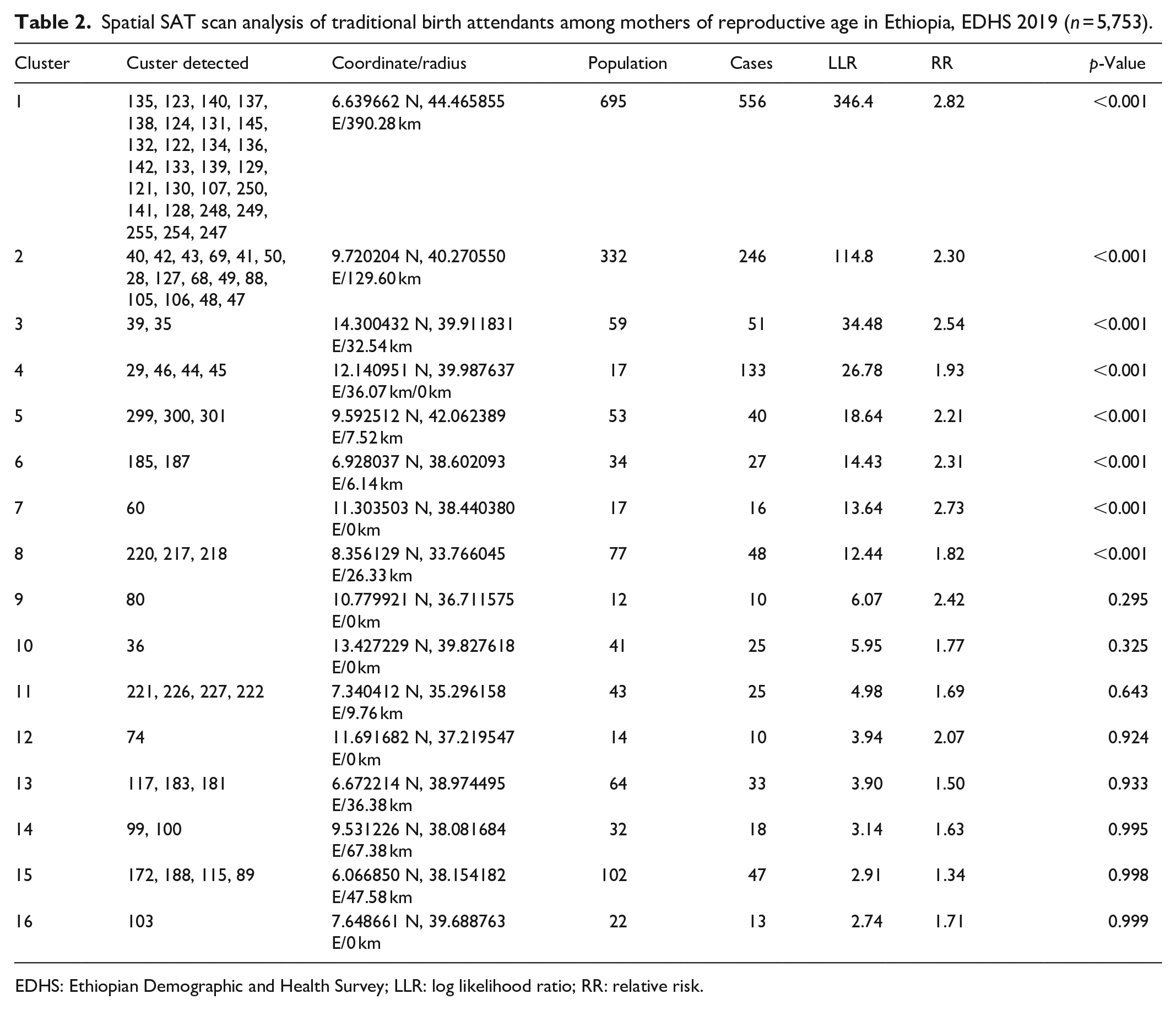
EDHS: Ethiopian Demographic and Health Survey; LLR: log likelihood ratio; RR: relative risk.

