
Abstract
Vascularized composite allotransplantation is becoming the emerging standard for reconstructive surgery treatment for patients with limb trauma and facial injuries involving soft tissue loss. Due to the complex immunogenicity of composite grafts, patients who undergo vascularized composite allotransplantation are reliant on lifelong immunosuppressive therapy. Decellularization of donor grafts to create an extracellular matrix bio-scaffold provides an immunomodulatory graft that preserves the structural and bioactive function of the extracellular matrix. Retention of extracellular matrix proteins, growth factors, and signaling cascades allow for cell adhesion, migration, proliferation, and tissue regeneration. Perfusion decellularization of detergents through the graft vasculature allows for increased regent access to all tissue layers, and removal of cellular debris through the venous system. Grafts can subsequently be repopulated with appropriate cells through the vasculature to facilitate tissue regeneration. The present work reviews methods of decellularization, process parameters, evaluation of adequate cellular and nuclear removal, successful applications of perfusion decellularization for use in vascularized composite allotransplantation, and current limitations.
Introduction
Severe injuries to the limbs and the face require reconstruction. Autologous transplantation or amputation with subsequent prosthesis in the context of limb injury has significant disadvantages.1–5 Soft tissue and volumetric muscle loss of the face lead to poor patient satisfaction and quality of life. 6 Transplantation of autologous muscle and fasciocutaneous flaps is limited by availability of donor tissue and requires two surgical sites, increasing the procedural risk and often causing donor site morbidity.2,7 Prosthetics often have unsatisfactory aesthetics, limited functional capacity, and no physiological integration. 3 Introduction of foreign material can cause fibrous scar tissue with inferior biomechanical properties to native tissue. 5
Vascularized composite allotransplantation (VCA) is the emerging standard for reconstructive surgical treatment for patients with limb trauma, and soft tissue and volumetric muscle loss. It allows for composite grafts to be transplanted from immunologically compatible donors.2,7 The transplantation of grafts with intact vasculature enables maintenance of metabolic demands, limiting the risk of tissue ischemia and necrosis.8,9 A limitation of VCA remains that transplant recipients must be reliant on lifelong immunosuppressive therapy.2,4,6 This is true regardless of the immunologic compatibility of the donor due to the complex varied immunogenicity of the different tissue types. 4 Immunosuppressants have long-term and potentially life-threatening adverse effects including an associated risk of neoplasm, opportunistic infections, lymphoproliferative disorders, and end-organ toxicity, uncertain mean graft survival time and reinnervation challenges.4,6
Decellularized extracellular matrix scaffold for VCA
Extracellular matrices (ECMs) hold significant promise for bio-scaffold technology. ECMs are comprised of crucial proteins, growth factors, and signaling cascades that provide tissues with structure, and the capacity for cell adhesion, migration, proliferation, and regeneration.10,11 The innate complexity of the composition and function of the ECM cannot be replicated with synthetic materials. 11 ECM scaffolds with adequately retained growth factors and structural proteins, including elastin, collagen, vascular endothelial growth factor (VEGF), laminin, and sulfated glycosaminoglycans (sGAGs), provide the opportunity for novel therapeutic techniques. 2
There is great potential for reducing VCA immunogenicity through implementing decellularized ECM bio-scaffolds as allogeneic transplantation grafts.1,2 Removing cellular and nuclear content from donor tissues while preserving key ECM contents minimizes the immune-mediated host inflammatory response while maintaining adequate structure and regenerative potential. 5 Since cellular and nuclear contents are proinflammatory, removal of cellular content would decrease recipient graft rejection.1,2,12 The preservation of ECM components allows for retention of specific tissue composition, biologic activity, and mechanical integrity. 1 Acellular, tissue-specific ECM bio-scaffolds can generate appropriate spatiotemporal and biochemical signaling to promote tissue regeneration and host endogenous stem and progenitor cell differentiation.1,13,14 The ideal graft for remodeling would be sufficiently decellularized, decontaminated from bacteria and endotoxins, and in contact with healthy surrounding vascularized tissue.2,15 The vascularized graft would subsequently enable recellularization with cell populations including stem or progenitor cells through the native vasculature, further enhancing regenerative potential.
