
Abstract
A pressure ulcer is a localized skin injury and underlying tissue, usually as a result of friction or pressure against the surface of the skin. The global mortality rate of pressure ulcers was above 60% for hospitalized patients who wait 1 year of hospital stay. Nurses are the primary responsible body and forefront line care providers for the prevention of pressure ulcers, so nurses’ knowledge and practices are the major rollers to handling this preventable problem.
Objective:
To assess pressure ulcer prevention knowledge, practices, and their associated factors among nurses in Gurage Zone Hospitals, South Ethiopia, 2021.
Methods:
A cross-sectional study was conducted in Gurage Zone hospitals from May to June 2021. Data were collected using a structured self-administered paper questionnaire from 372 participants using a simple random sampling procedure, and the collected data were checked for their completeness and entered into Epi-data version 4.6 and exported to SPSS version 26 for analysis.
Results:
In this study, 176 (49%) of nurses have good knowledge and 210 (58.5 %) of nurses have good practices. Variables having masters and above (adjusted odds ratio = 2.075; confidence interval: 1.886, 4.861), using guideline (adjusted odds ratio = 1.617; confidence interval: 1.017, 2.572), and cooperativeness of patients (1.859; confidence interval: 1.066, 3.242) was significantly associated with nurses prevention knowledge. Being divorced (adjusted odds ratio = 3.002; confidence interval: 1.023, 4.219), degree nurse (adjusted odds ratio = 2.639; confidence interval: 1.388, 3.051), workload (adjusted odds ratio = 0.480; confidence interval: 0.245–0.939), unproportioned nurse to patient ratio (adjusted odds ratio = 0.480; confidence interval: 0.158–0.747), patient cooperativeness (adjusted odds ratio = 1.859; confidence interval: 1.066–3.242), and nurses having good knowledge (adjusted odds ratio = 1.684; confidence interval: 1.078–2.632) statistically significant with prevention practices.
Conclusion:
The overall level of pressure ulcer prevention knowledge and practice of nurses were good. Qualification of nurses’ degree and above, use of pressure ulcer prevention guidelines, over workload, unproportionate nurse-to-patient ratio, and patient cooperativeness were statistically significant factors for pressure ulcer prevention knowledge and practices. Therefore, health managers should provide continuous professional development, and ensure proportionated nurse-to-patient ratio allocation policy.
Introduction
A pressure ulcer is a localized skin injury and underlying tissue usually over a bony prominence or pressure in combination with friction, and patients with a medical condition that limits changing positions and confines to a bed for a long time are most at risk for pressure ulcers. 1 Pressure ulcer risk patients should be identified and put on a management plan to prevent its development, improve healing, and prevent complications of existing pressure ulcers. 2 So aggressive, ongoing prevention programs like skin assessment, care, frequent repositioning, and use of supportive surfaces to reduce the incidence, time is taken for treatment. 3
The global morbidity and mortality rates of pressure ulcers were above 60% for older patients within 1 year of hospital stay. 4 The Coloplast pressure ulcer summit report indicated that about 60,000 people died because of the pressure ulcer complication worldwide. 5 Reports showed that around 700,000 patients were affected by pressure ulcers each year and around 186,617 patients develop a new pressure ulcer in acute care settings each year, and it accounts for 2% of preventable death. 6
A patient with a pressure ulcer has a mortality risk of 2 to 6 times greater than a patient with intact skin; despite its devastating effects, 95% of pressure ulcers can be preventable.7,8 Nowadays if a patient developed a pressure ulcer, then it indicates poor quality of health care service and has the effect of poor quality of life on the patient. 9 Although the responsibility of pressure ulcer prevention is given to all health care professionals, mainly nurses are the forefronts care providers, and the prevention of pressure ulcers requires the knowledge and skills of nurses working in the hospitals. 10
A pressure ulcer is one of the most costly and physically debilitating complications since the 20th century. 11 The pain and discomfort of pressure ulcers delay rehabilitation, prolong illness and timing of discharge, and contribute to compromising the physical, social, financial, and psychological quality of life. 12 It has been identified that nurses have poor knowledge of the prevention of pressure ulcers and reflected poor practices, and they do not comply with the use of guidelines. 13 Pieces of evidence revealed that inadequate pressure ulcer-related knowledge and skills contribute suggestively to the occurrence or worsening of pressure ulcers. 14 Studies conducted in South Africa showed that only 42.7%–49% of nurses have good knowledge and good pressure ulcer prevention practices and elsewhere in Ethiopia only 50.8% of nurses have good pressure ulcer prevention practices.15,16 The study also revealed that the contributing factors for pressure ulcer prevention knowledge and practices were heavy workload, inadequate staff, inadequate training, lack of supportive devices, and qualification of nurses. 17 While factors or barriers, educational competency, over workload, use of the guideline, and unproportionate nurse-to-patient ratio were not statistically significant for the knowledge and practice of nurses. 17 Therefore, identifying these hindering factors and enhancing the prevention level of knowledge and practices are the cornerstone of effective prevention of pressure ulcers. 18
A pressure ulcer is one of the most costly and physically debilitating problems, which is highly prevalent in Ethiopia; it is directly related to nurses’ knowledge and practices toward prevention aspect, but no study had presented this. The different situations or characteristics of nurses added in this study were over the workload of nurses, unproportioned nurse-to-patient ratio, and using pressure ulcer prevention treatment guidelines, but these predictors were not found on previous studies.
