
Abstract
Objective:
Millennium Development Goal 5 calls for increasing proportions of deliveries assisted by skilled health personnel to reduce maternal mortality. This study aims to identifying the implication of exposure to intimate partner violence on these proportions.
Methodology:
This study used domestic violence modules data of Demographic and Health Surveys of six countries from 2005 to 2007. Proportions of assisted deliveries were examined by sociodemographic characteristics and exposure to intimate partner violence in the studied countries. Influence on the proportion was examined against exposure to intimate partner violence through odds ratio and 95% of logistic regression analysis after controlling for women age, residence (urban/rural), household wealth level, economic level of country, educational level and working status of women and their husbands/partners.
Results:
Data sets of 18,507 participants over 20 years of age showed that almost three-quarters (73%) of women had deliveries assisted by skilled health personnel. One-third of the women were ever exposed to intimate partner violence (37%) and 9% of them to the severe level. Exposure to intimate partner violence statistically significantly lowered this proportion to 69% (odds ratio: 0.73; 95% confidence interval: 0.67–0.78) meanwhile severe violence lowered it to 65% (odds ratio 0.64; 95% confidence interval: 0.58–0.72). When running multiple regression analysis, exposure to intimate partner violence retained its statistically significant decreasing influence on proportions and was not biased by the other stronger socioeconomic characteristics.
Conclusion and recommendations:
Intimate partner violence has an independent influence on reducing assisted deliveries by skilled health personnel. Programs working for increasing proportions of assisted deliveries by skilled health personnel are recommended to integrate protection women from violence.
Introduction
Intimate partner violence (IPV) against women is a worldwide problem. The reported lifetime prevalence varied from 15% to 71%. 1 Extensive research indicates that IPV poses a significant risk to the physical health of women. IPV is associated with increased mortality, injury and disability; worse general health; chronic pain; substance abuse; reproductive disorders and poorer pregnancy outcomes. IPV is also associated with an overuse of health services and unmet need for services, as well as strained relationships with providers.2,3 Despite wide variations in its prevalence, many risk factors were noted. 4 In addition to being a breach of human rights, it is associated with serious public health consequences,5–11 and it was found to be a barrier to women access to health care specifically among vulnerable groups of women.12,13
High rates of IPV and disproportionately high maternal mortality ratios in developing countries were recognized as global public health problems. 14 The risk of maternal mortality is 3 times as high for abused mothers. 15 It was found that women’s experience of IPV may influence receipt of skilled attendance during parturition as lifetime experience of emotional violence was found to decrease the odds of skilled attendance at most recent delivery by 40%, while lifetime experience of physical violence reduced the odds by 29%. 16 Women reporting IPV in the year prior to pregnancy were at increased risk of many health problems such as high blood pressure or edema, vaginal bleeding and others compared with those not reporting IPV. 17 IPV is related to unwanted pregnancy and higher rates of pregnancy loss or termination, particularly miscarriage, induced abortion18–20 and complicated delivery. 21 It was found that women who were victims of IPV were more likely to give birth prematurely and deliver low-birth-weight and very low-birth-weight infants.22–24
Millennium Development Goal (MDG) 5
25
aims to improve maternal health through reducing maternal mortality by three-quarters by 2015 and achieving universal access to reproductive health services. The majority of maternal mortalities are avoidable through a range of interventions administered by a skilled health-care provider with adequate equipment and supplies. World Health Organization (WHO) defines a skilled birth attendant as
an accredited health professional—such as a midwife, doctor or nurse—who has been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth and the immediate postnatal period, and in the identification, management and referral of complications in women and newborns.26–28
Poor social and economical situation was found29,30 to have a detrimental impact on the use of maternal health-care services, which might be associated with poor education and low financial capacities of the women. The association between exposure to IPV and use of reproductive health-care services suggests that partner violence plays a significant role in lower utilization of reproductive health services among women. 31
In spite of extensive study of impact of exposure to IPV on women’s lives and the international efforts to reduce the maternal mortality rates through skilled birth attendants, there is a gap of literature relating the impact of IPV on utilization of assisted deliveries by skilled health personnel. This study aims to identify the influence of exposure to IPV on these proportions.
