
Abstract
Objectives:
To assess intimate partner violence and health system response among married women.
Methods:
A mixed method of quantitative and qualitative cross-sectional community-based study was conducted from August to September 2019. Later than ethical clearance, the data were collected using a pretested structured questionnaire adapted from the literature. Study participants were selected using systematic random sampling. Data collected is entered into EpiData and then exported to SPSS version 25 for analysis. The odds ratio with their 95% confidence interval was calculated. Variables with p-value < 0.25 in bivariate analysis were entered into multivariate logistic regression. Statistical significance was declared if the p-value was <0.05.
Results:
From all 770 sampled participants in Nekemte town, 730 married women participated in this study, yielding a response rate of 94.8%. The prevalence of intimate partner violence was 55.9%. From this study finding, no intimate partner violence screening was done for 678 (92.9%) respondents who visited health facilities. Educational status of women, partner being illiterate, occupational status being merchant, and daily laborer were associated with intimate partner violence with (adjusted odds ratio = 1.73, 95% confidence interval = (1.05–2.83)), (adjusted odds ratio = 5.94, 95% confidence interval = (1.25–12.23)), (adjusted odds ratio = 4.41, 95% confidence interval = (1.49–13.01)), and (adjusted odds ratio = 3.74, 95% confidence interval = (1.33–10.50)), respectively, were factors found to be associated with intimate partner violence Nekemte town. One of the study participants whose age was 36 years responded that, “our culture approves men’s superiority; we accept intimate partner violence as part of our marital life.” There is an assigned focal person and training was given to them, but screening of intimate partner violence has not started yet and it was not integrated into any maternal service in our health center.
Conclusion:
This study shows that in excess of half of women experience intimate partner violence. Educational status, occupation and violence seen during childhood were the factors that contributed to intimate partner violence. Educating women and partners, integrating, and strengthening a health service are important.
Introduction
Violence is defined as the intentional use of physical force or power, threats against a person, a group or community that results in injury, death, psychological harm, either maldevelopment or deprivation. 1 Although domestic violence (DV) against women, also known as intimate partner violence (IPV), is widely recognized as serious human rights abuse, and as an important public health problem with substantial consequences for women’s physical, mental, sexual, and reproductive health, the health system is not adequately addressing the problem of violence and contributing to comprehensive multisector response often. 2 Victims of IPV exhibit chronic physical and emotional health symptoms, injuries sustained, and even are at risk of death from homicide. 3
Globally, almost one-third (30%) of women who have been in a relationship report that they have experienced some form of violence by their intimate partner. 4 According to the National Intimate Partner and Sexual Violence Survey (NISVS), women’s lifetime experiences of sexual violence, physical violence, and/or irritation was reported to be 36% in the United States, and 48% of them have experienced at least one form of psychological aggression in the form of expressive aggression, or coercive control. 5
Another study in Uganda reported that about 24% of 15–49 women said their first sexual intercourse was forced against their will and almost 39% of women have ever experienced sexual violence. 6 A study among Kenyan women revealed that the rates of exposure to emotional, physical, and sexual violence were 24%, 38%, and 14%, respectively. 7 Ethiopia has the highest rates of IPV compared to the 10 countries in the study. About 53.7% of Ethiopian women had experienced IPV within 1 year preceding the interview and 70.9% over their lifetime. 8
Ethiopia is a culturally diverse country with institutionalized gender roles and structural power imbalances between women and men. The 2016 Ethiopian Demographic and Health Survey (EDHS) reported that wife beating is justified, which indicates that it is socially acceptable. 9 For everyone who dies because of violence, more were injured and suffer from a range of physical, sexual, and emotional health problems. 10 At a global level, IPV has been linked to a range of physical and mental health problems that may persist long after violence has ended and can lead to poor physical, emotional, sexual, and reproductive health outcomes. 11
In Africa, women are often sexually harassed, victimized, suffer physically, psychologically, and are unable to make their own decisions or protect themselves and their children because they fear their partner and other families due to deep-rooted socio-cultural and economic factors. As a result, some have contracted HIV/AIDS and other sexually transmitted diseases (STIs) since they cannot tell their partners when to use condoms and women lack power over their sexual rights. 12
Study done in Butajira reported that sexual violence occurs more than physical violence and perpetrators of this violence were mainly intimate partners and close family members. 13 In Ethiopia, specific programs and services represent principally the major disease and services vertical programs that are developed to some extent outside of the regular system, from those programs, gender and women’s health was included. 14
A study done in Tsegede district of North Ethiopia shows, IPV interventions are complex, requiring more than one healthcare provider training to enable effective program functioning within a health system. However, the evidence informed that the scale of IPV interventions and their integration into health systems are lacking. 15 Since healthcare professionals are often “the first-line response” for many people who experience IPV, it is vital to have education, policies, and protocols in place so that they can identify and record incidents of IPV and assist victims with getting the services and support they need. 16
A spouse, ex-spouse, or current or former boyfriend may commit IPV, and result in physical, sexual, and emotional violence and contribute to the ill health of women. There is poor understanding or acceptance within the health programs of the critical role that the health system and health care providers can play in terms of identification, assessment intervention, documentation, referral, and follow-up, including Ethiopia. This study aimed to assess the magnitude and identify contributing factors associated with IPV, as well as explore the health system responses toward IPV among married women in Nekemte town, Western Oromia, Ethiopia, 2019.
Methods and materials
Study area
The study was conducted in Nekemte town, which is located in Western part of Oromia, located 334 km from Addis Ababa of Ethiopia. Nekemte city covers 5480 km2 land. Nekemte town has seven sub-cities. They are Darge, Cheleleki, Keso, Bake-Jema, Burka-Jato Sorga, and Makanisa-Kese, with a total population of 127,380. From these 65,066 males and 62,514 females, and women in child bearing age is 28,151 and the total household (HH) of the town is 26,538. Nekemte has one specialized hospital, one teaching hospital, and two governmental health centers.