Recipient characteristics including age, comorbidities, and immunocompetence status would likely influence the success of transplantation. 2 Similarly, the ECM composition, surface topography, degradability, structure, and mechanical properties (importantly elasticity and compliance) could influence graft functionality and regeneration. 2
Ultimately, the application of ECM bio-scaffolds for VCA could result in non-immunogenic, tissue-specific graft transplantation that retains 3D architecture, promotes vascularity, and provides opportunity for regeneration. 1 This article provides a review of current literature on perfusion decellularization for VCA.
Methods
Eligibility criteria
Applied inclusion criteria were studies that detailed: perfusion decellularization of composite grafts; perfusion decellularization of connective tissue flaps; perfusion decellularization agents or parameters; methods to assess success of decellularization; comparison of decellularization methods to perfusion; strategies to improve decellularization efficiency, efficacy, and regenerative potential. Exclusion criteria were studies focused on whole-organ decellularization not otherwise meeting inclusion criteria; analysis of commercially available acellular grafts; creation of ECM hydrogels; decellularization solely via methods other than perfusion.
Information search
An electronic search was conducted in PubMed/Ovid Medline, Scopus, and Google Scholar databases from January 2012 to June 2021 limited to English language publications with available full texts. Published articles on relevant topics were found using the following keywords alone or in combination: vascularized composite allotransplant*, VCA, perfusion decellulariz*, decellulariz*, ECM scaffold, extracellular matrix scaffold, limb transplant*, face transplant*, extremity transplant*, ear graft, detergent, muscle graft, fasciocutaneous, adipose, and skin flap.
Study selection
Initial article selection was completed through review of titles and abstracts of all articles. Subsequently, the full texts were reviewed for inclusion and exclusion criteria.
Results
Figure 1 summarizes the results of the literature search and study selection. The initial search yielded 1081 unique articles, and upon review, 68 met the criteria for inclusion.

Summary of search results from database and study selection based on eligibility criteria.
Methods of decellularization
There are several methods and agents used for decellularization of ECM composite tissues. The most effective method largely depends on the clinical application, and the characteristics of the tissue, including the cellularity, density, lipid content, and thickness. 10 The ultimate goal of each method is to cause cell lysis, separation of cells from tissue, and removal of cellular debris. 16 Common decellularization agents and techniques are described in Table 1.

CHAPS: 3-((3-cholamidopropyl) dimethylammonio)-1-propanesulfonate; ECM: Extracellular matrices; EDTA: Ethylenediaminetetraacetic acid; EGTA: ethylene glycol-bis(β-aminoethyl ether)-N, N,N′,N′-tetraacetic acid.
Perfusion decellularization is generally the method of choice for decellularization of composite grafts, as it allows for control over reagent flow rate, venous outflow, and minimal required detergent diffusion distance. Thus, it enables access to all tissue layers and results in improved removal of cellular debris, and preservation of the 3D architecture. Since the vascular network is designed for optimal delivery of oxygen to cells, it is an efficient conduit for targeted detergent delivery and removal of cellular debris.8,9 In comparison, agitation distributes reagents poorly in thicker grafts due to diffusion limitations, pressurized systems cause ECM protein denaturation and retention of debris, freeze/thaw cycles have poor cellular removal, and supercritical CO2 is not always feasible for delicate vasculature.9,21–23,26,27
Chemical detergents, with or without supplementary enzymatic treatment, are the most commonly used decellularization agents for VCA grafts. Acidic and alkaline perfusates are less disruptive and immunogenic than chemical detergents; however, they are relatively inefficient at cellular removal and swelling can cause loss of GAGs and viscoelasticity.9,26 Extreme pH can cause further ECM damage. 28 Hypertonic, hypotonic, or enzymatic agents alone are insufficient to achieve decellularization, and trypsin targets collagens, significantly decreasing mechanical strength.9,26 Chemical detergents include non-ionic detergents, such as Triton X, ionic detergents, such as SDS, and zwitterionic detergents, such as CHAPS. Non-ionic detergents disrupt lipid–lipid, lipid–protein, and DNA–protein interactions, ionic detergents solubilize cell and nucleic membranes, and zwitterionic detergents demonstrate ionic and non-ionic properties. 29 The impact on cell removal and ECM preservation for each solution is summarized in Table 2.