Methodology
Study design
This study used secondary data analysis of Domestic Violence Modules of Demographic and Health Surveys (DHS), which are nationally representative surveys that employ standardized questionnaires to collect extensive data from women of reproductive age (15–49 years) in developing countries. The DHS obtain information on women’s sociodemographic characteristics, their reproductive behaviors, birth history and maternal health service utilization. 32 Six countries were selected, each representing one of the six WHO regions that used the domestic violence module of DHS in the period 2005–2007. They were Bangladesh, 2007; Cambodia, 2005; Colombia, 2005; Egypt, 2005; Ukraine, 2007; and Zambia, 2007. Half of the studied countries (Bangladesh, Cambodia and Zambia) were among the low-income economics according to the World Bank classification 33 of having gross national income (GNI) of less than US$995. Egypt and Ukraine were among the lower-middle-income economies (US$996–US$3945), while Colombia was higher from the upper-middle-income economies (US$3946–US$12,195).
Maternal mortality ratio from the selected countries for the same period showed the same pattern as the poorest countries (Bangladesh, Cambodia and Zambia) have higher maternal mortality rate with highest in Zambia (470/100,000). Countries with higher income had lower maternal mortality rate, specifically Ukraine that had 26 per 100,000 only, meanwhile both Egypt and Colombia had 85 and 82, respectively. 34
Variables
IPV was considered for the answer of yes for the DHS variable of “experienced any of less severe violence.” This variable is computed of four variables of spouse ever pushed her or threw something; slapped or twisted arm; punched with fist and ever kicked or dragged her.
Severe IPV was defined as the answer of yes to the DHS variable of “experienced any severe violence.” This variable is computed from three variables of spouse ever tried to strangle or burn; threatened with knife or weapon and ever attacked with knife or weapon.
Assisted delivery by skilled health personnel variable was computed from variables of deliveries assisted by a doctor, nurse or trained midwife.
Household wealth level was measured through the wealth index variable of the DHS that has five levels from poorest to richest level.
Economic level of the country was identified according to the World Bank classification.
Educational level was measured as defined according to MDG 2 35 such as completed at least primary education.
Inclusion and exclusion criteria
Since adolescence has different sets of reproductive health problems, participants aged 15–19 years were excluded from the data file. Only data for women over 20 years of age were included in the analysis.
Data analysis
Data were analyzed using SPSS version 21. Proportions of assisted deliveries by skilled health personnel were examined by different sociodemographic characteristics, exposure to both less severe and severe IPV in the studied countries using tests of significance, odds ratio (OR) and 95% confidence interval (CI). Logistic regression analysis was conducted to identify the influence of exposure to IPV on the use of assisted skilled personnel in deliveries as the dependent variable with control of women age, residence (urban/rural), household wealth level, economic level of country, educational level and working status of women and their husbands/partners.
Ethical considerations
Permission to download and use the data was obtained from Measure DHS Macro, Inc. The data were previously de-identified to keep the confidentiality of the surveys participants.
Results
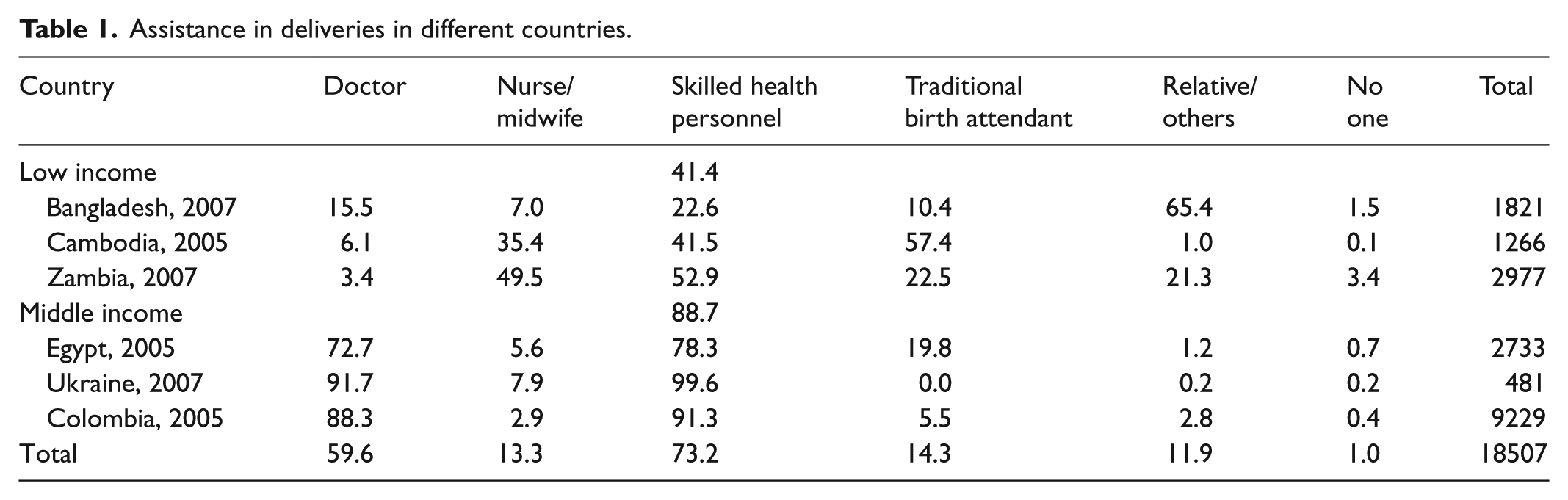
Data sets had 18,507 participants over 20 years of age from the six different countries. As Table 1 shows, almost three-quarters (73%) of the studied women had deliveries assisted by skilled health personnel as doctors (60%) and nurses/midwives (13%). This varied from country to other, as it was almost universal in Ukraine versus 23% only in Bangladesh. It also varied with economic level as countries with low income had statistically significant lowest proportions of 41%. Meanwhile, women living in middle-income countries had 11 times more (95% CI: 10.33–12.02) assisted deliveries. Traditional birth attendants (TBA) attended deliveries of more than half of women in Cambodia, whereas relatives attended the deliveries of most of women in Bangladesh.