Study period
The study was conducted from August to September 2019.
Study design
It is a mixed quantitative and qualitative community-based cross-sectional study.
Source population
All married women living in the HHs of Nekemte town.
Study population
All married women lived in randomly selected houses during the study period.
Inclusion and exclusion criteria
Inclusion criteria
All married women who live in selected HHs for 6 months and above were included in the study.
Exclusion criteria
Women who were critically ill and temporary residents (less than 6 months) were excluded.
Variables
Dependent variables
The dependent variables are IPV and health system response.
Independent variables
Socio-demographic factors
It includes age, religion, educational status, occupational status, age at first marriage, and family history of violence,
HH factors
It includes family size, number of children, economic position, discussion about sexuality openly, and decision-making power.
Socio-cultural factors
It includes marriage tradition, marriage type (poly or monogamy), and community attitude toward IPV.
Sample size determination
The required sample size eligible for the study was determined using the single population proportion formula

where p is the prevalence/population proportion of IPV (taken from EDHS 2016 17 ), which is 35% (p = 0.35), Zα/2 = 1.96 (95% confidence interval (CI)), and d = 5% (0.05).
Therefore
With calculation of design effect, that is, two times the actual sample sizes = 700. In addition, adding 10% for non-response rate, then the sample size is 770.
For quantitative data
For the purpose of this study, 770 participants in the study area were considered.
For qualitative data
Nineteen individuals participated in an in-depth interview among 19-selected key informants. They include two health managers, two directors, four health workers, two women affairs, four health extension workers, two legal persons, and three from victims of IPV. In addition, document review was done at registrations, referral protocols and guidelines, plan and report, training given, materials and integration of IPV to health service at health facilities to explore specific factors associated with IPV, and status of health system in responding to IPV.
Sampling procedure
Nekemte town is composed of seven sub-cities among which four sub-cities were selected for this study by simple random sampling (lottery method), Then, HHs for the study were selected using multistage sampling. The study participants were proportionally assigned to each zone according to their HH size. Then, systematic random sampling was applied to select HHs for each zone (taking a proportionate sample of the HH size of each zone, which is taken from Nekemte town administration offices as a sampling frame of zone, respectively).
Since K-value is proportionally allocated, the K-value is calculated as 2227/770 = 2.8 ≈ 3, then the first HH was selected by lottery method from 1 to 3, and then based on the selected number, it continued every three HHs in each selected zone.
Data collection instrument, procedure, and measurements
Structured questionnaires were adopted based on the 2005 standard World Health Organization (WHO) multicountry study on women’s DV 18 and additionally considering different literatures in line with the objectives of the study. 19
The data were collected through structured questionnaires that were prepared in English and were translated to Afan Oromo, and then the questionnaire was pretested on 5% of the sample size in Cheleleki sub-city 1 week prior to actual data collection.
Data quality management
To assure quality, the following measures were taken; training was given to the data collectors and supervisors for 2 days, pretesting the questionnaire and close supervision during data collection. Study participants were clearly informed about the purpose and usefulness of the study, to create a friendly atmosphere to lessen their stress as the study touches sensitive and critical issues. In addition, female data collectors and those previously exposed to collecting similar data were recruited to reduce the non-response rate and to ensure confidentiality of the participants. Reviewing and checking filled questionnaires on a daily basis during data collection and any incorrectly filled or missed question was addressed daily during data collection.
Operational definitions
IPV
It was defined as physical sexual or emotional violence by an intimate partner during the last 12 months before the study and during their lifetime.1,20
Physical violence
It meant the woman had been slapped, or had something thrown at her; pushed or shoved; hit with a fist or something else that could hurt; kicked, dragged, or beaten up; choked or burnt; threatened with or had a weapon used against her.1,20
Sexual violence
It meant the woman had been physically forced to have sexual intercourse; had sexual intercourse because she was afraid of what her partner might do; been forced to do something sexual she found degrading or humiliating; ignored by her partner to have sexual intercourse.1,20
Emotional (psychological) violence
It includes violence such as insults, belittling, constant humiliation, intimidation (e.g. destroying things), and threats of harm.1,20
Health system response
It was defined as availability of guidelines, protocols or standard of procedures, training, service integration, screening, counseling, assigned health care provider and separate room for survivor’s IPV. In addition, availability of equipment and other supplies, a budget allocated for provision of care, referral systems in place across different health services and between health and other sectors, and availability of plans and reports. 19
Positive attitude
It is the disbelief that a good wife is obedient to her husband even if he does not agree with her opinions and it is good for a man to show his partner that he is the boss.
Negative attitude
It is the belief that a good wife is obedient to her husband even if he does not agree with her opinions. In addition, it is good for a man to show his partner that he is the boss.
Statistical analysis
The collected data were checked visually for completeness, coded, and entered into EpiData version 3.1 and was exported to SPSS version 25.0 for analysis. p-value < 0.05 at 95% CI was considered statistically significant.
Descriptive statistics such as frequency, percentage, mean, and median were applied to different variables; binary logistic regressions and multivariate analysis were carried out. Significance level and association of variables were tested using a 95% CI and odds ratio. For the analysis of the qualitative data, the written notes taken during the time of the in-depth interview were translated into English. Thematic analysis was done to describe the exploratory ideas obtained from the in-depth interview and document reviews. By doing so, the information was reduced into manageable ideas. Finally, the qualitative findings were integrated with the quantitative results to give complete ideas about the contributing factors and health system response to IPV in the study area.
Patient and public involvement
Data collectors and PIs inform priorities, experience, and preferences on research questions and outcome measures. The results were disseminated through the city health office.