In my best search, there is not enough evidence on pressure ulcer prevention knowledge, practices, and their associated factor among nurses in Ethiopia, especially in this study setting. Some study results done elsewhere were away from this, and miss some important variables, and some variables were also not significantly associated with the dependent variable. So, this study would be essential to fill these gaps, and the finding of this result would use as evidence-based practices for health care providers and development of pressure ulcer prevention standards, policies, and guidelines. Therefore, this study aimed to assess pressure ulcer prevention knowledge, practice, and their associated factors among nurses working in Gurage Zone hospital South Ethiopia and to answer the research questions:
Research Question 1. what are the levels of nurses’ pressure ulcer prevention knowledge and practices? and
Research Question 2. what are the factors associated with pressure ulcer prevention knowledge and practices of nurses?
Methods and materials
Study setting and period
The study was conducted in Gurage Zone hospitals. The Gurage Zone has eight hospitals and the study setting was at Attat hospital, Butajira hospital, Wolkite university hospital, and Bue hospital. Attat primary hospital is located 187 km southwest of Addis Ababa, the capital city of Ethiopia. It had 44 nurses and 14 midwives. Butajira generalized hospital is found in the Butajira town of the Gurage zone, located 143 km from Addis Ababa. The hospital had 83 nurses and 17 midwives. Wolkite university hospital is found in Wolkite Town, which is located 158 km away from Addis Ababa. The hospital had 119 nurses and 22 midwives. Bue hospital is found in Bue woreda, which is located 168 km from Addis Ababa. The hospital had 47 nurses and 9 midwives. The study was conducted from May to June.
Study Design: Institutional-based cross-sectional study design was used.
Source of population: All Nurses working in Gurage Zone hospitals.
Study population: All Nurses working in the selected Gurage Zone hospitals fulfilling the inclusion criteria.
Inclusion and exclusion criteria
Inclusion criteria included all nurses working in Gurage Zone hospitals.
Exclusion criteria included nurses who were being on annual, maternal, sick leave during data collection time.
Sample size calculation and sampling procedure
Sample size determination
The sample size was determined by using a single population proportion formula for the first objective and associated variables of the second objective and the largest sample size was determined by considering the following assumptions; pressure ulcer prevention practice (P) is 67.3% at a study conducted in Addis Ababa, Ethiopia, 16 95% confidence interval (CI) and margin of error (d) = 5%.


Sampling procedure
There are eight hospitals in Gurage Zone and from those four (Wolkite University, Butajira, Attat, and Bue) hospitals were selected using simple random sampling, lottery method. A total of 385 nurses working in four selected hospitals were selected: 115 nurses from a total of 119 nurses working in Wolkite university specialized hospital; 78 nurses from 81 working in Attat hospital; 134 from a total of 138 working in Butajira hospital; and 45 nurses from 47 working in Bue Hospital were selected, with a final number of 372 study subjects; nurses were selected proportionally using simple random sampling method from each hospital.