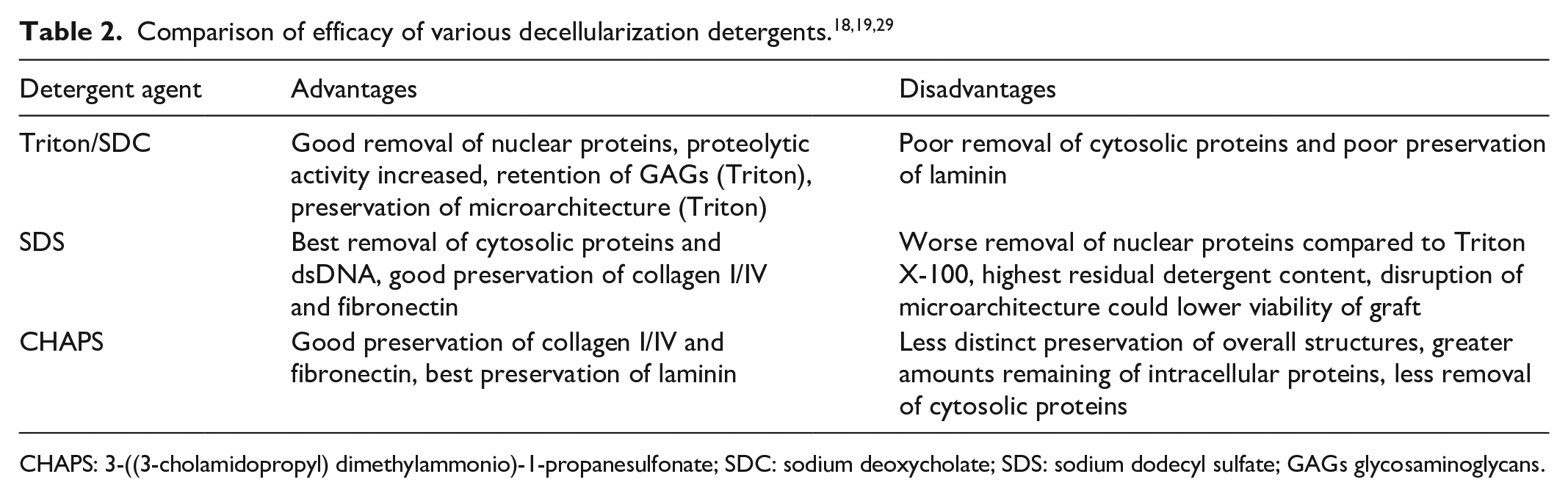
CHAPS: 3-((3-cholamidopropyl) dimethylammonio)-1-propanesulfonate; SDC: sodium deoxycholate; SDS: sodium dodecyl sulfate; GAGs glycosaminoglycans.
Milder zwitterionic detergents have been found to be effective for decellularization of thin tissue organs. However, their efficacy is minimal with the thicker tissues in VCA grafts. 10 In contrast, Triton X-100 and SDS are more effective at decellularizing thicker tissues.18,19 SDS is the most effective detergent agent for cell removal; however, it is the most disruptive to the ECM microarchitecture.18,19,29
Polar solvents, such as isopropanol (IPA), are often required for sufficient delipidization of high adipose content tissues.10,11,30 A study conducted on the decellularization and delipidization of processed porcine skin analyzed the impact of IPA on cellular removal and lipid content. 11 Results indicated that IPA removed more lipids, preserved ECM proteins and growth factors, and increased cellular removal. 11
Terminal sterilization of the scaffold is required to prevent microorganism contamination thus preventing proinflammatory macrophage activation 16,24 Sterilization techniques include use of solvents, acids, antibiotic solutions, HHP, supercritical carbon dioxide, depyrogenation, ionizing radiation, and ethylene oxide exposure.16,24 Gamma radiation for sterilization has further been proven to partially regenerate mechanical properties (tensile strength and elastic modulus) and decrease biodegradation of the decellularized graft, while retaining physiologic and structural properties. 24
Perfusion decellularization parameters
The pressure and flow rate of solution delivery and the concentration of the agent have implications on the success of perfusion decellularization. 10 Constant, low-physiologic pressure perfusion allows for optimal preservation of the native matrix.1,10 The vascular resistance does not remain constant throughout the process, since the initial presence of more cellular content creates higher resistance. 10 As such, many procedures deliver lower or intermittent flow rates initially to avoid mechanical stress damaging the ECM or vasculature basement membrane.1,10 Vascular resistance is also dependent on viscosity, and thus the concentration of the perfusate. 10 Therefore, resistance is variable if the solution composition or concentration is not constant. Graduated flow rates are often applied to prevent inappropriately high mean arterial pressure in the vasculature initially, while minimizing exposure time once the resistance drops with cellular removal. 10 The use of low-physiologic pressures reduces the risk of compartment syndrome in limbs.1,10
Evaluation of ECM scaffolds
Several histology, immunohistochemistry, immunofluorescence, and imaging techniques can be applied to evaluate the effective removal of cellular content and preservation of ECM proteins, growth factors, and cytokines after graft decellularization.1,4,31 It is accepted that decellularization techniques cannot successfully remove 100% of cellular material. Decellularization is predominantly measured via quantification of DNA exists across tissue and cell types, is quantifiable, and provides a reference level for other cellular components. 31 The generally recognized minimum criteria for adequate decellularized are as follows: < 50 ng double stranded DNA (dsDNA) per mg ECM dry weight, < 200 bp DNA fragment length, and lack of visible nuclear material in sections stained with DAPI or hematoxylin and eosin (H&E). 31 Time of flight secondary ion mass spectroscopy has been explored as a technique to quantify cellular remnants and residual detergent fragments. 29 Another method of evaluating decellularization is establishing modulation of the immune response, to ensure minimal reliance on immunosuppressive therapy. Adequate anti-inflammatory and immunoregulatory properties of the decellularized graft can be confirmed through phenotypic and functional polarization of macrophages toward M2, rather than M1, and negative staining for major histocompatibility complex-I (MHC-I) cellular antigen, nuclear antigens, and damage associated molecular patterns.32,33
There is no consensus on criteria to satisfy adequate maintenance of ECM mechanical properties. However, the removal of collagen decreases mechanical strength and the removal of GAGs impacts viscoelastic properties. 4 Grafts are often accessed via imaging and microscopy for maintenance of the 3D architecture, biomolecular patterning, and bioactivity. 4 Further methods to assess mechanical properties include measurement of tensile stress, elastic modulus, and mechanical strength.3,34 Vasculature preservation and patency can be evaluated using contrast computerized tomography (CT), fluoroscopy, radiography, or micro-CT, or re-perfusing the graft at physiologic pressures.1,4,6,35–37