Result
From 770 samples, 730 women participated in this study succumbed a response rate of 94.8%. The mean age of women participating in the study was 29.9 years with a standard deviation of ±7.03 years, and the majority 432 (59.2%) of the respondents were between 25 and 34 years. According to the information from the interviewed respondents, the mean ages of the husbands/partners were 34.8 years and a standard deviation of ±7.56 years. Majority 357 (48.9%) of respondents’ partners were between the age of 25 and 34 years. Among study participants, more than half of them, 422 (57.8%) were housewives and employees; there were 132 (18%).
About one in ten, 136 (18.6%) of partners had no formal education. Regarding occupation, 28.7% and 26% of partners were government employees and merchants, respectively. Concerning women’s educational status, about 241 (33%) attended formal education and only 88 (12.1%) attended college and above. Regarding the marital status of the respondents, 678 (92.9%) were married and living together with their husbands, whereas the rest of 32 (4.4%) were divorced and 20 (2.7%) were widowed. The socio-demographic characteristics of the study subjects are summarized in Table 1.
Socio-demographic characteristics of women and their partner.

Partners’ characteristics
According to the report from the interviewed respondents, more than one in ten, 79 (10.8%) of the partner’s have another wife. About 270 of the partners (36.9%) drink alcohol, and 17.9% and 16% of the partners chew khat and smoke tobacco, respectively (see Table 2).
Partners’ characteristics.

Women-related characteristics of married women and their partner
In this study, 291 (39.9%) of the respondents lived in marital relation for more than 11 years, and 192 (26.3%) of them lived in marital relation for 1–5 years. From 770 participants, 198 (27.1%) of them seen violence during childhood (Table 3).
Women’s and partners’ characteristics.

Socio-cultural characteristics
The findings of this study show, marriage arrangements of respondents indicate that about 493 (67.5%) were arranged by agreement of both women and men, while 135 (18.5%) were family involvement. Also, in this study, 277 (37.9%) of the women agree that a good wife is obedient to her husband even if he does not agree with her opinions, while 189 (25.9%) of them agree that it is good for a man to show his partner that he is the boss.
In a qualitative study, health managers, health workers, women’s affairs, legal people, and victims of IPV participated. Qualitative data analysis reveals that most of them responded that the main problem regarding IPV was community attitude. Even though there is improvement from previous community attitudes toward IPV, it should be changed. Still, the superiority of men is seen, IPV is not considered a problem since, socially, they accept it. However, it seems to have improved due to different reasons that may be educating women and employing women has been improved from previous. The strategies they recommended to combat these problems were as follows: educating women, giving awareness, focusing on communities’ attitudes, strengthening legal issues, integrating the service into health services given at health facilities, strengthening women’s economy, and specially giving awareness to men. One of the study participants whose age was 36 years responded that, our culture approves men’s superiority; we accept intimate partner violence as part of our marital life. Because we grow by observing our parents’ violence during childhood and some proverbs like “gaangee fi haadha manaa abbaatu sirreeffata” mean that horse and wife is as owner trained them. So all concerned body should be act on IPV.
Also said “this proverb direct the man can manage women at the style he wants she cannot disobey him” (Table 4).
Socio-cultural characteristics.

HH characteristics
According to this study, about 48 (6.6%) of women participated have no child, while 72 (9.9%) of them have five or more children. About 371 (50.8%) of them do discuss openly about sexuality while 359 (49.2%) of them do not discuss (Table 5).
Household characteristics.

Prevalence of IPV
Prevalence of IPV during lifetime
In this study, the prevalence of IPV was 55.9% during the lifetime in which 408 of the total study participants were violated physically, emotionally, or sexually. From this, about 358 (49%) of women face emotional violence while 254 (34.8%) physical and 242 (33.2%) of women face sexual violence during their physical lifetime.
According to qualitative data from study participants of health facilities, they said that knowing the status of IPV is difficult because it is a sensitive women fear to disclose to maintain their relationship with their husbands, and IPV is not considered a problem, since socially they accept it. However, it is deep-rooted and seen in every HH in our community. All forms of violence during lifetime were described in Figure 1.

Forms of intimate partner violence among married women, in Nekemte town, Western Ethiopia, 2019.
