
Abstract
Objectives:
The goals of benign parotid gland tumor resection are complete resection of the lesion and preservation of the facial nerve function. As the facial nerve cannot be directly visualized via imaging modalities, several methods, including the facial nerve line, Utrecht line, retromandibular vein, Stenon duct, and minimum fascia-tumor distance techniques, have been developed to estimate its location. However, there are no reports on their accuracy in determining tumor location. In the present study, we aimed to assess the diagnostic accuracy of these methods based on tumor location.
Methods:
This retrospective study analyzed medical records and histological reports of 359 patients with various types of benign parotid gland tumors who underwent a parotidectomy between April 2014 and March 2020. The tumor location was subdivided into the following sections: anterior, superior, inferior, and middle. The tumor location was estimated using five methods: facial nerve line, Utrecht line, retromandibular vein, Stenon duct, and minimum fascia-tumor distance. The final diagnosis of superficial or deep lobe tumor was made based on surgical findings.
Results:
Each method showed a higher accuracy for superficial tumors (was more than 90%) than for deep lobe tumors. In contrast, for deep lobe tumors, the accuracy of diagnosis with the facial nerve line, Utrecht line, and retromandibular vein methods was low, in the 30% range. Among all methods, the Stenon duct method had the highest accuracy in the diagnosis of deep lobe tumors. The SD method was most useful in cases where both the duct and tumors were detected. The minimum fascia-tumor distance method had the second highest diagnostic accuracy (63%); however, for anterior tumors, it tended to provide false negatives.
Conclusions:
All tested methods were useful in diagnosing superficial lobe tumors; however, they were not helpful in diagnosing deep lobe tumors, especially anterior tumors.
Introduction
During surgery for benign parotid gland tumors, it is crucial to achieve complete resection while preserving facial nerve function. According to previous reports, the incidence of transient postoperative facial nerve paralysis ranges from 9% to 65% after parotid tumor resection. Tumors in the deep lobe have a higher risk of facial palsy, and in a previous study, approximately 11% patients with superficial lobe tumors had temporary facial nerve paralysis, compared to 34% patients with deep lobe tumors. 1 Therefore, it is very important to preoperatively evaluate the correct location of the parotid tumors in the superficial or the deep lobe to avoid facial nerve palsy and to estimate the operation time and risk of paralysis. The facial nerve, which divides the parotid gland into superficial lobe and deep lobe, cannot be directly visualized on imaging modalities in most cases, although the facial nerve can be visualized in modern magnetic resonance imaging (MRI) sequences, with the evolution of MRI. Therefore, evaluating the tumor location helps in estimating the relation between the tumor and the facial nerve. Several methods, including the facial nerve line (FN line), Utrecht line (UT line), retromandibular vein (RMV), Stenon duct (SD), and minimum fascia-tumor distance (MFTD) methods, have been tested to estimate if the tumor is located in the superficial or the deep lobe.2–6
Traditional radiological methods for estimation, such as the FN line, UT line, and RMV, have been popular for a long time, and many studies have been conducted using these methods. Since the MFTD method was proposed by Higashino et al., studies related to MFTD have increased. 6 Although the SD method has been previously reported, it has not been widely used because it cannot be confirmed in all cases. 5 Several studies have been conducted to compare the usefulness of multiple methods for preoperative assessments, but there have been no reports comparing all criteria at the same time, or even just a comparison of only 2 or 3 criteria. In addition, no reports have evaluated accuracy indicators based on tumor locations (superficial and deep lobe or anterior, inferior, middle, and posterior parotid). This study is the first to examine site-specific comparisons of all criteria. In the present study, we aimed to assess the diagnostic accuracy of these methods based on the tumor location.
Patients and methods
Patients
In this retrospective study, medical records and histological reports of 359 patients with various types of benign parotid tumors who underwent parotidectomy at our University Hospital between April 2014 and March 2020 were reviewed and analyzed. Patients with recurrences and histologically confirmed malignancies were excluded. These cases are difficult to evaluate correctly because the boundaries are often unclear. In addition, we experienced some cases of parotid malignancies involving the facial nerve, which make preoperative evaluation difficult. Therefore, we excluded malignancies in this study. None of the patients had undergone neck dissection. All patients were evaluated preoperatively using computed tomography (CT), MRI, ultrasonography (US), or fine needle aspiration cytology. Radiologic evaluations of tumor size and location were also reviewed. Tumor size was defined as the largest diameter on imaging findings.
