
Abstract
Background:
This mixed-methods study examined the general public’s knowledge and attitudes about vascularized composite allografts. The availability of these anatomical gifts to treat individuals with severe disfiguring injuries relies largely on decisions made by family members. If vascularized composite allograft transplantation is to become more readily available, the knowledge and beliefs of the general public must be explored to ensure vascularized composite allograft donation approaches adequately support the donation decision-making process.
Methods:
We conducted six focus groups with 53 members of the general public, which were audio-recorded for accuracy and transcribed. Before each session, participants completed a brief survey assessing donation-related knowledge, attitudes, and beliefs. Analysis of qualitative data entailed the constant comparison method in the development and application of a schema for thematic coding. Descriptive statistics and Spearman’s rank coefficient were used in the analysis of the quantitative data.
Results:
Respondents were most knowledgeable about solid organ donation and least knowledgeable about vascularized composite allograft donation. Six major themes emerged: (1) strong initial reactions toward vascularized composite allografts, (2) limited knowledge of and reservations about vascularized composite allografts, (3) risk versus reward in receiving a vascularized composite allograft, (4) information needed to authorize vascularized composite allograft donation, (5) attitudes toward donation, and (6) mistrust of the organ donation system.
Conclusion:
The general public has low levels of knowledge and high levels of hesitation about vascularized composite allograft donation and transplantation. Education campaigns to familiarize the general public with vascularized composite allografts and specialized training for donation professionals to support informed family decision-making about vascularized composite allograft donation may address these issues.
Introduction
Vascularized composite allografts (VCAs) are defined as human tissue recovered for transplantation and as anatomical units containing multiple tissue types, requiring blood flow from surgical connections of blood vessels. 1 VCAs include the face, hands, arms, uterus, and penis, among others, and may offer an alternative treatment option for those who do not respond well to currently available reconstructive procedures or prosthetics.2–6 Twenty-nine transplant centers currently maintain vascularized composite allotransplantation programs in the United States. 7 To date, 112 VCA procedures have been completed nationwide, and 22 candidates were awaiting VCA transplantation.8,9
Although currently treated as solid organs by United Network for Organ Sharing (UNOS), 10 VCAs are not included with first-person donor pre-designations via driver’s license notations, donor cards, or online registries. 11 As with other anatomical gifts, donation professionals from regional Organ Procurement Organizations (OPOs) obtain authorization of VCAs from the next-of-kin (i.e. family decision makers (FDMs)) of potential donors. While there is some indication that VCA donation is usually raised with potential donor families after they have authorized solid organ and tissue donation, VCA donation requests are neither common nor uniform.11,12 Understanding how the typical layperson relates to and weighs the VCA donation opportunity against the donation of other anatomical gifts is critical to advancing the field.
In addition to its novelty and the relative infrequency of requests for VCA donation, only a modest body of literature exists describing the public’s knowledge, acceptance of, and willingness to donate VCAs. A survey of urban emergency department patients, for example, found lower willingness to donate a VCA (54.6% hand and 44.0% face) than a solid organ, such as a kidney (77.5%). 13 Respondents supported face donation if recipients’ injuries were sustained through military service or no-fault accidents. 13 A survey of the general public in 2016 (N = 1485) found that two-thirds of respondents were willing to donate their own face, legs, and hands/forearms, with a majority also expressing willingness to donate the penis and uterus. 14 Similar levels of support for VCA donation were found among veterans 15 and the general public when asked about a VCA donation from a deceased family member whose donation wishes were known. 14 A recent Gallup poll found strong support for solid organ donation (90.4%) but drastically lower support for VCA donation; 64% of respondents were willing to donate their own hands and 46.9% were willing to donate their own face after death. 16 Respondents were slightly less willing to donate a loved one’s hand (58.6%) or face (43.6%). 16 Reasons for resistance to VCA donation included psychological discomfort with the idea of VCAs, desire to remain whole after death, and the possibility of identifying a VCA on another person.13,14
A more nuanced understanding of the general public’s motivations and rationale behind reactions to VCA donation are needed if VCA transplantation is to become a more readily available treatment for individuals with severe disfiguring injuries. The informational needs of the general public must also be explored to ensure fully informed VCA donation decisions. This study was designed to investigate VCA-related beliefs, attitudes, and behaviors within the general population. The goal was to identify important themes to inform both public education about VCAs and OPO professionals’ discussions of VCA donation.