Sexual violence
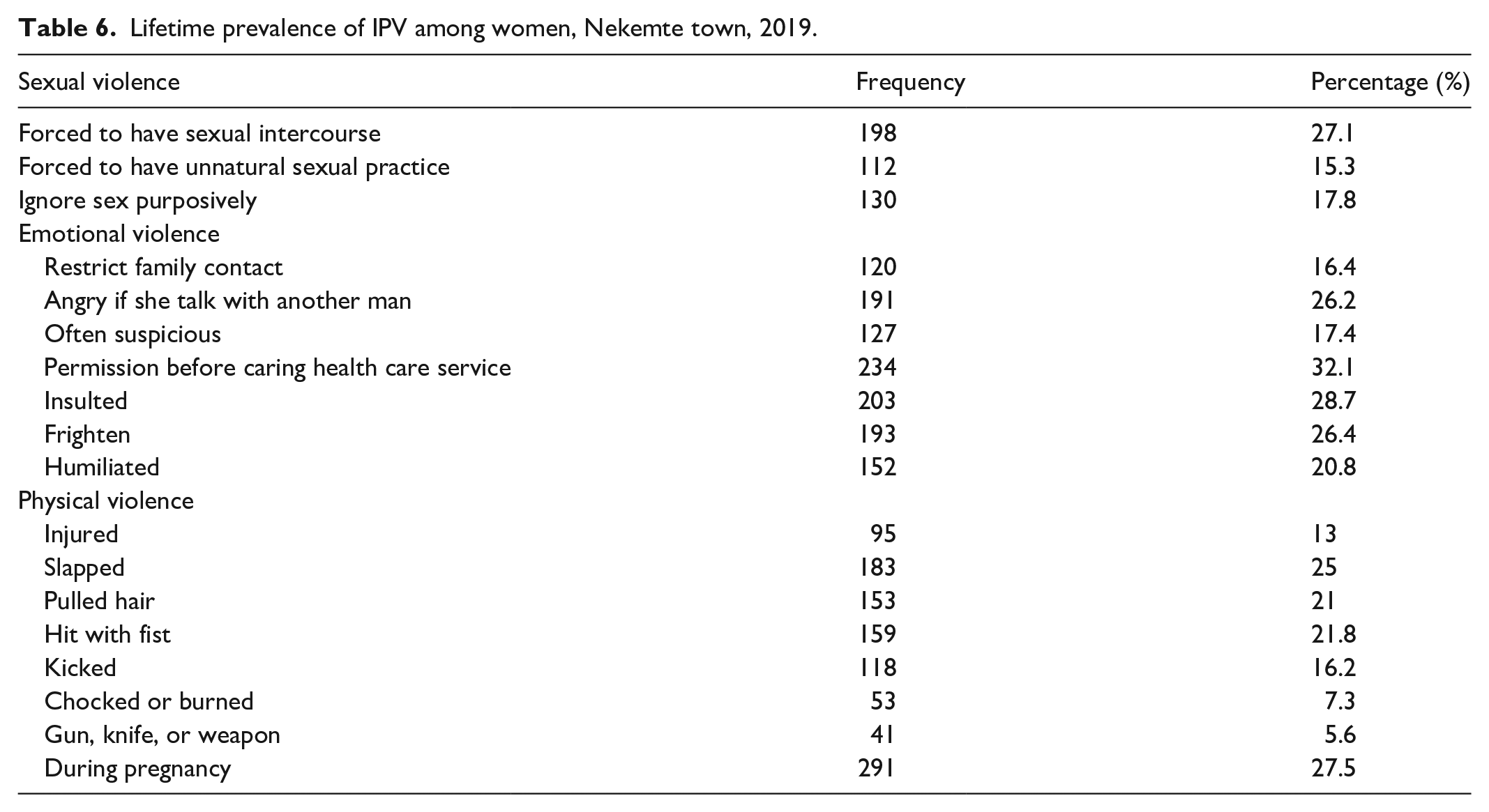
The prevalence of intimate partner sexual violence during their lifetime among women in Nekemte town was 242 (33.2%). About 198 (27.1%) of the respondents reported that their partners had forced them to have sexual intercourse without their interest. In addition, 112 (15.3%) of respondents experienced unnatural sexual intercourse and 130 (17.8%) of the respondents were ignored by their husbands for sexual intercourse. According to findings from qualitative studies, specific acts of sexual violence they faced that they forced to do sexual intercourse without their feelings and even they do not have right to refuse it if their husband wants.
Emotional violence
The prevalence of psychological or emotional IPV during their lifetime among women in Nekemte town was 358 (49%), of which the women needed permission to contact health care services was 234 (32.1%). Qualitative research consistently finds that women frequently consider emotionally abusive acts to be more devastating than physical violence. The specific acts of emotional abuse by a partner as most of them responded in this study include being insulted, humiliated or belittled in front of others, being intimidated, and being threatened with harm (directly or indirectly in the form of a threat) to hurt someone the respondent cared about services.
Physical violence
In this study, at least one-third (34.8%) of women were physically violated by their intimate partner. The women reported the type of physical violence was slapped 25% followed by being hit with a fist 21.8%, pulled hair 21%, kicked 16.2%, injured 13%, choked or burnt was 7.3%, and a pistol, knife, or another weapon was 5.6%. A quantitative study found that the majority of women respond that the specific acts of IPV acts of physical violence include being hit with a belt, pulling hair, and being hit with a fist. Types of physical, sexual, and emotional violence among women in their lifetime are illustrated in Table 6.
Lifetime prevalence of IPV among women, Nekemte town, 2019.
One of the participants aged 34 years who is found in Darge sub-city zone seven responded that, once upon a time when I asked him, about coming home late, he said that it’s not your business to ask me and he hit me with his fist directly into my eyes. This is not the only time he repeatedly hurt me, even in front of my children.
Prevalence of IPV during the last 12 months
The prevalence of IPV in the last 12 months in this study was 35.3%, from which sexual violence was 184 (25.2%), emotional violence 198 (27.1%), and physical violence was 202 (27.7%), the forms of IPV in the last 12 months (Table 7).
Twelve-month prevalence of IPV among women in Nekemte town, 2019.

In addition, this study finds that nearly half of the respondents believe that a good reason to beat a wife is when she disobeys her husband 356 (48.8%) and refuses sex with him 186 (25.5). The major reasons for occurrences of intimate partners as raised by the majority of the respondents from qualitative data analysis are social and cultural factors which undermine women, lack of education of women, lack of decision-making power of women, and also lack power in controlling resources. In addition, some women who are less educated than their partner are suffering more violence. Reasons to beat a wife are displayed in the following chart (Figure 2).
