
Abstract
Objective:
This study was aimed to assess the prevalence of pulmonary tuberculosis and its associated factors among adults living with HIV/AIDS attending Public Hospitals, Shashamene Town, Oromia Region, South Ethiopia.
Methods:
A cross-sectional study was conducted from November 2020 to February 2021 among Adults Living with HIV/AIDS attending Public Hospitals in Shashamene Town, Oromia Region, South Ethiopia. A sputum sample was collected and analyzed using Xpert MTB/RIF assay and blood sample was collected to count CD4 using BD FACSPresto analyzer. Semi-structured questionnaires were used to collect data. SPSS version 25 software was used for statistical analysis and a p value of <0.05 was considered as statistically significant.
Results:
In this study, the overall prevalence of pulmonary tuberculosis among adults living with HIV/AIDS attending the Public Hospitals was 23.5% (5% confidence interval: 18.26, 29.13). Variables such as age range of 50–64 years, female gender, occupation with house wife, and World Health Organization stage (III and IV) were significantly associated with prevalence of tuberculosis infection.
Conclusion:
The prevalence of tuberculosis in our study site was high. There is a need for regular screening of people living with HIV/AIDS for TB using highly sensitive method like Xpert MTB/RIF assay to know their TB status as well as early commencement of anti-TB.
Introduction
Globally, an estimated 9.9 million people fell ill with tuberculosis (TB), 1.3 million deaths among human immunodeficiency virus (HIV)-negative people and 214,000 deaths among HIV-positive people in 2020. 1 The problem of TB is worsened by HIV/AIDS, as people with HIV have a higher risk of developing active TB. About 45% of HIV-negative people with TB and nearly all HIV-positive people with TB have a high risk of death, without appropriate treatment. 2
TB and HIV co-infection remain a major problem in Africa, especially in sub-Saharan Africa which carries a high burden of both diseases. 3 The risk of HIV infection can accelerate the progression of TB within a short period through worsening the immune system. The rapid spread of the HIV epidemic in many countries had led to an equally dramatic increase in the estimated number of new cases of TB. 4 According to 2020 Global TB Report, Ethiopia is among the 30 high TB and TB/HIV burden countries, with annual estimated TB incidence of 140/100,000 populations and death rate of 19 per 100,000 populations. 5
Study in prevalence and risk factors of active TB among adult HIV patients in Northwestern Tanzania showed gender, baseline CD4, World Health Organization (WHO) stage were associated with developing TB. 6 Another study in South Ethiopia, Arba Minch showed smoking, previous TB therapy, and CD4 count were independently associated with TB detection. 7
The dual TB/HIV burden forms a lethal combination, each speeding the other’s progress. The national responses to the TB and HIV epidemics in Ethiopia that started in 2004 had effect on to decline TB/HIV co-infection rate over several years in Ethiopia ranging from 17% in 2011 to 6% in 2020 saving the lives of hundreds of thousands of affected citizens. Despite this, TB remains to be the leading cause of death of people with HIV, accounting for around 40% of AIDS-related deaths. 8
Ethiopia has adopted the post-2015 TB strategy called the end TB strategy which aims to end the TB epidemic by 2035 by reducing TB incidence by 90% and mortality by 95% from the 2015 baselines, and percent of affected households facing catastrophic costs due to TB to zero. Furthermore, the country has also committed to attain the targets set for the political declaration of the United Nations General Assembly High-Level Meeting on TB (TB-UNHLM), in 2018, which reaffirms the global commitment to end the TB epidemic by 2030. 8
To evaluate this aspiring plan, current and up-to-date information related to the occurrence of TB is vital. Therefore, this study explored prevalence of pulmonary TB and associated factors among adults living with HIV attending public hospitals in Shashamene Town, Oromia Region, South Ethiopia. The results obtained from this study will contribute to evidence for policy makers and program planners working at various levels of TB control programs, as well as informing healthcare professionals in the areas of TB control and prevention.