Materials and methods
Sample and recruitment
An explanatory sequential mixed-methods design 17 was employed. Specifically, brief surveys were administered before subjects participated in in-person focus groups that assessed and explored attitudes and knowledge regarding VCA donation. Because markedly lower levels of organ donation knowledge, less favorable attitudes, as well as lower rates of FDM authorization have been documented among ethnic minorities and groups with lower educational attainment,18,19 sampling was purposive. Specifically, we sought to capture this variation by concentrating recruitment on five demographic groups: (1) Whites with high educational attainment, (2) Whites with lower educational attainment, (3) Black Americans, (4) Latinx Americans, and (5) Asian Americans. The first phase of recruitment was accomplished via paid Facebook advertisements marketed to platform users above the age of 18 and living in the greater Philadelphia region from 1 March 2019 to 26 March 2019. The paid advertisements linked to an online Qualtrics form, which collected demographic and contact information of those interested in participating. We also posted informational flyers, staffed tables at community events, and leveraged long-standing relationships with community stakeholders to promote the study.
Potential participants were contacted by telephone, briefly screened, and scheduled for a focus group session. Participants were deemed eligible after meeting the following inclusion criteria: 18+ years of age, English-speaking, and with no obvious cognitive or decisional impairment. Participants received a $50 honorarium for completing the survey and focus group discussion. The study was deemed exempt by the Temple University Institutional Review Board (Protocol #25254). We used the Consolidated Criteria for Reporting Qualitative Research checklist for guidance in reporting qualitative research. 20
Data collection
Before each focus group began, participants read and signed an informed consent document and completed a brief self-administered survey, based on validated instruments used in past studies.21–24 The survey gathered baseline knowledge and attitudes of organ donation and sociodemographic information to characterize the sample. Sixteen 5-point Likert-type scale questions assessed attitudes toward organ donation; higher scores indicated higher agreement with each statement. Two questions gauged willingness to donate solid organs and a single dichotomous item assessed registered organ donor status (registered/not registered).
The focus groups were conducted on Temple University’s center city campus in Philadelphia, PA, easily accessible via private or public transportation. Focus groups were moderated by a member of the study team with extensive training and experience with qualitative methods (GPA) and facilitated by another trained team member (E.E.D.). Focus groups opened with a discussion about organ and tissue donation to provide background and context for VCA donation. A moderator’s guide focused on five domains: (1) knowledge of organ transplantation, (2) knowledge of tissue transplantation, (3) attitudes about organ donation, (4) attitudes about tissue donation, and (5) knowledge and attitudes about VCA donation. Focus groups also explored respondents’ receptivity to receiving a VCA and the information needed to make an informed VCA donation decision. The guide was informed by interviews with donation professionals. 12 Focus groups lasted from 78 to 110 min, were audio-recorded for accuracy, and transcribed verbatim.
Analytic plan
Descriptive statistics were used to characterize the sample and VCA attitudes and knowledge. Spearman’s rank correlation coefficients assessed the relationship between scale items. SAS 9.4 was used for statistical computations, with values considered significant at α = 0.05.
Focus group transcripts were uploaded to MAXQDA (2018), a qualitative analysis software package, for thematic content analysis. 25 An initial coding schema was developed deductively from moderator’s guide questions; additional codes were identified inductively through transcript review for emergent themes. A final codebook, containing coding rules, definitions, and examples, guided independent coding by two trained study staff. Inter-coder reliability was achieved at 84% agreement. Disagreements were resolved by discussion, and final coded transcripts used for analysis were reconciled cases reflecting coder consensus. 26
Results
A total of 208 individuals expressed interest in participating. Screening for eligibility led to a total sample of 53 individuals (25.5%) who met in six focus groups with 7 to 12 participants in each group. Participants ranged in age from 18 to 71 years, with a mean age of 41 years. Participants were primarily female and over half had earned a bachelor’s degree or higher. Twenty-one participants identified as White, 16 Black, 6 Asian, and 12 as Hispanic (Table 1).