Perfusion decellularization in VCA
Perfusion decellularization has been successfully applied to several solid organs for transplantation, including hearts, livers, lungs, kidneys, pancreases, porcine small bowels, and bladder smooth muscle.1,4,28,38,39 Emerging research shows potential for the application of ECM bio-scaffolds for VCA. Composite grafts are more challenging to decellularize, due to the many cell types and structural elements present in the varying tissue layers. Examples of successful perfusion decellularization of composite grafts for allotransplantation that reduce cellular material, maintain vascularity and structural support, and provide regenerative potential are outlined below.
Skeletal muscle decellularization
Skeletal muscle is challenging to decellularize, and to regain function upon recellularization due to the highly organized structure, contractile elements, and numerous vessels and nerves. 40 Several studies have analyzed isolated skeletal muscle decellularization.15,40–44
Sabbagh et al. 42 developed a decellularization protocol using SDS and Triton X-100 perfusion with Krebs–Henseleit buffer through the femoral artery for 5 h to produce an acellular superficial gracilis graft. They achieved 98% reduction in DNA content, while maintaining ECM components and preserving vascular patency. The tensioactive Krebs–Henseliet buffer allowed decellularization through cell membrane dissolution while preserving the matrix elasticity. 42
Porzionato et al. 40 decellularized human, rat, and rabbit skeletal muscle using SDC and DNAse supplemented with Triton X-NH4OH. They effectively removed all muscle fibers and myofibril elements, and preserved collagen, elastin, GAGs, and vascular patency, with an average final 10 ng dsDNA/mg dry weight. Mechanical properties of the decellularized muscle compared with native tissue showed normal stress versus strain relationships. The grafts were integrated into a rabbit abdominal wall defect with no signs of local or systemic graft rejection. Integration occurred mainly through reparative rather than regenerative mechanisms. 40
Zhang et al. 41 assessed the bioactivity and functional capacity of decellularized skeletal muscle from a porcine rectus abdominus flap using perfusion with trypsin, SDS, Triton X-100, peracetic acid, and DNAse through the inferior epigastric vessels. They preserved the 3D architecture, vasculature, neural channels, ECM components, and mechanical strength. The grafts were used to treat an abdominal wall defect. Analysis of neural channels within the muscle graft showed long ovoid nuclei, similar to Schwann cells, at 8 weeks post-surgery. The rectus abdominus tissue showed some ability for neovascularization and skeletal muscle regeneration. 41 In further work, they identified key steps for successful muscle decellularization including: isolating grafts with fully intact, perfusable microvasculature; catheterizing main vessels to ensure adequate blood flow; carefully sterilizing equipment and materials; and using subsequent rather than simultaneous perfusion of arteries and veins to remove residual detergent and debris. 15
Raffa et al. 43 decellularized rat legs by perfusion of 0.25% SDS through the abdominal iliac artery and subsequently isolated decellularized skeletal muscle to characterize its composition. The scaffolds preserved muscle-specific proteins for ECM remodeling and notably contained proteins that facilitate nerve regeneration through modulating neurite elongation and axon growth. 43
Urciuolo et al. 44 compared functional muscle regeneration of rat lower limb muscle decellularized by perfusion of the abdominal iliac artery with Latrunculin B (LatB), detergent enzymatic treatment (DET), or SDS. All agents created scaffolds that promoted neurogenic regeneration, angiogenesis, and host cell migration and differentiation. SDS removed more myofibril components; however, the ECM organization and component preservation with SDS are thought to have contributed to improved myofibril alignment and function upon regeneration. 44
An infusion decellularization study suggested that the addition of minced muscle autograft to decellularized allogenic skeletal muscle could improve contractile forces. 45
These studies show great promise for skeletal muscle recellularization.