Methods
Study design and study period
Institutional-based cross-sectional study design was conducted from November 2020 to February 2021.
Study area
This study was conducted in Shashamene Town Public Hospitals, Oromia Region, South Ethiopia. The town is located 250 km south of Addis Ababa, the capital city of Ethiopia. The town has one referral hospital and one general hospital which serve a total of 4582 patients currently on ART. Xpert MTB/RIF assay was used to diagnose TB in HIV-positive cases in ART clinics of the hospitals.
Study population
All HIV/AIDS patients who were visiting the clinics during the data collection period and fulfill the eligibility criteria were the study population.
Eligibility criteria
Adult people living with HIV/AIDS whose age was greater than or equal to 18 and willing to participate in the study were included. Patients on anti-TB treatment and unable to give sputum samples were excluded.
Sample size and sampling technique
The sample size (n) was calculated using the formula for single population proportions

Considering the following assumption: Zα/2 = significance level at α = 0.05, P = previous prevalence of TB and HIV co-infection 17.4%,
9
d = margin of error of 0.05, accordingly, the total sample size was calculated as
The total sample size of 242 adults living with HIV/AIDS patients on the anti-retroviral drug during the study period was selected using systematic random sampling from 2890 adults living with HIV/AIDS attendances (Shashamene Referral Hospital = 2241 and Melka Oda General Hospital = 649) during 4 months data collection period. The 242 sample size was distributed to the two hospitals proportionally.
Data collection
A pre-tested structured questionnaire adapted from previous studies conducted in Ethiopia7,9 was used to collect socio-demographic, history of cigarette smoking and alcohol drinking, and clinical characteristics. The questionnaire was prepared in English and translated into Afaan Oromo then back to English and compared for consistency. Data were collected from participants by nurse through face-to-face interviews after obtaining consent.
After collection of blood sample either from a fingerprick or vein puncture for CD4 count, each participant was instructed to bring a sputum sample in a clean, sterile, and screw-cupped container. A sputum sample of 2–5 mL was collected at spot from each participant aseptically giving a total of 230 specimens from HIV-positive participants and submitted to the laboratory immediately for diagnosis. In case of delay, sputum specimens were kept at 2°C–8°C.
The sputum samples were examined using Xpert MTB/RIF analyzer (Cepheid, Sunnyvale, CA, USA). Briefly, 1 mL of sputum sample was mixed with 2 mL sample reagent to deactivate the bacilli and digesting debris and incubated at room temperature for 10 min; then, 2 mL of the mixture was transferred to cartridge and then loaded in the GeneXpert (Cepheid) machine. The result was obtained with less than 2 h of processing. 10
CD4 cells were counted by BD FACSPresto analyzer (Becton Dickinson, San Jose, CA, USA). Briefly, a drop of blood from a fingerprick or vein puncture was added to the cartridge and incubated in the workstation for 18 min. The cartridge was inserted into the cartridge door for analysis. The results were displayed on the screen and printed automatically. 11
Quality assurance
Data quality was ensured using standardized data-gathering tools, pretesting of the questionnaires on 5% of participants, appropriate training for data collectors, and running a built-in quality control system. All laboratory procedures were carried out according to standard operating procedures (SOPs).
Statistical analysis
Data were entered into and cleaned using EpiData Version 3.1 and then exported to SPSS version 25 for further analysis. Bivariate logistic regression was used to determine predictors of TB among HIV-positive patients. Variables with value ⩽0.25 in the bivariate analysis were entered into multiple logistic regressions to identify variables independently associated with TB in HIV-positive patients. Associations between dependent and independent variables were assessed and its strength was described using odds ratios at 95% confidence intervals (CIs). A p value of <0.05 is considered as a statistically significant association.
Results
Socio-demographic characteristics
Of 242, a total of 230 study participants were interviewed with a response rate of 95%. In this study, the mean age of study participants was 36.75 (±14.84) years. The majority of study participants, 149 (64.8%), were 18–35 years old, 118 (51.3 %) were females, 116 (50.4%) were married, 146 (63.5%) were urban dwellers, and 35(15.2%) had no formal education (Table 1).