Tumor location and measurement methods
The tumor location was subdivided into anterior, superior, inferior, and middle sections, following a previously reported method. 7 If the tumor was large, the tumor was classified according to the location of the center of the tumor. Whether the location of the tumor was in the superficial or the deep lobe was assessed using the following methods:
FN line
The line connecting the lateral surface of the posterior belly of the digastric muscle to the lateral surface of the cortex of the ascending ramps of the mandible was used as a reference on MRI, and tumors located superficial to this line were considered superficial lobe tumors (Figure 1).

The FN line, RMV, and UT line.
UT line
Tumors located superficial to the line running from the most dorsal point of the ipsilateral half of the first vertebra to the most dorsal point of the RMV on MRI were considered superficial lobe tumors (Figure 1).
RMV
The RMV branches off from the external jugular vein and can be easily identified using MRI. Tumors located superficial to the RMV were considered superficial lobe tumors (Figure 1).
SD
The SD can be visualized as a curvilinear structure within the parotid gland with hypointensity on T1-weighted and/or hyperintensity on T2-weighted images. Tumors located superficial to the SD were considered superficial lobe tumors. This method was only applied to cases in which both the tumor and duct were detected on the same axial MRI slice. When the duct was not visualized on any image, or when it was visualized on an image where the tumor was not seen, the location of the tumor was not evaluated (Figure 2). 8

The SD.
MFTD
The minimum distance between the parotid fascia and tumor was calculated using US. For our cases, based on the study by Cheng et al., 9 the cut-off value was set at 2.4 mm for superficial lobe tumors (Figure 3).

The MFTD.
Evaluation
The final diagnosis of superficial or deep lobe tumor was made based on surgical findings. The accuracy of diagnosis for each method was compared based on the tumor location.
Statistical analyses