Fasciocutaneous flap decellularization
Several adermal skin matrices have been developed; however, due to the lack of a perfusable vascular network, they cannot be used for functional full-thickness grafts.7,46 Zhang et al. 4 and Jank et al. 47 have both developed acellular full-thickness fascicocutaneous flaps through perfusion decellularization.
Zhang et al. 4 combined freeze-thaw methods and perfusion with detergent and enzymatic agents through the femoral arteries to achieve decellularization of rat skin and adipose tissue groin flaps. The flaps were subjected to three freeze-thaw cycles (−80° C) and subsequently perfused with 0.25% trypsin/EDTA and 1% Triton X-100. Staining showed adequate cell removal and preservation of GAGs, VEGF, collagen in adipose tissue, and laminin in vessels, nerves, and nanofibrous structures. Three-dimensional architectural characterization and scanning electron microscopy (SEM) showed well-preserved structure and patent micro-network. 4 Regenerative potential and immunogenicity were assessed through reseeding and transplantation into a rodent recipient. Initially, transplantation caused CD68-positive macrophage infiltration, followed by co-M1 and M2 presence, and finally predominantly M2 macrophages at 3 months post-transplant. 4 Dermal tissue showed degradation and remodeling as adipose.
Jank et al. 47 decellularized porcine groin fasciocutaneous flaps via perfusion of the superficial femoral and saphenous vessels with 1% SDS for 10 days and 1% Triton X-100 for 1 day. Histology, microscopy, and immunofluorescence proved removal of nuclei, preservation of dermal and subcutaneous structure, and retention of elastin, laminin, collagen I, and collagen III. dsDNA content was reduced by over 75%. 47 Mechanical properties were compared to available adermal matrices and native skin showing comparable stiffness as determined by Young’s modulus. 47 Regenerative potential of the skin’s protective function was assessed through both in vitro reseeding with human keratinocytes and in vivo implantation into a full-thickness skin graft. 47
Trypsin paste may enhance hair follicles removal during skin decellularization. 48
Nerve decellularization
Porcine sciatic nerve grafts were decellularized by perfusion with SDS, Triton X-100, and type 1 bovine DNAse through the medial circumflex femoral artery. 13 The dsDNA content was reduced to 20.6 ng/mg dry weight, and nuclei were removed from the nerves; however, the surrounding connective tissue retained some nuclear content. 13 Collagen, sGAGs, and laminin were maintained, and neurotrophic growth factors were detectable at decreased levels. 13
Decellularizing with elastase and storage at cold temperatures may improve motor and sensory function.49,50
Human penile decellularization
Tan et al. 51 successfully decellularized a complete human penile organ using 1% SDS delivered via combined micro-arterial perfusion, urethral catheterization, and external diffusion. Micro-CT showed preservation and patency of the complex vasculature network. DNA content was reduced to 33.3 ng/mg tissue. Histology proved adequate retention of collagen, fibronectin, laminin, and growth factors. The scaffold biocompatibility was assessed through reseeding with human adipose-derived stromal vascular cells. 51 Further experimentation focusing on differentiation and reseeding with multiple cell lineages is necessary to produce a penile allograft that can restore cosmetic, urinary, and sexual function.