Socio-demographic characteristics of PLHIV attending anti-retroviral therapy clinic at Shashamene public hospitals, Shashamene Town, 2021 (n = 230).

Clinical characteristics and health behavior
More than half of the study participants had cough 143 (62.2%), fever 170 (73.9%), night sweating 156 (67.8%), and normal body mass index 165 (71.7%). Regarding drug adherence behaviors, most of them had good drug adherence 182 (79%) and 203 (90%) used isoniazid preventive therapy. Concerning their immune status, 134 (58.3%) had CD4 counts ⩾350 cells/mm3 and 145 (63.0%) participants were in stage I and II of WHO clinical staging. Participants with the habit of cigarette smoking 21 (9.1%) and alcohol drinking 34 (14.8%) were reported (Table 2).
Clinical characteristics and Health behavior among PLHIV attending anti-retroviral therapy clinic at Shashamene public hospitals, Shashamene Town, 2021 (n = 230).

Prevalence and associated factors of pulmonary TB among PLHIV
A total of 230 HIV/AIDS-positive subjects were included in this study. Of these, 54 (23.5%, 95% CI: 18.26, 29.13) were positive for MTB and rifampicin-resistant MTB was not detected. In this study, age range of 50–64 years (adjusted odds ratio (AOR) = 0.05, 95% CI: 0.01, 0.34, p = 0.002), female (AOR = 0.10, 95% CI: 0.04 0.29, p = 0.002), occupation with house wife (AOR = 26.05, 95% CI: 4.4, 154.6, p = 0.001), and WHO stage (III and IV) (AOR = 3.39, 95% CI: 1.50, 7.68, p = 0.003) were significantly associated with prevalence of TB, whereas other factors such as residence, educational level, marital status, monthly income, ART enrollments, CD4 status, TB-preventive therapy, previously treated with anti-TB drugs, cigarette smoking, alcohol consumption, and a habit of opening window at daytime were not statistically associated with prevalence of TB (Table 3).