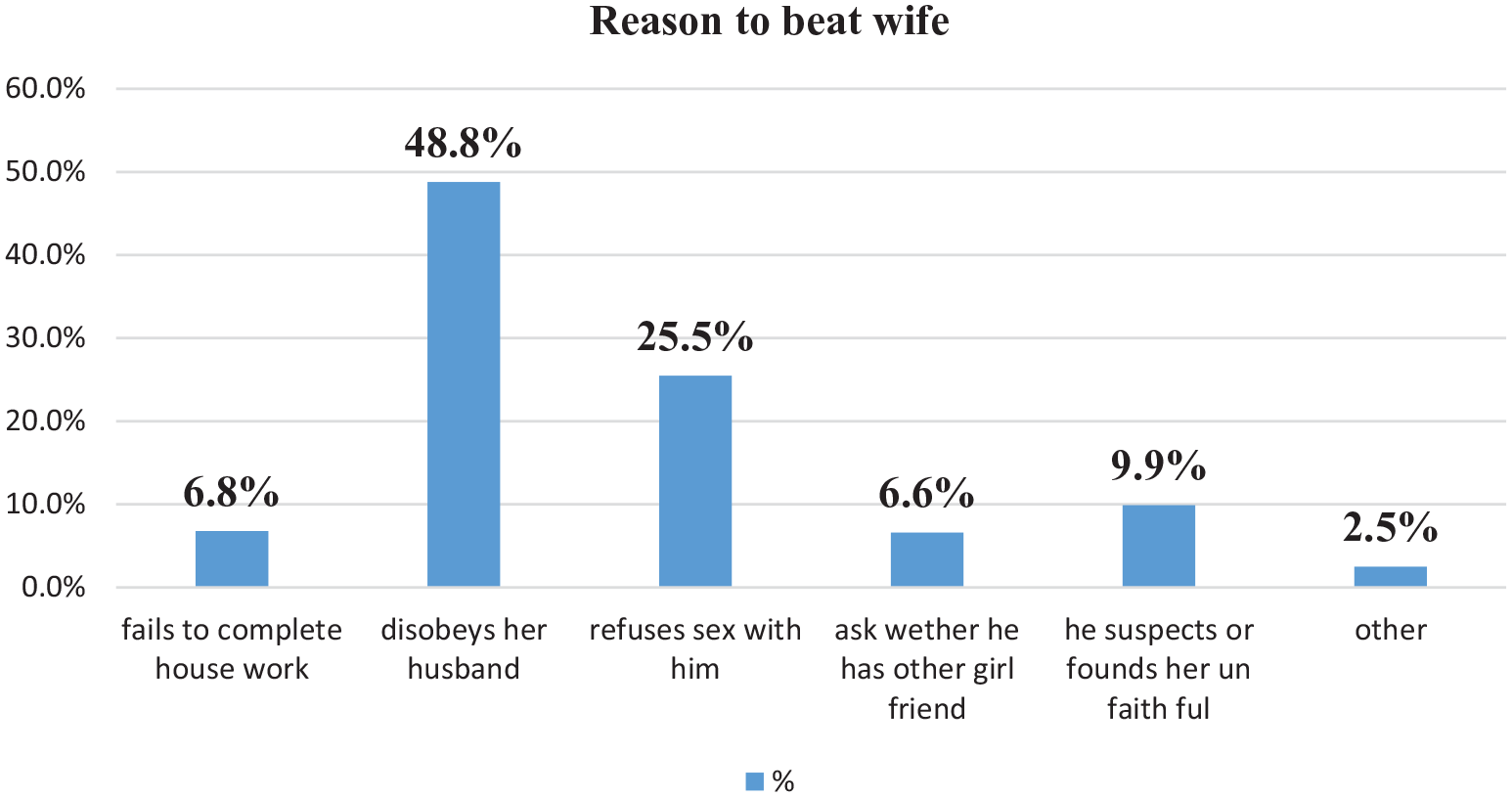
The reason to beat wife among married women, in Nekemte town, Western Ethiopia, 2019.
Health system response to IPV
The study shows that there was no screening done for occurrence of IPV at health facilities among the respondents who visited health facilities for any services, which was 678 (92.9%). Regarding the place where they go when they face any type of violence, the total occurrences of IPV are 408 (55.9%), majority of them resolve the case with family 247 (33.8%), while 59 (8.1%) of them go to a health facility. From those who visit health facilities, about 44 (74.5%) of them get treatment, while 15 (25.4%) get counseling. Regarding qualitative data analysis, most of respondents, especially from the health sector, state that the service given at health facilities was not done adequately as needed or as standard and the rest were documented as follows in a document review of those facilities. About seven documents reviewed at public health facilities during this study in Nekemte town reveal that a screening service for IPV has not yet started, and it is not integrated into any maternal service for women’s coming for any service, for example: antenatal care, delivery, postnatal care, family planning, and outpatient department and all needed units.
There were assigned focal persons at three health facilities and Nekemte Town Health Office. They took training with WHO standard guidelines for integration of women’s affairs, and police to be together at a health facility in an identified room to give one shop service. However, there is no identified room for them, and currently, they are not giving one shop service at health facilities. Only Nekemte specialized hospital is currently building identified rooms to respond to all gender-based violence, but other facilities are on the same standard. Even though the training they have taken able them to give minimum package provided like—screening, clinical care, and psychosocial support, currently, those services were not given in all health facilities rather for women coming to health facility when they raped and report to police then come with complaint with police to health facility which is not IPV. In addition, there is no standard registration and report format for this, it is not prioritized and included in a Woreda-based plan. The assignment focal person at the facility only prepared a plan.
One of the participants aged 30 years who is found in the Nekemte Health Center responded that “There is has a has been assigned focal person and training was given to them, but, screening of intimate partner violence not started yet and it’s not integrated to any maternal service in our Health center.” This was the service given at health facilities regarding IPV during the study period.
Factors associated with IPV
Woman-related factors
Binary logistic regression for factors of IPV among study participants found that age, occupation, educational level, live in marital relation, age at first marriage, and seen parent’s violence during childhood among women-related factors were statistically associated with IPV (see Table 8).
Woman-related factors for Intimate partner violence in Nekemte town, Ethiopia, 2019.