Spatial interpolation of traditional birth attendants among mothers of reproductive age in Ethiopia (n = 5,753).
Random effect and multilevel analysis of the determinant factors of TBAs in Ethiopia
The total variation in TBAs among mothers of reproductive age in the 2019 EDHS was attributable to clustering. The clustering effect is shown in the Table 3, which is directed to conduct multilevel analyses to determine the factors associated with TBAs among mothers of reproductive age.
Random effect analysis and multilevel analysis of factors associated with TBAs among women of reproductive age in Ethiopia, EDHS 2019 (n = 5,753).

EDHS: Ethiopian Demographic and Health Survey; TBA: traditional birth attendant; SNNP: Southern Nation Nationalities and People; ICC: intra-class correlation coefficient; PCV: proportional change in variance; MOR: median odds ratio; LLR: log likelihood ratio.
Statistically significant at a p-value <0.05.
In this study, a multilevel analysis was carried out to identify factors affecting TBAs among mothers of reproductive age and presented with an AOR and 95% CI.
At the individual/household level, the significant factors associated with TBAs utilization were age of mothers: 25–34 years old (AOR = 1.2; 95% CI (1.01–1.44)), 35–49 years old (AOR = 1.31; 95% CI (1.04–1.63)), maternal education: no education (AOR = 4.12; 95% CI (2.90–5.79)), primary education (AOR = 2.89; 95% CI (1.63–3.22)), wealth index: poorest (AOR = 7.2; 95% (4.82–10.51)), poorer (AOR = 5.64; 95% CI (3.82–8.32)), middle (AOR = 4.98; 95% CI (3.38–7.34)).
At the community level, the significant factors associated with TBA utilization were rural residence; mothers from rural residence were 9.1 times more likely to utilize TBA as compared to urban mothers (AOR = 9.1; 95% CI (5.44–15.2)), community illiteracy level (AOR = 1.8; 95% CI (1.53–2.14)), community poverty level (AOR = 1.4; 95% CI (1.22–1.72)), and the regions: Somali (AOR = 15.5; 95% CI (7.40–27.53)), and Afar (AOR = 9.8; 95% CI (3.28–29.59)).
In multivariable multilevel analysis, the significant factors associated with TBAs’ utilization were maternal education, wealth index, place of residence, and regions.
Reproductive mothers who had no formal education were 3.04 times more likely to utilize TBAs as compared to educated mothers (AOR = 3.04; 95% CI (2.13–4.33)).
Regarding the wealth index, the highest odds of TBA utilization was observed among the poorest households (AOR = 2.76; 95% CI (1.83–4.19)). Mothers from the poorest households were 2.76 times more likely to utilize TBAs as compared to mothers from the richest households. Another significant factor associated with TBAs was place of residence (AOR = 5.69; 95% CI (3.35–9.67)); rural mothers were 5.69 times more likely to utilize TBAs as compared to urban mothers.
Among the regions, the highest odds of TBA utilization were observed in Somali (AOR = 12.1; 95% CI (4.99–25.68)) and Afar (AOR = 7.13; 95% CI (2.37–21.38)). Mothers from the Somali region were 12.1 times more likely to utilize TBA, and mothers from Afar were 7.13 times more likely to utilize TBAs as compared to the other regions (Table 3).