Data collection tool and procedure
A structured self-administrated standardized questionnaire was used to collect the data. Three graduating class nursing students as data collectors through direct visiting of the participants and three BSc nursing clinical practitioners as supervisors were used during data collection. The questionnaire tool has five sections: sociodemographic part (sex, age, ethnicity, religion, marital status, educational status, monthly salary, work experience), clinical-related (working unit, receiving training on pressure ulcers, use of guidelines, workload, shortage of staff, staff cooperativeness, and patient cooperativeness) and nurses attitude-related questionnaire which has 10 questions with a scale of 5 for “strongly agree,” 4 for “Agree,” 3 for “neither agree nor disagree,” 2 for “disagree,” and 1 for “strongly disagree and was determined by nurses who scored greater or equal to the mean of attitude-related questions as having a good attitude, while below the mean having a poor attitude. Pressure Ulcer Prevention Knowledge and Practices Assessment Instrument was used for dependent variables. 19 The instrument consists of 18 knowledge and 18 practices-based questions and each knowledge question has three responses with a scale of 0 to 2 (0 = I don’t know, 1 = False, and 2 = True) response and each practices question has three responses with a scale of 0 to 2 (0 = Never, 1 = Sometimes, and 2 = Always) response, and was determined by participants who scored greater or equal to the mean of knowledge and practices-based questions as having a good level of knowledge and practices; while below the mean having poor knowledge and practices; which adapted from the study conducted in Gondar university hospital and public hospitals in Wollega Zone, Ethiopia with the internal consistency reliability (Cronbach’s α) correlation coefficient of 0.88.20,21 A structured questionnaire was prepared in the English language and pretested 1 week before starting data collection. The training was given to data collectors and supervisors regarding each description of the tool and the way they collect the data. For the appropriateness of data collection, four fourth nursing students and two nurses for supervision were used.
Data quality assurance
To maintain data quality, the pretested tool was used. One week before undertaking the actual data collection, the instrument was tested by taking 5% of the sample size to check the validity and reliability of the tool, and modification was done accordingly. Even, training was given to data collectors for 1 week before the data collection on the objective of the study and how to collect data for this study purpose using the data collection tool. Each component of the tool was discussed clearly for data collectors. Up to this, the data collection process was monitored closely by the supervisor throughout the data collection period. Finally, data was cleaned, coded, and entered into a computer. During data entry, a consistency check was made, and an entry error was manually checked by going back to the questionnaires.
Statistical analysis
After the data were checked for their consistency and completeness, data were entered into Epi data Version 4.2 and transported to SPSS version 26 for further analysis. Tables, graphs, and narration presented the descriptive findings of this study. Binary logistic regression using bivariate analysis and multivariate analysis with a 95% CI was used to estimate the association between the independent variables and the outcome variable. Independent variables with a p-value ⩽ 0.2 were included in the multivariate analysis to control confounding factors. Adjusted odds ratio along with 95% CI was used to estimate to associate factors of pressure ulcer prevention knowledge and practices. Finally, the variables that have a p-value
Ethical consideration
Ethical approval was obtained from Wolkite University, College of Medicine and Health Science, Institutional Review Board (IRB) with ethical approval number RCSUILC/08/2021. We have obtained verbal informed consent from each study participant, but since it is not a clinical trial, it was not mandatory to obtain written informed consent, and this consent was approved by the Institutional Review Board.
Result dissemination plan
After this research was conducted, the result was submitted to the College of Medicine and Health Sciences research coordinator and Wolkite University research directorate and library. Then, the study findings were disseminated to selected hospitals. The research article was presented in health professional organizations, annual meetings, professional conferences, and training. Finally, it was published in national and international peer-review journals to disseminate the result worldwide.
Results
Sociodemographic characteristics
In this study, 372 study participants were involved, with a response rate of 96.5%. Of the total number of respondents, more than half 205 (57.1%) were females. Moreover, the age of the participants ranged from 20 to 43 years, with a mean age of 29.7 ± 4.6 years. Of the respondents, 175 (48.7%) were Muslim and 234 (65.2%) were married. The majority 194 (54%) of nurses were bachelor degree holders in nursing with a mean work experience of 5.6 ± 4.9 years. patients minimally inquire 3500 ETB and maximally inquire 16700 ETB per month with a mean monthly income of the nurses was 7271.2 ± 3270.2 ETB (Table 1).