Prevalence and associated factors of pulmonary tuberculosis among adults with HIV/AIDS attending ART clinic at public hospitals, Shashamene Town, 2021 (n = 230).
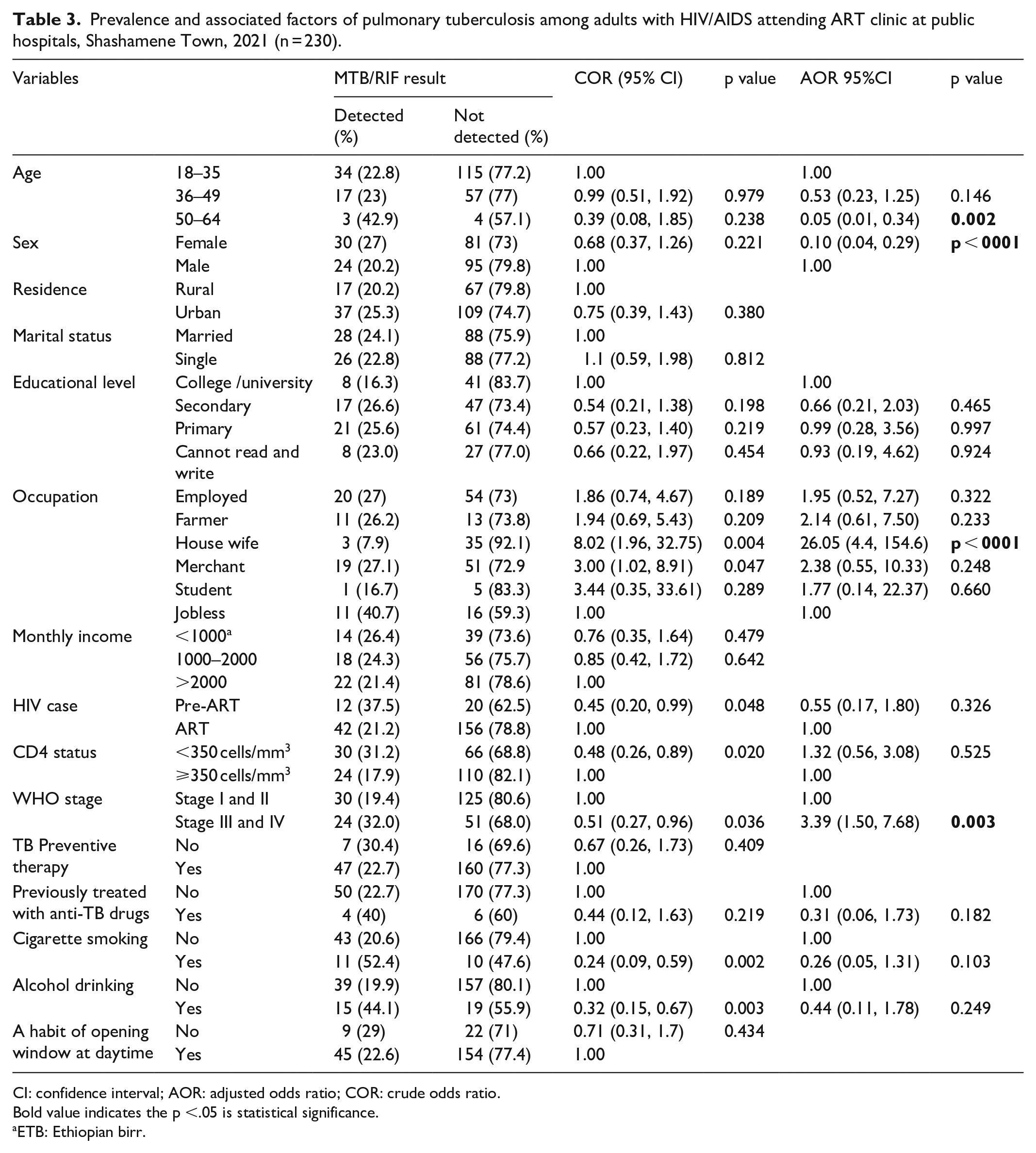
CI: confidence interval; AOR: adjusted odds ratio; COR: crude odds ratio.
Bold value indicates the p <.05 is statistical significance.
ETB: Ethiopian birr.
Discussion
Our study revealed that the overall prevalence of pulmonary TB among people living with HIV/AIDS was 23.5 % (95% CI: 18.26, 29.13). The finding of this result is comparable to the study done in Afar, Ethiopia (26.4%); 12 Amhara, Ethiopia (27.7%); 13 and Shashamene, Ethiopia (24.9%). 14 Similarly, it is consistent with the study done in Abuja, Nigeria (24.5%) 15 and Tirana, Albania (27.4%). 16 It is also comparable to the pooled prevalence of pulmonary TB reported in Ethiopia which was 25.6%. 17
Our study showed that the prevalence is higher than the study done in Wolaita Sodo, Ethiopia (17.4%); 9 in Arba Minch, Ethiopia (7.2%); 18 and Debre Birhan, Ethiopia (5%). 19 The prevalence is also higher with the study done in Lagos, Nigeria (21.6%); 20 Cape Town, South Africa (17.3%); 21 Eastern Cape Province, South Africa (8.8%); 22 Mozambique (10.1%); 23 Dare Salam, Tanzania (7.9%); 24 Georgia, USA (11.5%); 25 and Mainland China (7.2%). 26 The discrepancy in the magnitude of TB among HIV-positive participants may be due to the difference in the healthcare system among ART centers, variation in study design, the diagnostic methods employed (smear microscopy, culture, GeneXpert), ART regimens, and their adherence and adverse drug-related problems.