Facial decellularization
Duisit et al.6,52 attempted decellularization of deceased human face grafts and subsequent lip recellularization. A proof of concept study was performed using porcine ears.
The porcine ears were cannulated at the caudal auricular artery and perfused with subsequent solutions of adenosine, 1% SDS, 1% Triton X-100, and type 1 DNAse. 52 Results showed absence of cellular and nuclear material, with 93% reduction of DNA content. ECM components were preserved, including collagen, proteoglycans, GAGs, elastin, reticular fibers, and laminin on the dermal side. Mechanical properties were assessed for cartilage rigidity and skin elasticity, with a resulting 13.8% reduction in Young’s modulus. 51 Adequate immunogenicity was proven through transplantation into porcine peritoneum. Vascular patency and integrity were demonstrated by re-anastomosis to the common carotid artery and internal jugular vein and subsequent reperfusion at physiologic pressure. 52 Regeneration potential was shown through reseeding disks and whole grafts with fibroblasts and bone marrow mesenchymal stem cells. Results showed poor cell density with increased lipid content, however, cell migration, proliferation, and organization was adequate. 52
Before attempting the process using human face grafts, the team applied their findings to a rodent hemifacial graft model, with similar results. 35 Notably, in the rat models, cartilage cellular content removal was not satisfactory with immersion treatment as compared to perfusion. 35 Additional studies were performed on human ear grafts, and a polar solvent step was added to remove adipose content. 37
The research group adapted their decellularization protocol for human face grafts, including the polar solvent step. 6 Five segmental face grafts, including lips, cheeks, and nasal structures, and one full face graft were tested. The facial arteries of the segmental grafts, and both the facial arteries and the superficial temporal arteries of the full face graft, were cannulated.6,36 Perfusion decellularization was achieved using detergent, alcoholic, and enzymatic agents in three subsequent steps: 1% Triton X-100, 2-propanol (stir bath and perfusion), and type 1 bovine DNAse. The resulting decellularized face grafts showed patent vasculature throughout. 6 Reperfusion ability at physiologic pressure was proven by heterotrophically re-anastomosing the facial arteries to the abdominal aorta and inferior mesenteric artery of a porcine recipient. The full face graft was mock transplanted onto the initial donor, showing preservation of facial morphology with nasal cartilaginous support. Cellular content was removed and DNA content was reduced 97%, with longer fragments remaining in cartilage and muscle. MHC-I antigen staining was negative. Laminin was preserved in muscles, and collagen IV was retained in skin. There was a significant reduction of elastin and GAGs in skin, mucosa, and muscle, with partial preservation in fat and cartilage. Most cytokines and growth factors were significantly reduced in all tissue types, with the best preservation in adipose. Recellularization was attempted through static cell seeding of lip disks with dermal fibroblasts and myoblast progenitors, and through bioreactor seeding of full upper lips with either myoblast progenitors or human aortic endothelial cells. Both recellularization methods showed some cell survival and attachment to the ECM; however, cells mainly clustered around the ECM surface with limited deeper migration. 6 The study concluded that perfusion decellularization of a complex face graft is possible. Further investigation is required for adequate regeneration with preserved functional capacity.