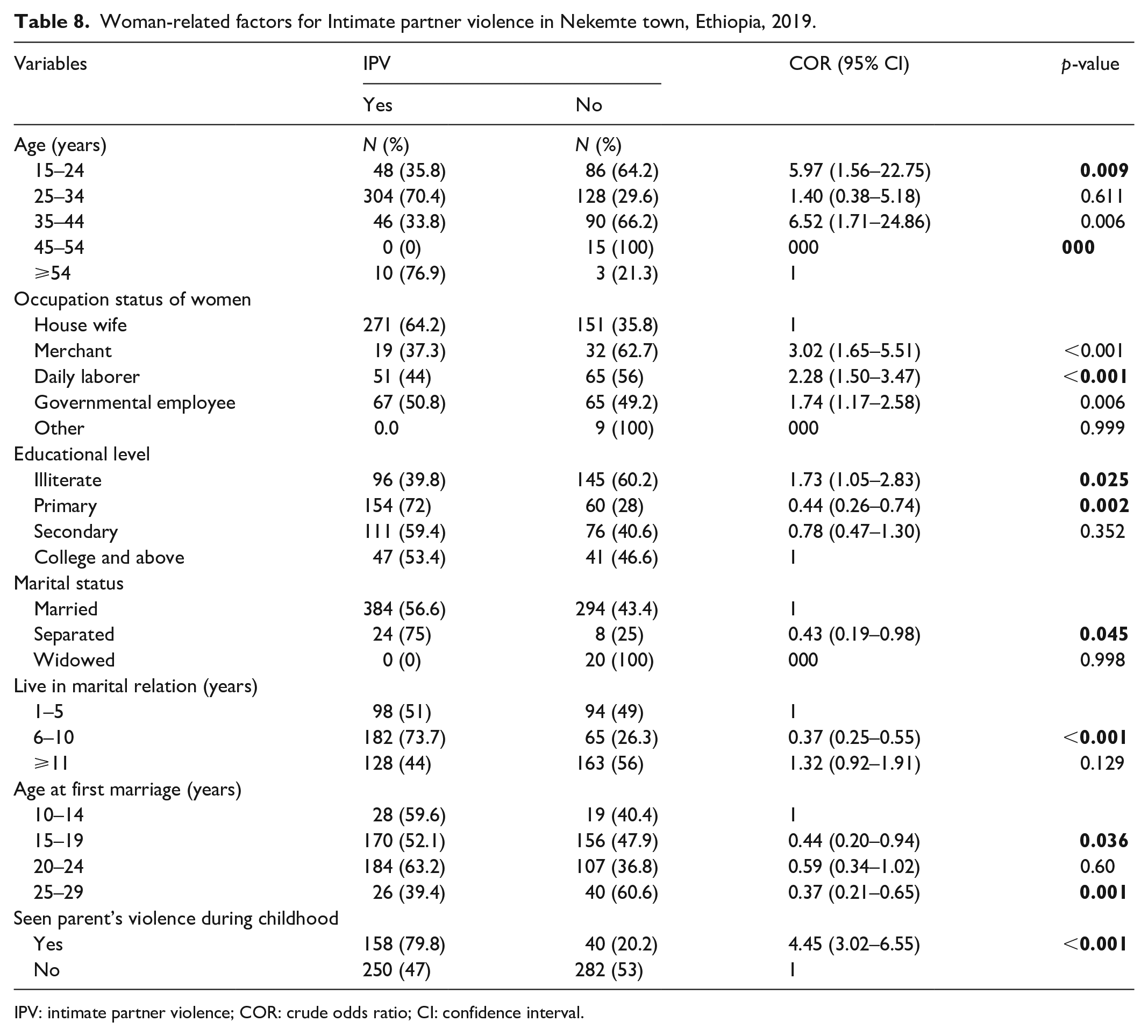
IPV: intimate partner violence; COR: crude odds ratio; CI: confidence interval.
Factors associated with IPV related to partners
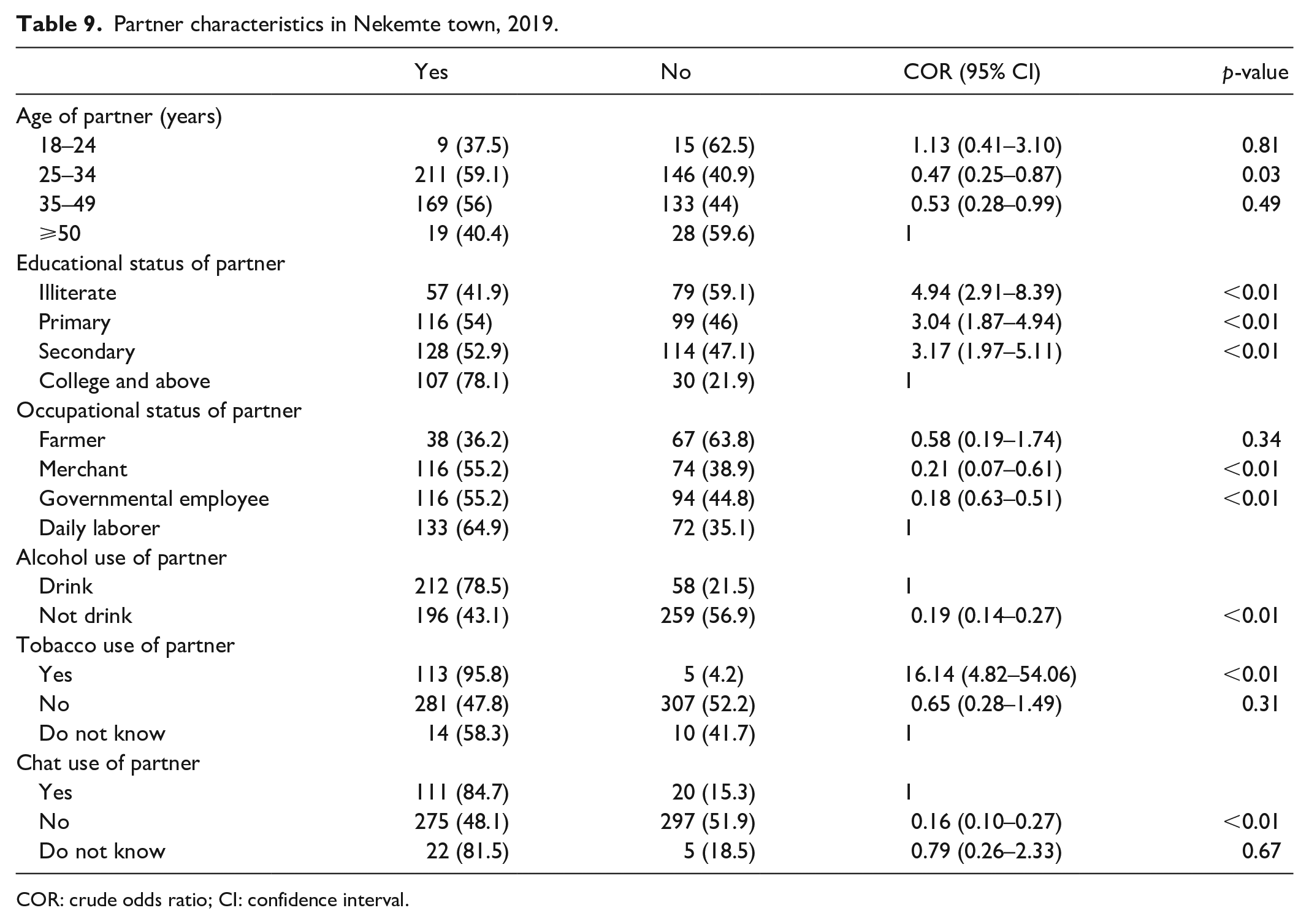
Binary logistic regression for factors of IPV among study participants found that age of partner, educational status of partner, occupational status, partner having another wife, and alcohol, chat, and tobacco use of partner among husband-related factors were statistically associated with IPV (see Table 9).
Partner characteristics in Nekemte town, 2019.
COR: crude odds ratio; CI: confidence interval.
HH-related characteristics of women and their partners
Binary logistic regression for factors of IPV among study participants found that number of children, economic status, discussion about sexuality openly, and decision-making power and marriage arrangement HH-related factors were statistically associated with IPV (see Table 10).
Household-related factors for Intimate partner violence in Nekemte town, Ethiopia, 2019.

COR: crude odds ratio; CI: confidence interval.
Socio-cultural factors to IPV
Binary logistic regression for factors of IPV among study participants found that marriage arrangement, having another wife of their partner, and attitude toward IPV among socio-cultural–related factors were statistically associated with IPV (see Table 11).
Socio-cultural factors for Intimate partner violence in Nekemte town, Ethiopia, 2019.

COR: crude odds ratio; CI: confidence interval.
Multivariate analysis of factors associated with IPV
Nineteen 18 variables in bivariate logistic regression analysis were entered into multivariate logistic regression analysis models to control for possible confounders. There are some factors identified in the occurrence of IPV, such as educational status, occupational status, seen childhood partner violence, having another wife of partner, and alcohol intake of a partner are significantly associated with the occurrence of IPV during the study period.
Multivariate analysis of this study showed that illiterate women were 1.73 times more likely to be violated by their intimate partner than women with college and above educational status (adjusted odds ratio (AOR) = 1.73, 95% CI = (1.05–2.83), p < 0.001). Partners who have no formal education are 5.94 times and those with primary are 4.05 times more likely to violate their wife than partners with educational status of college and above (AOR = 5.94, 95% CI = (1.25–12.23), p < 0.001) and (AOR = 4.05, 95% CI = (2.07–6.49), p < 0.001), respectively.
Regarding the occupation of the study participants, those who are merchants were 4.41 times and those with occupation of daily laborer 3.74 times more likely to be violated by their intimate partner when compared to those who are house wife (AOR = 4.41, 95% CI = (1.49–13.01), p = 0.007) and (AOR = 3.74, 95% CI = (1.33–10.50), p = 0.012). From those study participants, those who have seen parents’ violence during childhood were 2.15 times more likely to be violated by their intimate partner than those who have not seen (AOR = 2.15, 95% CI = (1.00–4.63), p = 0.048).