Sociodemographic characteristics of nurses in Gurage Zone hospitals, Ethiopia, 2021 (n = 372).

Clinical factors
The majority of the nurses had not received training, 233 (62.1%) and 191 (53.2%) of them were not using the existing guidelines about pressure ulcer prevention practices. Above 308 (85.8%) nurses complain over workload and 283 (78.8%) of nurses had unproportionate nurses-to-patient ratio in the ward, and 285 (79.4%) and 282 (78.6%) of staff and patients were cooperative with the health care service, respectively (Table 2).
Clinical factors of nurses on pressure ulcer prevention in Gurage Zone hospitals, Ethiopia 2021 (n = 372).

Pressure ulcer prevention knowledge
Of the respondents, 176 (49%) had good knowledge, while 183 (51%) of the respondents had a poor knowledge with the mean value of 42.38 ± 2.843 for the prevention of pressure ulcers (Figure 1).

Pressure ulcer prevention knowledge among nurses working in Gurage Zone hospitals, South Ethiopia, 2021 (n = 372).
Pressure ulcer prevention practices
Of the total respondents, 210 (58.5 %) of them had good pressure ulcer prevention practice; whereas the remaining 149 (41.5%) of the respondents had poor practice with a mean value of 39.94 ± 2.910 (Figure 2).

Pressure ulcer prevention practices among nurses working in Gurage Zone hospitals, South Ethiopia, 2021 (n = 372).
Factors associated with pressure ulcer prevention of knowledge and practices
Marital status, professional qualification of nurses, income, over workload, unproportioned nurse-to-patient ratio, staff cooperativeness, patient cooperativeness, and knowledge were associated with pressure ulcer prevention practices of nurses working in the hospital.
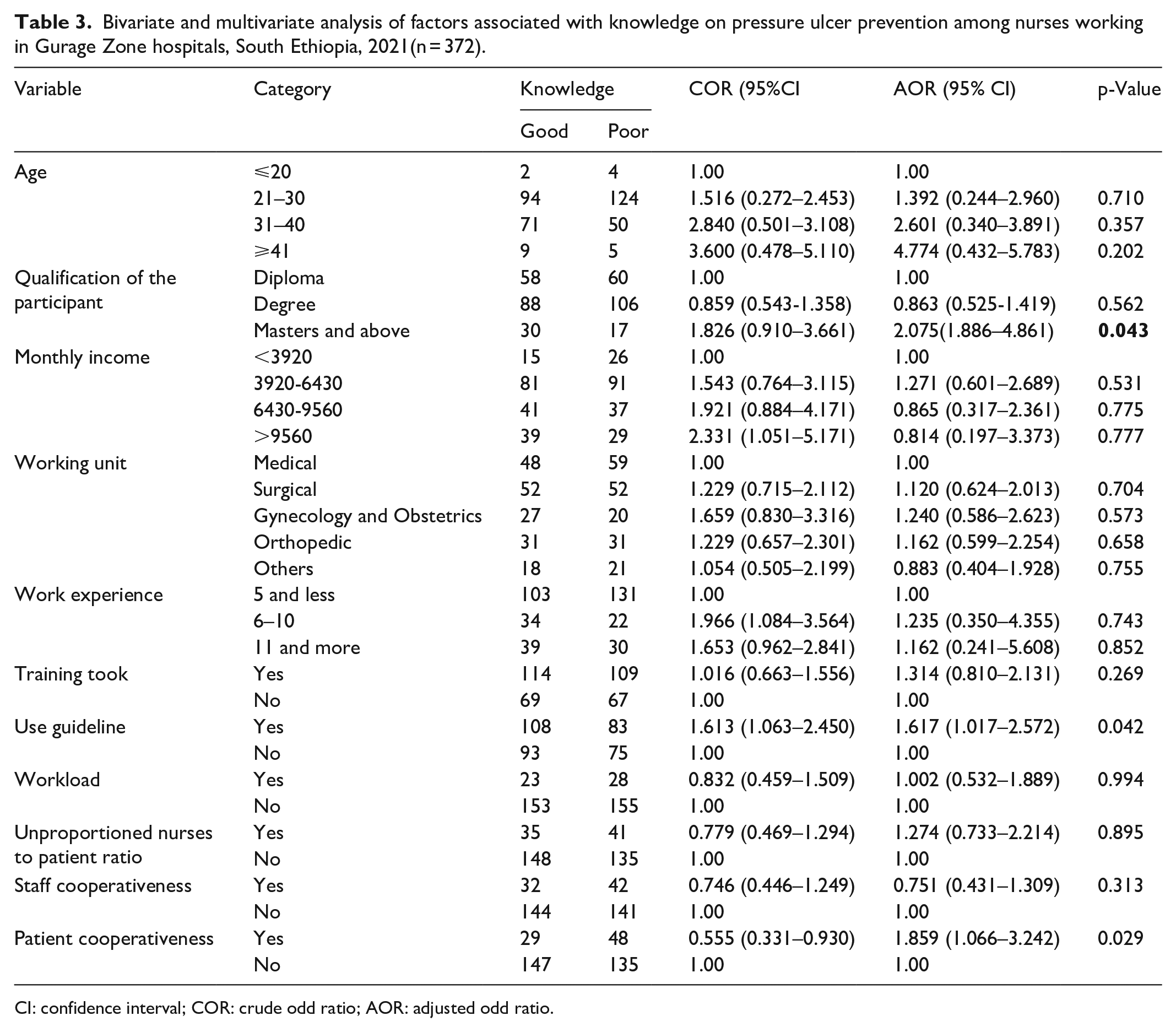
Variables having professional qualification of master’s and above, use of pressure ulcer guidelines and patient cooperativeness were statistically associated with nurses’ knowledge. Nurses having qualifications of master’s and above are two times more likely to have pressure ulcer prevention knowledge than diploma nurses (adjusted odds ratio (AOR) = 2.075; CI 1.886, 4.861). Nurses using pressure ulcer prevention guidelines were 1.6 times having the