Fisher’s exact test was used to evaluate the relationship between each group. A P value of < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 22.0.0, IBM, Armonk, NY, USA). This study was conducted using data obtained from electronic medical records of our institution.
Ethical statement
This study was approved by the local institutional review board (approval number: E21-0346-H01). The need for informed consent was waived off by the review board due to the retrospective nature of the study.
Results
Patient characteristics
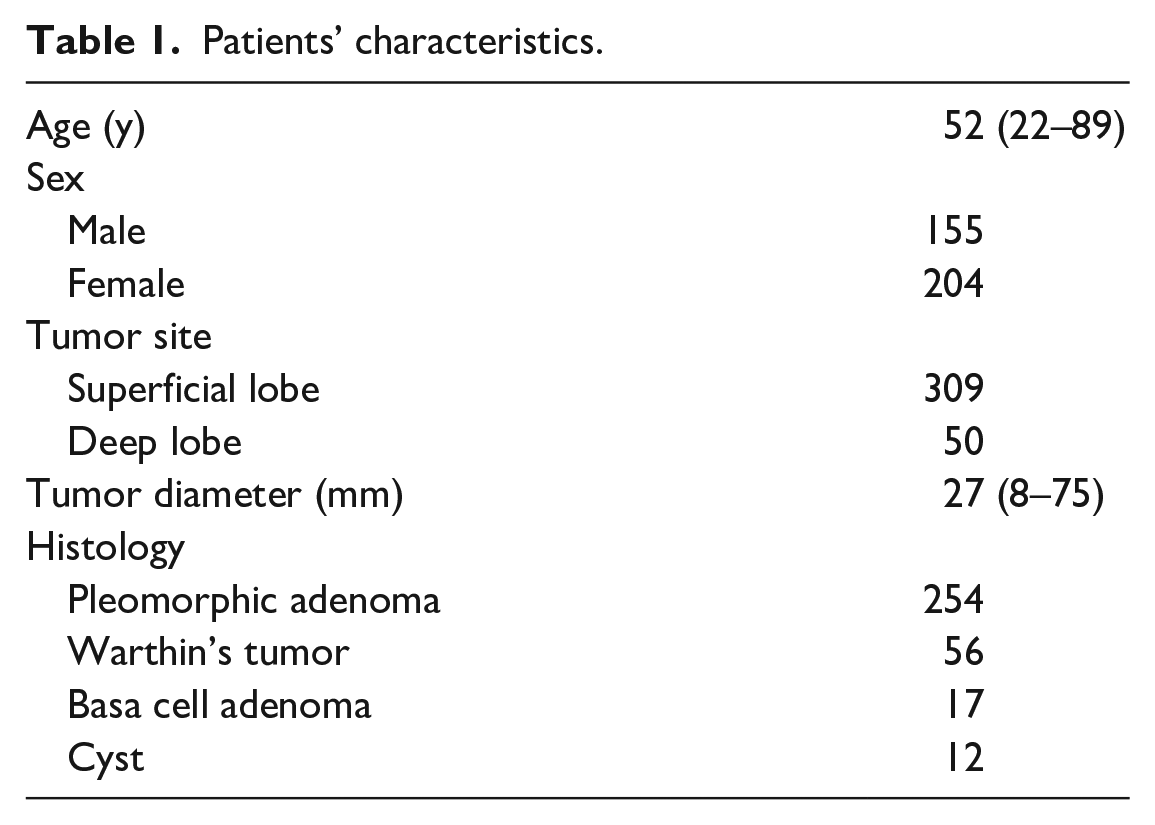
The patient characteristics are shown in Table 1. To correctly evaluate the tumor location using the FN, UT, RMV, and SD, an anatomical landmark and the tumor needed to be detected on the same axial MRI slice. Using the FN line, the posterior belly of the digastric muscle was not detected in some patients due to the presence of a large tumor. The UT line and RMV were not visualized on MRI in some patients because they were compressed by a large tumor. Regardless of tumor size, the SD was more difficult to visualize. US was performed for almost all the patients; however, there were no records. For these reasons, the number of cases was different among each method. The patients’ age during surgery ranged from 22 to 89 years. The median age of the patients was 52 years. The study included 155 men and 204 women. The average tumor size was 27 (range, 8–75) mm. Regarding histopathology, 254 pleomorphic adenomas (70.8%) and 56 Warthin’s tumors (15.6%) were included. A total of 309 patients had tumors in the superficial lobe, and 50 patients had tumors in the deep lobe. The most common location of the tumors was the middle portion of the superficial lobe (Table 2).
Patients’ characteristics.
Tumor location.

Accuracy of diagnosis according to methods
For the tumors diagnosed as superficial lobe tumors preoperatively, the diagnostic accuracy of all the methods was good and more than 90%, with no significant differences observed between these methods. In contrast, for the tumors diagnosed as deep lobe tumors preoperatively, the accuracy of all the methods was low, especially for the FN line, UT line, and RMV methods, which were in the 30% range. For anterior and deep lobe tumors, the accuracy of the above three methods was 