From those study participants, who live with partners that do not have another wife are 0.97 times less likely to violate their intimate relationship than partners who have another wife (AOR = 0.97, 95% CI (0.03–0.27), p = < 0.001). Regarding alcohol use of partners, partners who do not drink alcohol are 0.32 times less likely to violate their partner than those who drink alcohol (AOR = 0.32, 95% CI = (0.16–0.64), p < 0.001). Multivariate analyses of factors associated with IPV were elaborated in Table 12.
Predictors of IPV.

IPV: intimate partner violence; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
p < 0.05.
Discussion
In this study, the prevalence of IPV was 55.9% during their lifetime and 35.3% during the last 12 months. Prevalence estimates in this study were greater than the study done in Ethiopia, in 2016. 21 Estimates, however, were lower in comparison to a study done in Western Ethiopia, in 2011; 22 this may be due to the exclusion of women from rural areas in this study. Another reason might be that some women may suffer from recall bias, which leads to under-report of IPV.21,22
From this study, physical violence was 34.8% during their lifetime and 27.7% in the last 12 months. That is greater than study done in Uganda, which was 30% and less than study done in Kenya, which was 38%. This difference may be due to social differences in Ethiopia and respective countries.6,7
Another feature of IPV investigated in this study is sexual violence, which was 33.2% during their lifetime and 25.2% in the last 12 months. This is greater than a study done in the EDHS 2016 and less than a study done in Western Ethiopia 2011. This may be justified as women are less inclined to disclose sexual violence because it is a shameful and very sensitive topic.21,22
The emotional/psychological IPV was 49% during a lifetime and 27.1% during the last 12 months in this study. This study is much greater than the study done on EDHS 2016, and it is greater than a study done among Kenyan women that revealed that the rates of exposure to emotional violence were 24%. 7 In addition, this study was greater than study done in Uganda, in which the prevalence of IPV by a male against his female partner was found to be 40% and less than the study done in Western Ethiopia 2011 indicated that the lifetime prevalence of IPV was 70.2%. 21 This may be due to that, as rural areas were not included in this study and some women may suffer from recall bias, unable to remember some of the IPV experiences that they may have accepted as a part of marital life.