Discussion
Traditional birth attendance among mothers of reproductive age in Ethiopia was a common practice. It is an important indicator of health care quality, the country’s health care system, and economic development. The utilization of TBAs among mothers of reproductive age is also a crucial indicator of maternal morbidity and mortality, as well as poor maternity care. This study presented the geospatial variation and determinant factors of the utilization of TBAs among mothers of reproductive age in Ethiopia, based on data from EDHS 2019. This study revealed that the prevalence of utilization of TBAs among mothers of reproductive age in Ethiopia was 34.59% with a 95% CI (33.35%–35.83%) in the 2019 national survey. In this study, the prevalence of TBA utilization among mothers of reproductive age was higher than in other studies conducted in Angolella Tara Ethiopia (31.5%) 22 and Dega Damot Ethiopia (5.4%). 26 This discrepancy might be because our study was conducted based on EDHS data with a large sample size and included the most affected regions of the country, like Afar and Somali, whereas the other studies stated above were conducted on a small sample size and covered a certain community. The utilization of TBA among mothers of reproductive age was influenced by many sociodemographic and socioeconomic factors at the individual, community, and multilevel variables. The burden of TBA utilization and its determining factors have geospatial variations among the regions of the country. Mothers’ ages were one of the determinants positively associated with TBAs. Those mothers of older age groups were more likely to utilize TBAs during childbirth as compared to mothers of younger age groups. This finding was in line with other studies conducted in Kenya 27 and Nigeria. 28 The possible reason for this finding might be that older women often perceive TBAs as respectful, skilled, friendly, trustworthy, and available when needed. They believe TBAs have enough midwifery knowledge and skills to assist during labor and childbirth. It also might be due to sociocultural norms and attitudes toward TBAs because cultural norms and beliefs toward TBAs mainly affect older women as compared to younger women. 29 On the contrary, younger women are usually able to access social media and information related to reproductive health, and opposes traditional activities. Promoting women’s attitudes toward facility-based delivery services and strengthening the maternal health care system could address these preferences and promote safer childbirth practices.
Another factor affecting the utilization of TBAs was maternal education. Uneducated mothers had higher odds of utilizing TBAs compared to educated mothers. This finding was supported by other studies conducted in Bench Maji Zone, Ethiopia, 30 Nigeria, 21 and sub-Saharan Africa. 31 This finding was indicative that formal education plays an important role in a mother’s reproductive health-informed decision-making. Uneducated mothers may not be aware of the benefits of skilled birth attendance in health facilities. In addition, uneducated mothers may face financial constraints, making it difficult for them to access formal healthcare services. In fact, education improves women’s health-seeking behaviors. This might be due to the fact that education helps mothers access essential information needed to get reproductive health services for themselves as well as for their babies, starting from antenatal care follow-up up to postnatal care services. 32 Mother’s education also helps to avoid traditional beliefs and TBAs. Education empowers mothers to make informed choices, seeks timely healthcare, and ensures better outcomes for themselves and their children.
This study found that the household wealth index significantly influenced the utilization of TBAs among mothers of reproductive age. The odds of utilizing TBAs were higher among mothers from the poorest households compared to those from the richest households. This finding was supported by other studies conducted in southwest Shoa Ethiopia, 33 Zambia, 29 and Nigeria 21 and selected sub-Saharan African countries. 34 This might be due to the fact that better household wealth status can access adequate health care services, including in private health institutions; access to transportation to health institutions for follow-up and health care visits, a good lifestyle easily improves the health of pregnant mothers, and better access to health-related information. It’s important to consider socioeconomic factors when designing maternal and child health interventions to ensure equitable access to healthcare services.
The findings of this study showed that there was no association between religion and TBA utilization during childbirth. But other studies conducted in Cameroon showed that there was an association between religion and birth service utilization. 35 Evidence has shown that mothers who are traditionalists are less likely to utilize skilled birth attendants due to their high inclination toward their traditional beliefs, spiritual practices, and religious norms prior to receiving health facility services.
Among the community-level variables, place of residence was significantly associated with TBA utilization. Reproductive-age mothers who live in rural areas were nine times more likely to utilize TBAs during childbirth as compared to those mothers who live in urban areas. This finding was in agreement with other studies conducted in western Ethiopia,36,37 Kenya, 27 sub-Saharan African countries, 31 and Afghanistan. 38 According to previous studies, living in rural areas has a negative effect on maternal health care accessibility due to the distance and means of transportation constraints for rural mothers. 39 This might be due to the fact that rural areas often have limited access to formal healthcare facilities, including hospitals and clinics. Therefore, rural mothers need to travel long distances on foot or pay a lot of money for transportation to seek maternal health care services, so most mothers prefer to deliver at home, assisted by TBAs. In general, access to healthcare facilities, cultural norms, geographical challenges, cost considerations, and lack of awareness hinder rural women from attending health facility deliveries. 40 Efforts to improve maternal healthcare should focus on addressing these challenges and promoting evidence-based practices.