knowledge about pressure ulcer prevention than nurses who did not use the guideline (AOR = 1.617; CI: 1.017, 2.572). Being cooperative patients were almost two times more statistically associated with knowledge of pressure ulcer prevention than non-cooperative patients during their health care delivery (1.859; CI: 1.066, 3.242) (Table 3).
Bivariate and multivariate analysis of factors associated with knowledge on pressure ulcer prevention among nurses working in Gurage Zone hospitals, South Ethiopia, 2021(n = 372).
CI: confidence interval; COR: crude odd ratio; AOR: adjusted odd ratio.
Marital status of being divorced, having qualification of nursing degree, over workload, unproportioned nurse-to-patient ratio, and nurse’s knowledge were statistically significant with pressure ulcer prevention practices. The marital status of nurses being divorced was relatively three times of those having patient pressure ulcer prevention practices than being widowed (AOR = 3.002; CI: 1.023, 4.219). Degree nurse professionals were almost 2.6 times having pressure ulcer prevention practices than diploma nurse professionals (AOR = 2.639; CI 1.388, 3.051).
Nurses having over workload decreased their pressure ulcer prevention practices by two times than nurses who have no workload in the working area (AOR = 0.480 CI; (0.245–0.939)). An unproportioned nurse-to-patient ratio was two times less likely to have pressure ulcer prevention practices than having a proportioned nurse-to-patient ratio in the health care delivery system (AOR = 0.480; CI: 0.158–0.747). Patient cooperativeness was more than 1.9 times increasing nursing pressure ulcer prevention practices than non-cooperative patients (AOR = 1.859; CI: 1.066–3.242). Nurses having good knowledge of pressure ulcer prevention were 1.7 times more likely to have good pressure ulcer prevention practices than nurses who have a poor level of knowledge (AOR = 1.684; CI: 1.078–2.632) (Table 4).
Bivariate and multivariate analysis of factors associated with pressure ulcer prevention practices among nurses working in Gurage Zone hospitals, South Ethiopia, 2021(n = 372).

CI: confidence interval; COR: crude odd ratio; AOR: adjusted odd ratio.