Participant sociodemographics (N = 53).
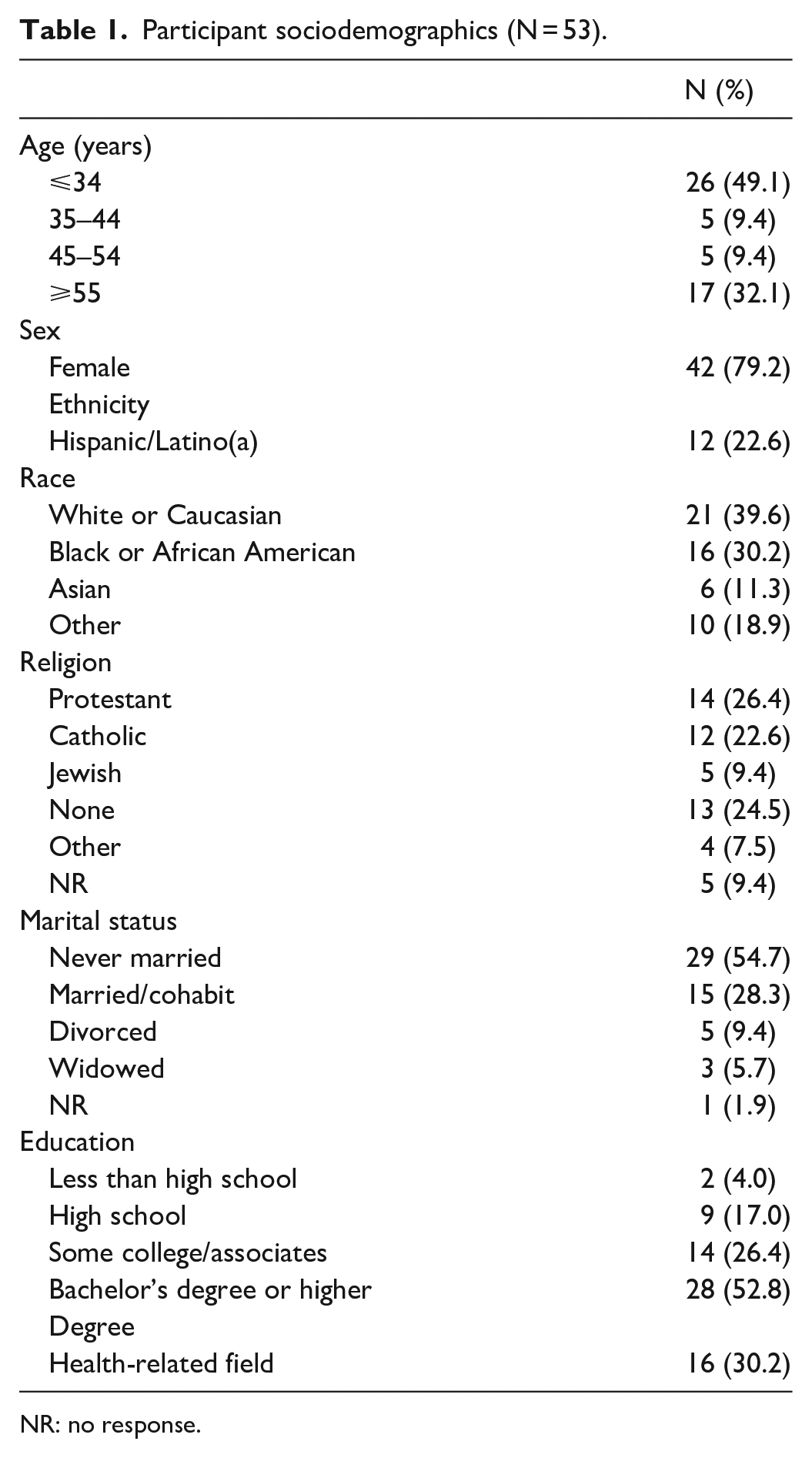
NR: no response.