Assistance in deliveries in different countries.
One-third of the women were ever exposed to IPV (37%) and 9% only were ever exposed to severe violence (Table 2). Half (55%) of the women who were exposed to IPV were formerly married ones with highest level among divorced (63%) and they were twice the currently married ones. Younger, uneducated, poorer, living in low-income country with uneducated and not working husband were more to be exposed to IPV. Exposure to IPV was higher among women who were working as skilled manual workers (42%) and in services and sales (40%); meanwhile, those working in clerical or professional occupations were the least (26% and 19%, respectively). Bangladesh and Zambia showed the highest prevalence (49% and 47%, respectively), while Ukraine showed the least level of IPV (9%).
Sociodemographic characteristics of women exposed to IPV.

IPV: intimate partner violence; OR: odds ratio; CI: confidence interval.
p < 0.0001; number of partners = 16,487.
Severe violence was 3 times among formerly married women as it was among 21% and more specifically among divorced (26%). It was almost twice among those married to unemployed husbands and living in low-income countries than middle-income ones. Poorer, uneducated women, married to uneducated husbands were more to be exposed to severe IPV. Women working in sales and services were more to be exposed to it (11%), whereas those working in clerical jobs and professional occupations were the least (4% and 4.5%, respectively). Bangladesh and Zambia had the highest prevalence (16% and 14%, respectively), whereas it was the least in Egypt (1.5%).