The spatial variation analysis in this study showed that there were regional variations in the burden of utilization of TBAs. Mothers of reproductive age from Somali and Afar regions had higher odds of TBA utilization as compared to the Addis Ababa and Gambela regions. Somali, Afar, and some parts of SNNP regions were identified as hotspot areas, whereas Addis Ababa, central Oromia, Dire Dawa, and Harari regions were identified as cold spots in the country. This finding was supported by other studies.37,41 The possible reason might be due to cultural influence and the limitation of infrastructure.
This might also be due to the fact that Somali and Afar regions have a higher burden of utilization of TBA in reproductive-age mothers because of the geographically hot temperate and lowland nature of those regions; there are inadequate health facilities, inadequate infrastructure, and poor access to healthcare services, and their health care practices depend on their cultural beliefs and traditional norms, whereas Addis Ababa (the capital city of the country) and other regions have had a relatively lower burden of utilization of TBA in reproductive-age mothers. This might be due to the fact that the population can easily access maternal health care services, health-related information, and other infrastructure as compared to the population of Somali and Afar regions. Acknowledging these spatial disparities is important for effective health policy development and equitable maternal and child healthcare delivery. 42
The findings of this spatial analysis study were alarming and highlighted the worsening situation of maternal health service problems among mothers of reproductive age in Ethiopia, particularly in the Somali and Afar regions of the country, which was the most affected areas by TBA in opposition to health facility maternal care services. Therefore, it is highly recommended to take appropriate measures to bring reproductive mothers to the health facility by improving access to health care services in the rural and most affected regions of the country.
Strengths and limitations of the study
This study was conducted based on a large and nationally representative data set. The study employed advanced statistical analysis like random effect analysis, fixed-effect multilevel analysis, and spatial variation analysis. This approach allows for understanding regional variation and hotspot identification. It is also important to get more informative and intervention-based findings. However, due to the community-based nature of the data, obstetric-related factors and TBAs level of skill-related factors were not included in this study. Due to the cross-sectional nature of the study, some variables that were aggregated at the community level might potentially mask within-community variations. In addition, since this study was based on secondary DHS data, the power analysis for sample size calculation was not considered. Future researchers can address the limitations to enhance maternal health outcomes.
Conclusions
The prevalence of TBA utilization among reproductive-age women remains a significant public health concern, with geospatial disparities across Ethiopia. Hotspots for TBAs are predominantly observed in the Somali and Afar regions. Factors associated with the utilization of TBAs include maternal age (higher odds among older women), educational level (higher odds among uneducated women), wealth index (higher odds among poorer households), and regional variations (highest odds in Somali and Afar regions). Therefore, promoting maternal health education for older women, improving maternal educational status, designing interventions for poorer communities and hotspot regions, and improving strategies for maternal antenatal care services are essential to reducing TBA utilization and its health consequences. Understanding geospatial distribution informs targeted strategies to promote maternal health services and reduce reliance on TBAs.
Footnotes
Acknowledgements
The authors acknowledged the Demographic and Health Survey administrators for granting the data.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Data sharing statement
All data are available upon request. The reader could contact the corresponding author for all the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
This study was based on secondary data analysis of publicly available national survey data from the DHS program. Ethical approval and participant’s consent were not necessary for this particular study. We requested permission to download the DHS program, and it was granted. It uses data from ![]() . The Institution Review Board-approved procedures for DHS public-use datasets do not in any way allow participants, households, or sample societies to be identified. The names of individuals or household addresses in the data file were not stated. Each enumeration area primary sampling unit has a number in the data file, but the numbers do not have any labels to indicate their names or locations.
. The Institution Review Board-approved procedures for DHS public-use datasets do not in any way allow participants, households, or sample societies to be identified. The names of individuals or household addresses in the data file were not stated. Each enumeration area primary sampling unit has a number in the data file, but the numbers do not have any labels to indicate their names or locations.
Consent for publication
Not applicable.
Informed consent
Not applicable.
Trial registration
Not applicable.