A comparison of pre-focus group surveys and focus group findings revealed several themes: (1) strong initial reactions toward VCAs, (2) limited knowledge of and reservations about VCAs, (3) risk versus reward in receiving a VCA, (4) information needed to authorize VCA donation, (5) attitudes toward donation, (6) mistrust of the organ donation system. Each theme is described in detail in the following sections.
Strong initial reactions to VCA
Initial reactions to the idea of VCA transplantation as a viable treatment option varied widely. Most participants expressed awe and curiosity about advancements in medical technology. A 21-year-old Hispanic woman said, “I’m just so amazed that medicine has come this far. That that is something that’s possible. I really, I’m happy about that. That’s awesome” (P2, FG4). Similarly, a 61-year-old Black man shared, “it’s amazing to me that the technology has advanced that far that you can do stuff like that” (P1, FG2). However, not everyone shared the same enthusiasm. A 22-year-old Asian woman stated, “I’m not exactly comfortable with it . . . that is literally your face on another person’s face” (P6, FG1). A 37-year-old Black woman had a strong visceral reaction to the idea of VCA donation proclaiming, “Hell to the no!” (P1, FG1). These initial responses gave way to more nuanced rationale for both supporting and opposing VCA donation.
Limited knowledge of and reservations about VCA
The group discussions also exposed limited understanding of VCAs generally, as well as more specific reservations about VCA donation. Apprehensions centered on bodily mutilation and the loss or transfer of identity.
Bodily mutilation
The discussions evoked vivid reactions about bodily mutilation not typically seen in discussions about solid organ and tissue donation. Distinguishing VCAs as externally visible, a 51-year-old Black woman said, For me, out of sight out of mind. You take my organs, you’re talking inside. They’re covered up. I can’t see them. You have something tangible that I can touch, and I can see. I think that would be too much for me to deal with. I couldn’t do it. (P1, FG5)
A 37-year-old Black participant agreed and explained her strong reluctance about hand donation, stating, Because, they can take your hand! You’re being disfigured. So I feel like that’s a lot different from taking your heart which is like, you’re sewed back up and you can’t see any of that . . . I don’t want to be ripped apart and sliced and diced. (P1, FG1)
Mutilation concerns within the context of funeral plans, including viewings and wakes, were also commonly discussed. A Middle Eastern woman, age 26, noted, I think I could see this being a lot harder for people’s families to accept if you have any sort of tradition of viewing the body or cleaning the body before a funeral. I think internal organs you don’t see when you’re [donating]. I think there could be people’s family members that could have—I guess—a lot more of a hesitation because [a VCA] is more visible. (P7, FG2)
A Black woman, age 63, reiterated, “I don’t wanna go to my son’s funeral when his face ain’t there” (P2, FG5). Similarly, an 18-year-old Latina remarked, “No parent wants to see their child get cut up or like missing a hand . . . I don’t want my family to see my children all cut up and all ugly like that, I can’t” (P10, FG6).
Transfer and loss of identity
Loss of the VCA donor’s identity was a significant concern, with participants least receptive about face donation for this reason. A Black woman, age 61, explained, I struggle with the face probably more than anything. Something about a face is to me the biggest genetic representation of your parents more so than your hands or your feet or anything like that. If you put my feet and my sister’s feet in a line up they’d . . . be different but nothing distinguishing about either one as opposed to our faces. (P4, FG1)
Respondents were distressed that the face—a defining feature of one’s identity—could be transplanted on another individual. A 60-year-old Black woman explained, “I don’t want to walk down the street and see the exact face of my loved one because it’s been transplanted to somebody else” (P2, FG2). Face recipients were commonly believed to appear either similarly or identically to their donors.