Proportions of assisted deliveries by skilled health personnel were the highest among women residing in urban areas, higher income countries and wealthier households and those who were currently married. Younger, educated women, working, married to educated and working husbands were more to have assisted delivery by health personnel. Exposure to IPV statistically significantly lowered this proportion to 69% (OR: 0.73; 95% CI: 0.67–0.78), whereas exposure to severe violence lowered the proportions to 65% (OR: 0.64; 95% CI: 0.58–0.72; Table 3).
Influence of sociodemographic characteristics and IPV on proportion of assisted deliveries.
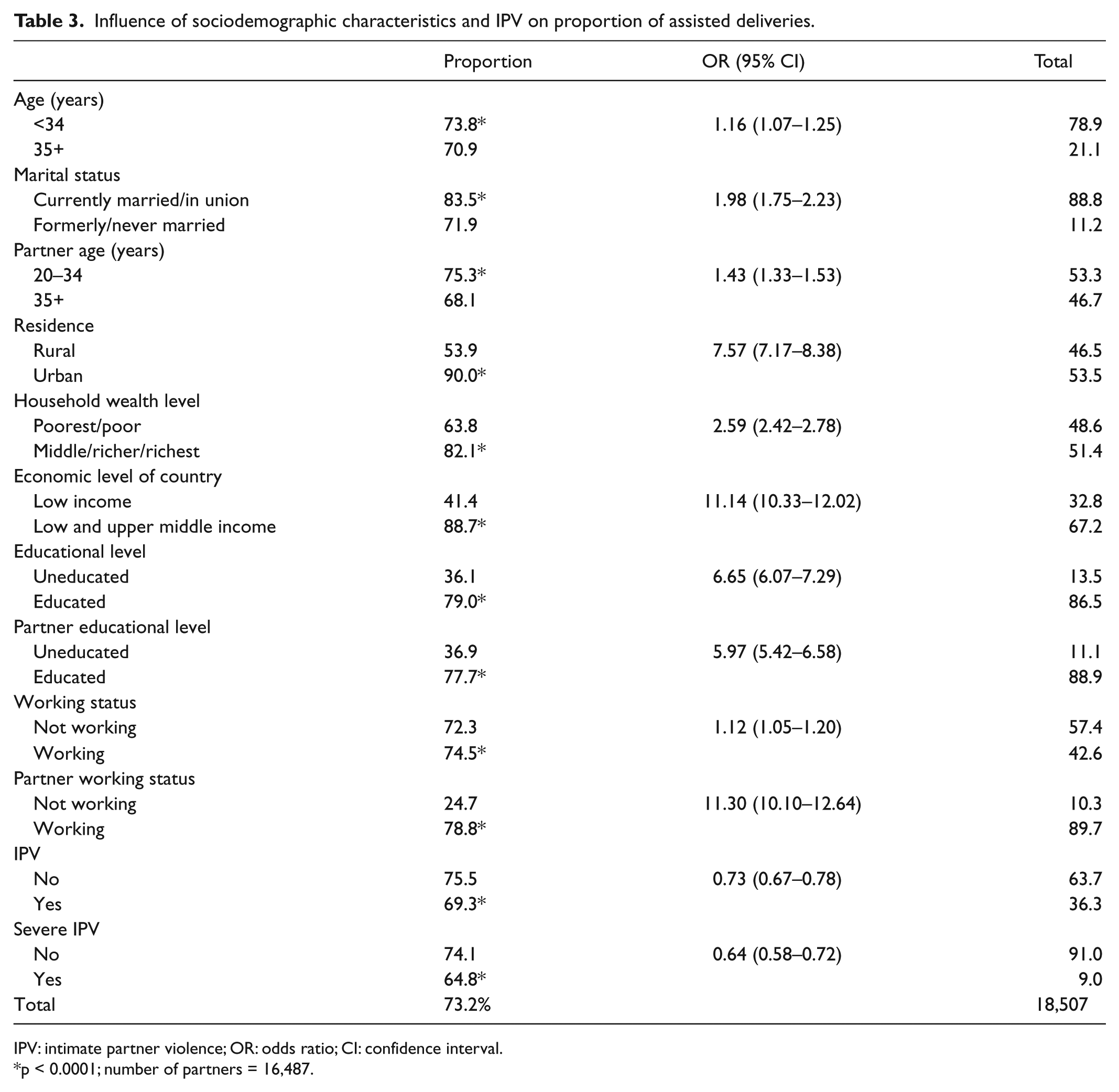
IPV: intimate partner violence; OR: odds ratio; CI: confidence interval.
p < 0.0001; number of partners = 16,487.
Declining of assisted deliveries due to exposure to violence was among all countries (Figures 1 and 2) and was highest in Bangladesh as it was lowered to the half as 15% versus 30% among unexposed to IPV (OR: 0.41; 95% CI: 0.32–0.51), followed by Egypt as it was 74% versus 80% among unexposed to IPV (OR: 0.71; 95% CI: 0.58–0.86). Exposure to severe IPV lowered it in Bangladesh to 14% versus 24% of unexposed to severe IPV (OR: 0.49; 95% CI: 0.35–0.71), followed by Colombia of 88% versus 92% among unexposed (OR: 0.68; 95% CI: 0.55–0.85).

Influence of exposure to IPV on proportion of assisted deliveries among the six different countries.

Influence of exposure severe IPV on proportion of assisted deliveries among the six different countries.
When running multiple regression analysis (Table 4), exposure to IPV retained its statistically significant decreasing influence on deliveries assisted by skilled health workers and was not biased by the other stronger socioeconomic characteristics. The strongest determinants of having assisted deliveries were living in middle-income country (8 times the lower income ones); followed by urban residence and working husband/partner (4 times each) then being an educated woman (3 times).
Influence of IPV and socioeconomic factors on proportion of deliveries assisted by skilled health personnel (multiple logistic regression analysis).