0%; therefore, tumors located in the anterior lobe cannot be assessed accurately by these methods. The total preoperative diagnostic accuracy for deep lobe tumors using the SD and MFTD methods was 74.2% and 63.0%, respectively. The SD method had a significantly higher accuracy. Although the accuracy of the MFTD method for the superior and anterior deep tumors was 0% and the accuracy of the SD for the anterior deep lobe tumors was 42.8%, for the middle deep tumors, the SD and MFTD methods had a high accuracy (Table 3). There were no cases of superior deep lobe tumors identified using the SD methods.
Accuracy of diagnosis according to each criterion.
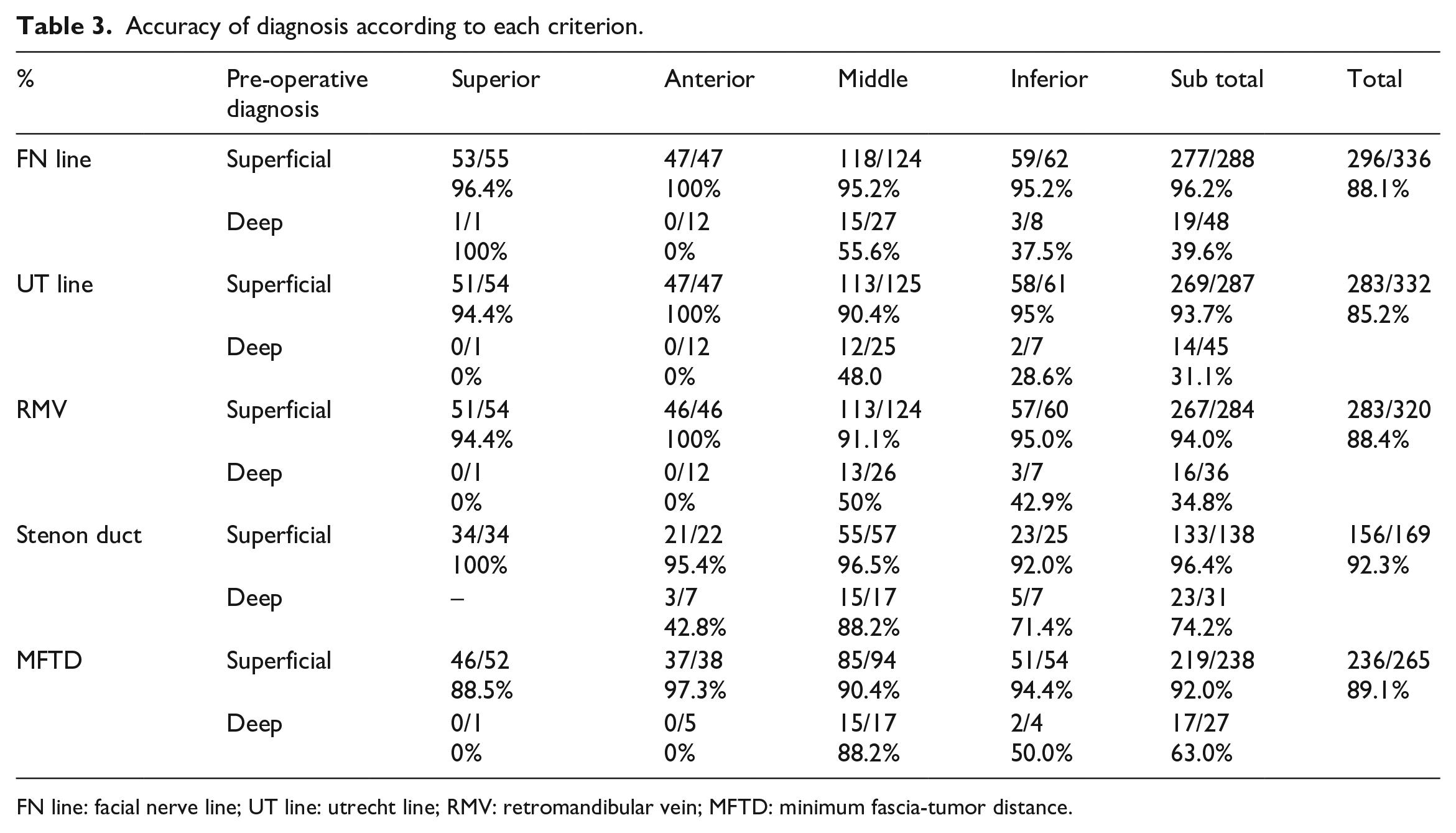
FN line: facial nerve line; UT line: utrecht line; RMV: retromandibular vein; MFTD: minimum fascia-tumor distance.
Discussion
In our study, for parotid tumors in general, all methods achieved a satisfactory accuracy of more than 85%. Lim et al. 10 compared the accuracy of the traditional radiological methods, including the FN line, UT line, and RMV, and the accuracy of each method in their study (85%, 94%, and 82% respectively) was comparable to our results. For superficial lobe tumors, the accuracy of diagnosis using any method was more than 90%, and these methods can be useful in clinical practice. The FN line was proposed by Som and Biller. The FN line has been reported to be useful in predicting tumor location because the mandible and digastric muscle are relatively fixed structures outside the parotid gland and are rarely displaced. Previous studies have shown an accuracy ranging from 63% to 85%. This method is well known and the oldest. 2 The UT line method was proposed by De Ru et al. and had an accuracy of 85.7% in identifying parotid tumor locations in 28 patients. However, it cannot always be used because the vein is not always visible on a CT scan. 3 The RMV method was proposed by Divi et al. 4 The RMV method is frequently used, but its usage can be greatly affected by the size of the tumor. The larger the tumor, the more difficult it is to see the veins because they are drained. Lim et al. 10 reported that if the tumor size was over 2.0 cm, the accuracy was markedly decreased.