Limb decellularization
Jank et al. 3 performed perfusion decellularization with SDS and Triton X-100 through cannulated brachial arteries of rodent and primate upper limbs, and repopulated the limbs with muscle progenitors, endothelial cells, and mesenchymal cells. The limbs were decellularized with 1% SDS for 50 h and 1% Triton X-100 for 1 h. Histology showed removal of cellular components and preservation of tissue architecture and structures. Endomysial sheets around muscle fibers were preserved. Vasculature remained patent, and no significant deterioration in mechanical, mineral, and geometric bone characteristics were observed. Results showed 90% removal of DNA content, 40% retention of sGAGs, and preservation of collagens and GAGs. 3 Recellularization was performed over 21 days using a biomimetic bioreactor system with vascular perfusion and electrical stimulation to improve the formation of functional muscle. Myoblasts were injected into the matrix, and the functionality and vascular patency were assessed with isometric force measurement and orthotopic limb transplantation. The electrical stimulation during the growth and differentiation phase improved cell alignment along endomysial sheets allowing for functional muscle formation. 3
Gerli et al. 1 investigated the decellularization of a human upper limb by perfusing the brachial artery with SDS and Triton X-100 using a bioreactor decellularization chamber set-up. The extremity was explanted 24-h postmortem from a 57-year-old male donor without diabetes, obesity, infectious diseases, or prior chemotherapy treatment. After performing bilateral fasciotomies to protect against compartment syndrome, the brachial artery and vein were cannulated for perfusion and to monitor outflow, respectively. The limb was decellularized with 1% SDS for 30 days and 1% Triton X-100 for 15 days with graduated flow rates. Isolated biopsies were treated with nuclease. 1 The vascular architecture and patency were preserved. Intracellular structures including muscle sarcomeres, peripheral nerve axons, and vascular smooth muscle were sufficiently removed, as were cell nuclei from muscle, nerve, skin, and vascular compartments. Bone marrow was removed from trabecular bone with preservation of structural bone elements. Collagenous structures were mostly preserved, and elastin was adequately retained in skin and vessels. Overall, there was an average 4.6-fold reduction in dsDNA, with better removal in skin, vessels, and nerves exposed to higher detergent concentration. 1 Perfusing the vasculature with nuclease may have increased dsDNA removal. 1 Although the study outlined several limitations for perfusion decellularization of human allografts, it indicated the feasibility for large-scale ECM bio-scaffold use in VCA.
Next steps and limitations
Extracellular matrix damage
A significant challenge with perfusion decellularization is achieving adequate cellular removal without causing extensive ECM damage. SDS is widely considered the most effective agent at reducing cellular content. However, its ionic strength can destroy the non-covalent interactions of native ECM proteins, resulting in denaturation and loss of function.9,53,54 Failure to preserve collagen, GAGs, elastin, and VEGF can reduce mechanical properties and limit regenerative potential. 26 SDS destabilizes the collagen triple helix and swells elastin fibers, disrupting the mechanical integrity and decreasing the capacity for cell signaling and adhesion during recellularization.8,53,55 GAGs are particularly targeted due to their positioning in the cell membrane, thus affecting the growth factor binding and water retention that contribute to ECM biocompatibility.26,55 The high affinity of SDS for proteins increases residual detergent after washing. However, rinsing with a non-ionic surfactant such as Triton X-100 can help eliminate residual detergent.8,9,26,55
Techniques to prevent excessive ECM structural damage or to regenerate ECM potential after deceullarization have been studied in whole organs. The most commonly employed techniques include limiting exposure time to SDS through novel experimental designs, or repairing structural damage through crosslinking.
Poornejad et al.53,55 successfully maintained ECM structure and function through perfusion decellularization of porcine kidneys with SDS by implementing a freeze-thaw cycle, osmotic shock to the cellular membrane, isobaric incremental increases in flow rate, and low detergent concentrations. The freeze-thaw cycle induced partial cellular membrane damage.8,53 The perfusion process alternated 30-min exposures to a hypertonic solution, SDS, and DI water, increasing the flow rate by 1.5 mL/min every 30 min. 53 The hypertonic solution increased cell removal through osmotic shock to cellular membranes and decreased graft exposure time to SDS.8,53 The constant pressure graduated flow rates reduced structural damage by allowing for low flow at the start of the process when the resistance due to cellular content is the highest. The incremental increase in flow rate minimized SDS exposure. These techniques reduced the SDS contact time from 36 h to 5 h, resulting in total GAGs and soluble collagen preservation of 79.6% and 55.1% as compared to the SDS perfusion only control with preservation of 30.5% and 22%, respectively. 53 Other studies have combined SDS with milder detergents, protease inhibitors, enzymatic agents, or freeze-thaw cycles to achieve decreased tissue contact time with SDS.8,30,48,56–58
Crosslinking between reactive sites among collagens or amino groups is often used after perfusion decellularization of whole organs to improve mechanical properties.59,60 Physical, chemical, or biological crosslinking methods can be applied to improve hardness, tensile strength, elastic modulus, enzymatic resistance to degradation, or anti-oxidation, anti-inflammatory, or anti-calcification properties.58,60 Such mechanical support is necessary for cell seeding, proliferation, and differentiation. 60 Physical methods such as photo-oxidation are difficult to control, and chemical agents such as glutaraldehyde, epoxy compounds, or carbodiimide can cause cytotoxicity, calcification, and ultimately immune rejection.59,60 Glutaraldehyde in particular accelerates calcification, reduces long-term mechanical properties, and depolymerizes, releasing breakdown material and resulting in cytotoxicity. 61
Comparatively, biological agents, such as genipin and proanthocyanidins, are more biocompatible, allowing for elastin crosslinking, inhibition of elastin calcification, facilitation of recellularization, and anti-inflammatory potential.59,60,62,63 Genipin has been applied to crosslink adipose-derived stem cell-derived ECM, resulting in enhanced mechanical properties with less degradation. 62 Crosslinking through radical polymerization of vinyl groups has been shown to preserve collagen and elastin structure while maintaining cytocompatibility. 61
The extent of ECM damage due to detergent decellularization varies across different organs and tissue types. 34 As such, it is unclear if crosslinking could improve mechanical integrity of decellularized VCA grafts similarly to solid organs.