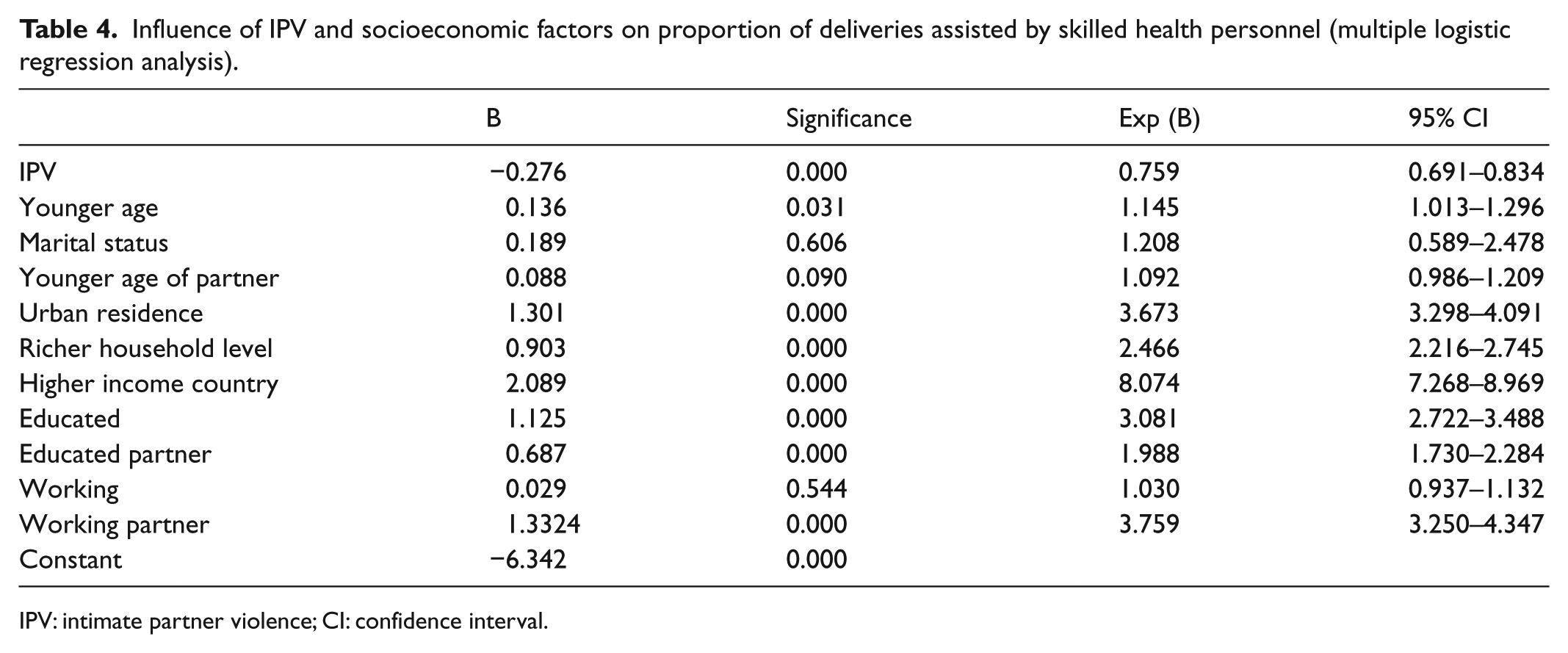
IPV: intimate partner violence; CI: confidence interval.
Discussion
Maternal mortality is still unacceptably high. The high number of maternal deaths in some areas of the world reflects inequities in access to health services and highlights the gap between rich and poor. There are also large disparities within countries, between people with high and low income and between people living in rural and urban areas. 36 The results of this study confirmed these inequalities of access to assisted deliveries by skilled birth attendants, with exception of Ukraine that showed universal access despite that it was not the highest in income; however, the highest in educational level. Low-income countries showed the highest levels of exposure to domestic violence and suffered the highest burden of it on the proportions of assisted deliveries. The highest impact of IPV on lowering proportion of assisted deliveries confirmed previous study results of the impact of IPV on lower utilization of reproductive health in Bangladesh. 37 Results confirmed the impact of income and education on assisted deliveries by skilled birth attendants in developing countries too.38,39 In spite of the limitation of using the cross-sectional design of DHS data collection, the results of this study showed that the burden of exposure to IPV was not biased by the stronger influence of socioeconomic factors.
United Nations led international efforts in the form of MDG 5 in decreasing maternal mortality through strengthening training of skilled birth attendants and upgrading infrastructures. Meanwhile, MDG 3 is aiming to promoting gender equality through women empowerment. However, violence against women continues to undermine efforts to reach all goals. 40 Integration of prevention and protection of women from IPV in health profession educational programs is required to help health personnel to identify IPV and screen for its manifestation; 41 however, health professional curricula still need comprehensive approaches to teaching IPV.42–44
Some governments and professional organizations recommend screening all women for IPV rather than asking only women with symptoms. Studies comparing screening versus case finding (with or without advocacy or therapeutic interventions) for women’s long-term well-being would better inform future policies in health-care settings.45–47
This study calls for integrating protection of women against exposure to domestic violence in programs working on reducing maternal mortality, especially for women living in developing countries. Integration into health professional educational curricula and regular screening of IPV would have a positive social change on the proportions of use of skilled health personnel in deliveries.
Footnotes
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.