The finding of pulmonary TB among HIV patients was lower than the study done from Harari, Eastern Ethiopia (29.8%); 27 Northern India (29.5%); 28 and Moscow, Russia (33.5%). 29 This difference might be due to sample size, study design, and diagnosis method. Besides, the variation may be attributed due to the course of infection and the presence of concomitant opportunistic infections that alter the host immunity, the socio-economic condition of study subjects, and awareness of the community to seek healthcare for both TB and HIV. 30
This study showed females were more likely to be positive for TB than males as study reported in Harari, Ethiopia. 31 Advanced WHO clinical stage (III and IV) was also found to be positively associated with TB among HIV-positive adults in our study. This finding is comparable with the study done in Debre Tabor, Ethiopia and Tanzania which showed that advanced WHO clinical disease staging becomes more risk for developing and recurrence of OIs (Opportunistic infections) including TB,6,32 and this study showed marital status, alcohol consumption, and ART enrollments and TB-preventive therapy were not associated with TB infection like that of the study reported in Wolaita Sodo Teaching and Referral Hospital. 9 In contrast to this study, Arba Minch, Ethiopia study indicated that taking TB-preventive therapy was an independent predictor of TB among HIV-positive adults on ART. 7 Patients who had not taken TB-preventive therapy were more likely to develop TB as compared to those who took IPT (Isoniazid Preventive Therapy). 33 A report from Harari, Ethiopia 27 and from South Tongu district, Ghana showed not taking IPT were significant predictors of TB. 34 A report from Nigeria following the regimen correctly can minimize the infection even though not associated. 3
Our study finding showed that CD4 cell count is not significantly associated with pulmonary TB infection. This is comparable with findings which 3 indicated that not associated for development of TB in HIV/AIDS patients but maintaining the CD4 cell level as high as possible in patients with the advanced disease helps the person to have low risk of infection or reactivation of tubercle bacilli. Reactivation or re-infection might also be a possible explanation for the existing deregulated immunity.6,7,35
Limitation of the study
This study was a facility-based study; it does not capture HIV-positive individuals who were not visiting health facilities. The participants may not remember all information asked during data collection; therefore, the data are not completely free of recall bias.
Conclusion
The prevalence of pulmonary TB among people living with HIV/AIDS attending public hospitals in Shashamene Town was 23.5%. In this study, age range of 50–64 years, female gender, occupation with house wife, and WHO stage (III and IV) were significantly associated with prevalence of TB infection.
Therefore, TB case finding and early initiation of ART are necessary to minimize the burden of disease among patients with HIV. In addition, studies on the trends in TB/HIV co-infection and associated factors should also be implemented in large scale across the country.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221122437 – Supplemental material for Prevalence of pulmonary tuberculosis and associated factors among adults living with HIV/AIDS attending public hospitals in Shashamene Town, Oromia Region, South Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221122437 for Prevalence of pulmonary tuberculosis and associated factors among adults living with HIV/AIDS attending public hospitals in Shashamene Town, Oromia Region, South Ethiopia by Belayneh Tadesse Gisso, Mesfin Worku Hordofa and Moges Desta Ormago in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank laboratory staff and ART clinic staff who were working at Shashamene Referral Hospital and Melka Oda General Hospital for their support during data collection. We also acknowledge all study participants for their willingness to take part in the study.
Author contributions
B.T.G., M.D.O. and M.W.H. designed the experiment, carried out laboratory work and participated in data analysis. M.D.O. wrote the manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data availability
All relevant data are available within the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from Hawassa University College of Medicine and Health Science Institution Review Board (IRB) with ref. no. IRB/227/12. A permission and support letter was obtained from Oromia Regional Health Bureau to conduct the study in the hospitals. Informed written consent was obtained from each participant and also informed about the rights to terminate participating in the research at any time of the study. Confidentiality of information was maintained by codes and putting in a lockable cabinet. Clinicians were communicated the findings for management of patients.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.