In contrast, for the deep lobe tumors, the diagnostic accuracy of the FN line, UT line, and RMV methods was low (in the 30% range), and these were not useful for evaluating the tumor locations preoperatively. Of all the methods, the SD line had the highest accuracy in the diagnosis of deep lobe tumors. Richards et al. 11 found that the SD was always located just medial to the facial nerve branches, confirming that tumors located medial to the duct are deep lobe tumors. Eracleous et al. 12 reported that the SD was identified in 69% of cases on MRI. This method was only applied to cases in which both the tumor and duct were identified on the same axial MR image slice. The SD can be seen on both T1-weighted and T2-weighted images with fat saturation. Imaizumi et al. 8 reported that T2-weighted images are very useful because the difference in signal intensities between the duct and parotid parenchyma was enhanced. In our study, the SD with the parotid tumor was demonstrated on the same axial slice by MRI in approximately 47% cases. However, since the positive diagnosis rate of these cases was high, we considered that this method was the most useful in cases where both the duct and the tumors are visible. However, it cannot be used when the duct and tumor are not detected on the same axial slice. The MFTD method had the second highest diagnostic accuracy (63%). This method is cheaper and easier to use. Cheng et al. 9 reported that the advantages of US include low cost, easy use, real-time practice, no radiation exposure, and no need for contrast material injection. They suggested that US is sufficient for locating benign parotid tumors with a clearly defined margin, because the overall facial nerve paralysis rate was not significantly different from that of other benign superficial tumors when assessed using CT. US is the primary method used in diagnosis of parotid tumors. The shape of the parotid tumor can be clearly identified, and it is sometimes possible to approximately diagnose whether the tumor is benign or malignant. US is also helpful for diagnosis of superficial and deep lobe tumors and is a very simple method that only measures the shortest distance between the tumor and the parotid fascia. It can be used in almost all cases, making it a very useful method compared to others. MFTD, is a tool similar to CT and MRI, which can also be used for retrospective confirmation if the images are saved. In addition, this method does not require any difficult techniques. The only disadvantage is there can be differences in tumor positioning and soft tissue compression depending on the operator, but this should not be a problem if a certain level of skill is demonstrated. In our hospital, all cases are performed by head and neck specialists who have been practicing for more than 10 years. Unfortunately, in some cases, US results were not preserved, which is a limitation of this study. The MFTD was first proposed by Higashino et al., 6 who set a cut-off point of 3 mm. However, Cheng et al. 9 reported that more accurate results can be obtained with an optimal MFTD cut-off point of 2.4 mm; therefore, we chose 2.4 mm for our study. They reported that MFTD is useful for diagnosing benign tumors of the superficial lobe, but not for malignancy, and the tumor size is > 3 cm. In addition, they mentioned that the parotid tumors in false-negative cases tended to be located anteriorly. Therefore, the MFTD is not useful for diagnosing anterior tumors.
Regarding anterior and deep lobe tumors, although the SD had the highest accuracy among all methods (43%), it was not considered applicable in the evaluation of anterior tumors in clinical practice. All tumors located anteriorly were diagnosed as superficial lobe tumors using the FN line, UT line, RMV, and MFTD, except in 5 patients in the MFTD group. These methods had no diagnostic value for anterior and deep lobe tumors. As the facial nerve runs more anteriorly and more superficially in the parotid gland, the tumor is more likely to be located deeper than the facial nerve, even if the tumor is close to the skin surface. The proportion of anterior tumors that were deep lobe tumors was higher than that for superficial tumors. This may make the diagnosis more difficult, regardless of the method used. Thus, in the case of anterior tumors, the possibility that the tumor may be in the deep lobe should be considered, even if the preoperative diagnosis is superficial lobe tumor, regardless of the diagnostic method used. In those cases, a retrograde dissection of the facial nerve might be better than an antegrade dissection, as less nerve dissection would be required. On the other hand, in the posterior section of the parotid, a deep tumor is likely to require more nerve dissection and retraction. Therefore, we need to make a surgical plan depending on the location of the tumors.
The facial nerve is primarily identified using intraoperative monitoring equipment. The main trunk of the facial nerve is identified using the Pointer’s cartilage, the digastric muscle, and the mastoid process as landmarks. Basically, the same surgical approach is used for both superficial and deep lobe tumors. However, if the superficial or deep lobe tumors are determined preoperatively, the extent of facial nerve travel can be predicted intraoperatively and the facial nerve can be identified more quickly. In addition, since deep lobe tumors require a longer operative time, this involves surgical planning for the day, and the possibility of postoperative facial nerve palsy should be strongly considered. Therefore, it is very important to identify superficial or deep lobe tumors before surgery. In the case of an obvious superficial lobe tumor, extracapsular dissection may be an option. Extracapsular dissection is less invasive because the facial nerve is not dissected, and the operative time can be shortened. However, in cases with deep lobe tumors, the facial nerve is susceptible to further injury, thus requiring careful selection. In cases with anterior tumors, as mentioned above, the possibility of deep lobe tumors is higher, and this requires more careful judgment.
This study had some limitations. First, although this study had a relatively large number of cases, it was a retrospective study. Second, the sample size was not calculated. Further prospective studies evaluating ethical outcomes are warranted to clarify the usefulness of these methods in the preoperative diagnosis of tumor location within the parotid and to establish possible novel methods.
Conclusion
All these methods are useful in diagnosing superficial lobe tumors; however, they are not very helpful in diagnosing deep lobe tumors, especially anterior tumors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This retrospective analysis was approved by the ethics committee of Juntendo University (approval number: E21-0346-H01).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for the present study because *The need for informed consent was waived off by the review board due to the retrospective nature of the study*.