Risk versus reward in receiving a VCA
The discussions revealed a general unwillingness to receive a VCA, although 85% of participants reported a willingness to receive a solid organ transplant in the survey. In addition to issues described above, participants cited concerns that an intensive recovery would outweigh an allograft’s potential benefits. A 64-year-old White woman explained, If I thought there was going to be a prolonged recovery period that was miserable, I think I would probably rather do without. Because I would begin to wonder if my emotional life would be so compromised, that it wouldn’t be worth it. (P5, FG4)
Others were concerned about their advanced age, with one 71-year-old White woman saying, I’m not sure. I mean the fact right now that I’m now in my 70s, I don’t really know whether I think it would be worth it at this point. If I were younger, absolutely, or for my sons or whatever, absolutely. But I mean I think at this point, I might be able to sort of get by without having a limb. (P6, FG5)
An Asian participant, age 22, was concerned about acquiring a donor’s characteristics. She said, Just thinking about me living with another person’s organ or body part is a bit uncomfortable because I think that sometimes, in some cases, other people’s traits get mixed up with yours—like you gain like new traits or something. . . I don’t know if I want to change. (P6, FG1)
Information needed to authorize VCA donation
In order to make an informed decision about donating a VCA, participants wanted more information, including details about the potential recipient, expected procedure outcomes, impact on funeral arrangements, and the possibility of contacting the recipient. For instance, a White woman, age 29, explained, “I could lean more ‘yes’ to being willing . . . providing that I know more specifically where [the donated VCA] may be going” (P3, FG1). Speaking specifically about the age of the recipient as a decisional factor, a Black man, age 57, said, “It depends on what stage of life you’re in. It’s a big difference if a five- or ten-year old kid [needed a VCA] or seventeen or twenty-something adult versus a 55- or 75 year old person” (P7, FG4). A 65-year-old White participant explained that she would want to know “What it would improve. Or how much and in what ways it would improve someone’s life” (P9, FG4). Regarding funeral arrangements, a 68-year-old Black woman asked, “If they’re not going to be cremated, will you have to let them know you’ll have to have a closed casket for a funeral, all that stuff so they can take it in before they make a final decision?” (P2, FG1). The extent of contact between recipient and donor families was also of significant interest. A 60-year-old Black woman asked, “So with VCA is that same option given where you can reach out to the donor’s family to say thank you or is that anonymity there?” (P2, FG2).
Potential donor’s wishes
Participants were also reluctant to authorize a VCA donation on behalf of a loved one when the decedent’s wishes were unknown. The primary concern was that a donor may have neither known about VCA donation nor expressed any support for it. A Black man, age 57, explained, “If we talked about it before they passed away, then I would do it. But if they never agreed or never talked about it and discussed it, then I’m more inclined not to” (P7, FG4). Others mentioned that surrogate decisions would be more difficult than personal ones. A 22-year-old White woman stated, “If it’s my mom, I know she wants to donate her organs, but I don’t know if she wants to go this far. Like I think that would be a harder choice for me to make” (P5, FG5). Respondents seemed to not extrapolate wishes concerning donation of more common organs, such as kidney and heart to wishes concerning VCA donation.
Attitudes toward donation
Survey responses indicated a moderate to strong willingness to donate solid organs upon death (Table 2). Over half of the sample were registered organ donors. Comparatively, slightly less than half of participants expressed a willingness to enroll in a VCA donation registry. When surveyed about donating a family member’s organs and tissues, willingness declined to 41.5%, with most indicating that they would do so only if they knew their family member supported donation.
Disposition toward donation.

NR: no response.
Participants offered similar reasons for supporting solid organ, tissue, and VCA donation, including making “something positive come out of death” (Table 3). Group discussion revealed that comfort with donating solid organs, tissues, and VCAs resulted from the belief that they would not be needed after death. For example, a 68-year-old woman stated, “I won’t need them anymore once I’m gone. So, somebody else can live on with my organs” (P2, FG1). An Asian man, age 24, agreed saying “Oh, I don’t care, I’m dead” (P4, FG6).
Organ donation attitudes from pre-focus group surveys.

Five-point Likert-type scale: 1 = Completely Disagree, 5 = Completely Agree.