Recellularization
As attempted in some studies, the next steps in determining the viability of ECM bio-scaffolds for use in VCA are recellularization. 1 Optimal cell types for recellularization are tissue dependent.1,10 In vitro studies assessing cell reseeding have shown limitations in cell migration beyond the ECM surface. 6 Better distribution of cells in muscle tissue was observed when myoblasts were injected, however, this technique was disruptive to the ECM structure and resulted in apoptosis at the injection site.4,40 Skeletal muscle is particularly challenging to recellularize; however, perfusion of myogenic progenitors that can cross vessel walls could allow for broader differentiation. 4
Conjugating chemo-attractant growth factors or hypoxia-inducible factors to the bio-scaffold could promote mobilization of endogenous progenitors for regeneration.1,64 This would create a more suitable environment for progenitors to attach to the ECM, migrate to deeper tissues, and differentiate in vitro prior to transplantation. 1 It has been proposed that the use of the recipient as their own bioreactor for regeneration may allow for better cell attachment, migration, and differentiation, and minimize immune response. 6
State-of-the-art techniques
Other state-of-the-art techniques that have been developed for whole-organ perfusion decellularization could further be adapted for VCA. Large throughput or automated valve systems would allow for consistency and reproducibility of the procedure, the use of various reagents implemented at set time intervals, and minimal to no DNA or bacterial contamination.28,65–67 Schilling et al. 65 developed an opensource prototype for a tissue/infusion device with peristaltic pumps, three-way values, and a tissue chamber controlled by customizable software to allow for adaptable, reproducible, and affordable tissue decellularization. The combination of aqueous solutions with supercritical carbon dioxide delivery could decrease decellularization time and increase removal of cells, debris, and residual detergent.28,67 Finally, implementation of biological crosslinking agents or combining decellularization methods to reduce detergent exposure time could minimize ECM damage and improve graft.8,53,55,59–63
Limitations
Feasibility studies using human tissues are limited by specimen availability, as composite graft donation is uncommon.1,6 The grafts must be obtained shortly after the donors are deceased. 1 The most significant limitations for the use of perfusion decellularization and subsequent recellularization of ECM scaffolds for VCA are challenges associated with regeneration of nerves and functional capacity of the muscles. Particularly, there is limited evidence to suggest that skeletal muscle can be effectively functionalized, and few studies have attempted adequate reinnervation of tissue.68,40–42 This is of concern, as a primary goal of transplantation is to regain function of the grafted tissue, to improve the recipient’s quality of life. Novel nerve regeneration strategies may be required to successfully reinnervate perfusion decellularized grafts. These include nerve guidance conduits, chondroitinase, introduction of adipose-derived stem cells, or fibrin glue. 68 Further investigation toward mitigating these limitations could lead to perfusion decellularization of allografts as a clinically meaningful improvement in quality of life for VCA recipients (Figure 2).

Anatomical locations for VCA and possibilities for perfusion decellularization and recellularization prior to transplantation.
Conclusion
Perfusion decellularization and recellularization of vascularized composite allografts holds great promise for prevention of complications related to lifelong immunosuppression. The appropriate decellularization parameters need to be selected in order to maintain the extracellular matrix. Recellularization techniques then become the next challenge for selection of recipient-specific cells or a universal non-immunogenic cell line allowing repopulation of each component within these vascularized grafts. Finally, nerve and muscle regeneration need to be re-established in order to allow for functional organs. This innovative field represents the future of VCA. Due to its complexity, this field remains in its infancy compared to solid organ decellularization and recellularization. Despite the complexity and challenges, there have been several examples as outlined in this review, that have met significant milestones in moving the field forward. In particular, they have been important in identifying the current limitations in the field and the next steps required to address the limitations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.