In addition, this study finds that just about half of the respondents believe that a good reason to beat a wife is when she disobeys her husband and refuses sex with him. This study is in consistence with study done in Butajira. 4
Correspondingly, from a study conducted in Butajira, the study shows attention was not given to health facilities. There was not any screening done for occasions of IPV at facilities among the respondents who were going to the health facility for any service, which indicates service is not yet started and there is no service integration at those health facilities at: antenatal care, delivery, postnatal care, family planning, and outpatient department and all needed units. One of the participants aged 30 years who is found in the Nekemte Health Center responded that “there is an assigned focal person and training was given to them but screening of IPV has not started yet and it’s not integrated into any maternal service in our health center.” 4
According to findings from this study, there was assigned a focal person at Nekemte Town Health Office including those facilities and they took training with integration of women’s affairs and police to be together at facilities in identified room, but there is no identified room for them, and currently they are not giving one shop service at health facilities. Even though the training they have taken able them to give minimum package provided such as screening, clinical care, and psychosocial support, currently, those services were not given rather for women’s coming to health facility when they raped and report to police and then come with complaint with police to health facility which is not IPV. In addition, there is no standard registration and report format for this; it is not considered in a Woreda-based plan. Only assigned focal person at facility level prepared plan.
The result of this study depicted that educational status, occupational status, childhood partners’ violence partner having another wife, and drinking alcohol of partner are factors found to be associated with occurrences of IPV among married women in Nekemte town.
The level of education for both women and men was identified as statistically significant. IPV decreased as the educational status of women increased and decreased when the educational status of partners increased. This is consistent with study done in East Wollega 2011; 22 the protective effect of education appears to start only when women’s education goes beyond secondary school. It may be that women with higher education have a greater range of choice in partners and more ability to negotiate greater autonomy and control of resources within the family. This helps to change norms and improves socio-economic conditions that capacitate them to protect themselves. 22 One of the respondents whose age was 30 years and lives in Makanisa-Kese sub-city said that “I don’t have any peace in my house since our marriage, but when I improve my educational status it’s somewhat improved.”
Unlike the study done on Abay Chomen, the risks of experiencing intimate partners with women were about five- and four-fold in merchants and daily laborers, respectively. 23 This may be because there is a burden of workload on women and less satisfaction with her partner in her work (taking care of children and preparing food for family), which leads to being violated by her partner.
In this study, respondents who have witnessed partner violence during childhood were more than twofold violated by their intimate partner. This is consistent with a study done in Southwest Ethiopia and Abay Chomen.23,24 Even though in the majority of the study done in Ethiopia, such as study done in Hosanna town, Hadiya Zone, and Abay Chomen, drinking alcohol by partners is an associated factor of IPV, while in this study, partners who have not drunk alcohol are protective factors.23,25
Limitations of the study
The disclosure of IPV against women can be a sensitive private issue kept as a family secret in most instances. It might be affected by social desirability bias. In addition, some women may suffer from recall bias, unable to remember some of the IPV experiences that they may have accepted as a part of marital life. Therefore, social desirability and recall biases may result in under-reporting of IPV by the study participants.
Conclusion
In this study, the prevalence of IPV was more than 50% of the women who experienced at least one of IPV by their intimate partners during their lifetime. In addition, the study shows that there was no screening done for occurrences of IPV at health facilities. Factors like educational status, occupational status, seen childhood parents’ violence, partner having another wife, and drinking alcohol of partner were factors found to be associated with IPV.
The implication of the study findings regarding the practice of IPV is common in the study site. Even though family law was revised in favor of women and established women’s groups. However, there is still a lot more to be done to reduce the incidence of IPV, as it remains a substantially under-reported crime due to the culture that IPV is considered as part of marital life. From the study, we conclude that by increasing the educational status of men and women, engaging the health system to integrate violence into health service and strengthening legal issues, we can reduce occurrences of IPV.
Educating women, men, and acting on socio-cultural and behavioral factors integrating into the health system and including the husbands/partners in the IPV prevention strategies are important. Reducing the incidence of intimate partners needs to be an important multisectoral goal which all stakeholders and responsible bodies should act on.
It is better if the Health Department integrates IPV service into health system response starting from planning and budgeting, also integrating at facility level in all departments and providing a minimum package including screening, and it is better to include IPV as one component of the health extension package. Researchers need to conduct research on factors of IPV and on health system response and factors associated with it in detail.
Footnotes
Acknowledgements
The authors thank Nekemte Town Administration Office, selected sub-cities and Nekemte Town Health Office, health centers, all supervisors, data collectors, and study participants for their cooperation and support during study period.
Author contributions
E.W. conceived the study, wrote the proposal, facilitated data collection, analysis, data interpretation, drafted the final report, wrote up, and prepared the manuscript. E.A.G., B.M., L.A., and M.M. participated in developing the tools and data collection process, data analysis, and involved in report write up. All authors read and approved the final manuscript.
Data availability and materials
The data set analyzed during this study available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
An ethical clearance to conduct this study was obtained from the Department of Public Health, Institute of Health Sciences, Wollega University Institutional Research Review Committee, and a letter of approval with reference no. WU/RD/279/11 was granted.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the subjects/legally authorized representative/parents prior to study initiation.