Mistrust of the organ donation system
Black respondents across all focus groups expressed distrust of the US organ donation system, citing historical, systemic racism and the existence of a black market. Speaking of community-held beliefs, a Black woman, age 58 said, “There’s a lot of racial myths that go on. Like they think that if you’re African American, you don’t get a preference towards getting a transplant or that you might be targeted to be a donor” (P3, FG5). Some participants made specific references to the Tuskegee Syphilis Study.
27
A Black woman, age 48, stated, You hear about the Tuskegee. We’ve been used lots of times—as a lot of African Americans are. Like our parents have taught us and their parents have taught us . . . we’ve been experiments for a long time, and it’s starting to creep back into our community again . . . so I think that has a lot to do with our resistance from wanting to do and participate in a lot of things. (P8, FG2)
Mistrust also stemmed from fears of a black market. While participants of other races mentioned this topic, Black participants specifically referred to the illicit organ trade as a dominant, widely held belief in their communities. A 58-year-old Black female participant noted, At least in my group of friends and associates, people are hesitant because there’s the black market that people hear about for organs, and every time someone’s posting [on social media]. People are wondering what’s happening to all these missing young black kids. And I don’t know for sure there’s a black market, but I’m not gonna say there isn’t either. (P3, FG2)
Discussion
In addition to the 22 patients currently waitlisted for VCAs, there are millions of Americans living with limb loss or severe facial disfigurement and over 1600 service men and women living with single or bilateral injuries 28 for which VCA transplantation may be a viable treatment option. To ensure this therapeutic option is available to all Americans in need, concerted effort must be made to increase both first-person and family authorization of VCA donation, an option typically offered to FDM upon the death of family member and after asked to donate solid organs and tissues for transplantation and research purposes. This investigation explored the general public’s attitudes, beliefs, and knowledge about VCA transplantation using a mixed-methods design. Our findings support those of other large survey studies of VCA13–16 while generating novel information on the rationale behind VCA attitudes and behaviors.
General knowledge about VCAs was low. Descriptions of VCA transplantation provided by the moderator were met with astonishment but also a hesitation for personal and surrogate VCA donation. While all participants were familiar with solid organ and tissue donation, there was progressive decline in knowledge from solid organs to tissue to VCA. Group discussions revealed the general public is largely unaware this new type of transplantation exists and elicited novel concerns about VCA donation distinct from those cited for other donation types. All participants exhibited limited VCA knowledge despite its coverage in the mass media.29–31
For most participants, support of organ and tissue donation was grounded in a belief that the act of donation makes something positive come out of death, reinforcing past findings on organ and tissue donation. 32 Consistent with prior research on organ and tissue donation,32–34 respondents supportive of VCA donation also expressed a desire to help others in need and the belief that they would no longer need their body after death. Another factor contributing to willingness to donate was knowing the potential donor’s wishes. Yet, while 56.5% of the sample were registered organ, tissue and eye donors, only 49.0% were willing to join a registry specifically for VCA donation.
Specific concerns about VCA donation were also revealed. While bodily mutilation has been noted as a source of reluctance for solid organ and tissue donation,21,33–36 respondents reacted more viscerally to the idea of the donor being “cut up,” evoking imagery from horror films. Participants further distinguished VCA donation from solid organ and tissue donation, stating the former is visibly obvious. This concern was also discussed in relation to burial practices and the ability to have open casket funerals. While posthumous prosthetics may acceptably substitute for a donated hand, foot or limb, face donation precludes a viewing. In addition, respondents expressed unease about face donations, associating faces as critical markers of identity. Participants expressed concern about seeing their loved one’s face on a stranger, not knowing that face grafts assume the underlying bone structure of the recipient and would bear little to no resemblance to the donor. They also felt strongly that a loved one’s hands would be identifiable. These concerns are unique to VCA donation.
Black participants expressed a distinct mistrust of organ and tissue donation across all focus group sessions, more so than any other racial/ethnic group sampled. Mirroring well-documented concerns among this population,37–41 respondents across generations pointed to a belief in a black market of organs and systemic racism that targeted and manipulated Black Americans, citing the Tuskegee Syphilis Study specifically. Clearly, medical mistrust remains a major barrier to organ donation among Black Americans, despite decades of public awareness campaigns and interventions targeting this community.38–51 Future research that examines and tests culturally targeted and acceptable messaging during VCA donation discussions may help to address Black families’ hesitance about solid organ and tissue donation and may make VCA donation better received among Black communities.
These findings have implications for both public education about VCAs and VCA donation discussions. Limited knowledge about VCAs demonstrates a clear need to increase public awareness of this treatment option, which would make VCA donation as familiar and commonplace as organ and tissue donation and dispel its likeness to astounding technological advancements only found in science fiction. A recent study reported increased willingness to donate facial allografts after exposure to an educational video on the topic. 52 However, most available public education materials do not adequately address concerns regarding transference/loss of identity, bodily mutilation, and the possibility of recognizing face donors. 53 Improving public awareness may also stimulate conversations among families/kin, thus making potential FDMs aware of their loved ones’ VCA donation wishes, which was noted to be a major decisional factor (Theme 4) by participants in this study. Furthermore, increasing public conversations could increase VCA authorization or increase FDM comfort/confidence in their VCA donation decision-making. Inserting VCA into the American lexicon may also reduce families’ initial surprise and confusion if approached for VCA donation. Future public education campaign messaging should underscore VCAs’ benefits, while preempting concerns identified in this study. To be most effective, these campaigns should utilize interpersonal channels for communicating information about VCA donation and provide an opportunity for enrollment on a registry. 54
OPOs training donation professionals to effectively communicate the VCA donation opportunity to families of deceased potential donors should consider the unique challenges of the process. Our recent work has found that current VCA donation approaches are neither uniform throughout the United States nor are there sufficient existing resources for donation professionals to successfully lead such discussions. 12 Moreover, the positive, curious reactions espoused by participants when first learning about VCAs indicates that the wider public may respond similarly, which could be leveraged to introduce and encourage VCA donation as a unique opportunity for substantially improving potential recipients’ lives. Incorporating VCA-related questions and concerns into future training for donation professionals is likely to create higher levels of comfort, confidence, and competence in their communication with FDM.12,22,23,35,55–57 Evidence-based training that provides suggested language and communication techniques for allaying families’ concerns would ensure donation professionals are well equipped to obtain family authorization and support families’ VCA donation decision-making process.
The strengths of this study include the mixed-methods approach, which yielded rich, nuanced data to fill an important gap in our understanding of public perceptions of VCA donation, and the relatively large sample size (N = 53). The study also has limitations. First, the sample was drawn from a single metropolitan area. In addition, over half of participants had at least a 4-year college degree, a considerably higher proportion than the general population (21.3%). 58 The sample was predominantly female. Furthermore, recruitment messaging stated that focus group participants were needed for research about organ donation. As such, selection bias is possible. Respondents in a more generalizable sample of the population might express even less knowledge about and support for VCA donation, and even greater hesitancy about donation of VCAs.
This mixed-methods study highlights unique concerns and questions about VCA donation in general and multiple types of VCAs not previously identified in past studies. As with solid organs and tissues, authorization of VCAs in the hospital remains the primary way to ensure an adequate supply for those in need and the only means of growing VCA transplantation as a treatment modality. The results support the need for initiatives to raise public awareness about VCAs, as public acceptability of and the ultimate authorization of VCAs are prerequisite to the continued development of vascularized composite allotransplantation as a transplantation subfield.
Footnotes
Author contributions
Heather M Gardiner participated in research design, writing of the paper, and data analysis. Ellen E Davis participated in research design, the performance of the research, writing of the paper, and data analysis. Gerard P Alolod participated in research design, the performance of the research, writing of the paper, and data analysis. David B Sarwer participated in research design, writing of the paper, and data analysis. Laura A Siminoff participated in research design, writing of the paper, and data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the US Department of Defense (grant numbers W81XWH-18-1-0680 and W81XWH-18-1-0679).