Discussions
Pressure ulcer prevention knowledge and practices of nurses working in the hospitals
According to this study finding the level of nurses’ knowledge of pressure ulcer prevention was well scored above the mean value (Figure 1). This finding was similar to the studies reported in the United Kingdom, 6 Australia, 22 Japan, 23 and Bangladesh. 24 The finding also resembles the studies from Kenya 25 and Addis Ababa. 16
The nurse’s level of knowledge in this report was good (Figure 1) when relatively compared to the study findings reported from Slovakia 26 and Lohar University hospitals. 27 South Africa, 15 Uganda, 14 Umgungundlovu District in South Africa, 28 and National Orthopedic Hospital of Enugu in Nigeria 29 show that nurses have poor knowledge of pressure ulcer prevention. Similarly, the levels of knowledge were poor in the studies conducted in Federally Administered Hospitals in Addis Ababa, 30 Gondar University Hospital, 20 Hawassa University comprehensive specialized hospital, 31 and public hospitals in Wollega 21 relative to this study finding (Figure 1). The difference might be due to a change of methodology and also might be due to increased knowledge source of information, scientific evidence, and research results, along with increased educational level of health care workers (qualification) that might also be the cause of the difference.
According to this study, the levels of pressure ulcer prevention practices have been good, scored above the mean level (Figure 2). This finding was consistent with the study conducted in German, 32 Saudi Arabia, 10 and Bangladesh. 33 Also, the study finding was similar to studies in South Africa, 15 Gondar University, 20 Harari regional state and Dire Dawa, 33 and Public hospitals in Addis Ababa, 16 Federally Administered Hospitals in Addis Ababa. 30
While studies conducted in Sweden, 10 Japan, 23 Lohar university hospital, 27 University of Maiduguri Teaching Hospital in Nigeria, 34 Uganda, 14 Umgungundlovu District in South Africa, 28 Enugu in Nigeria, 29 and Gondar University Hospital 20 had poor pressure ulcer prevention practices relative to this study finding (Figure 2), which was good pressure ulcer prevention practices. The reason might be due to nurses having a good level of knowledge and increasing scientific evidence, using guidelines on pressure ulcer prevention source of knowledge, and increasing the overall health care delivery system for hospitalized patients which might be the difference.
Factors associated with pressure ulcer prevention knowledge and practices of nurses
In this study, nurses qualifying master’s degree and above were an important factor; it was statistically associated with pressure ulcer prevention knowledge of nurses with more than two times having good knowledge on pressure ulcer prevention than nurses qualifying diploma (Table 3). This finding was consistent with the studies conducted in Australia, 22 Finland, 35 Slovakia, 26 and the University of Lahore. 27 The finding also resembles studies conducted in Saudi Arabia, 10 Umgungundlovu District in South Africa, 28 and Gondar University Hospital. 20 The reason that nurses having a master’s degree and above are more likely to have good pressure ulcer prevention knowledge might be due to their advanced education level and better academicals level, and long years of experience may cause acquiring and retaining more knowledge.
Using pressure ulcer prevention guidelines was significantly associated with pressure ulcer prevention knowledge of nurses, which was 1.6 times having a good knowledge level than nurses who were not using pressure ulcer prevention guidelines (Table 3). This result was similar to the studies reported from Australia, 22 German, 32 South Africa, 15 Embu in Kenya, 25 and Addis Ababa. 16 The result is also similar to reports in Federal Hospitals in Addis Ababa 30 and Wollega, Ethiopia. 21 The reason might be due to the use of guidelines used as a direct source of information and hold sets of systematic procedures that were expected from nurses for pressure ulcer prevention and having good knowledge.
Patient cooperativeness was statistically associated with pressure ulcer prevention knowledge of nurses, with almost two times more positively associated with nurses’ knowledge level than those patients who were not cooperative (Table 3). There were no similar researches that displayed this finding. The difference might be due to respecting and compassionating with health caregivers may patronage the care providers to know more about their patients.
This study found that nurses being divorced were significantly associated with pressure ulcer prevention practices, with more than three times more positively associated with prevention practices than being widowed (Table 4). There were no similar studies with this finding. Being divorced is more associated with the practices of nurses than nurses being widowed, this difference might be due to social challenges faced within their daily activities, which may interfere with or hinder widowed nurse practitioners in clinical practices in the working area.
Degree nurses were positively associated with pressure ulcer prevention practices with 2.6 times more likely to have good pressure ulcer prevention practices than diploma nurse workers did (Table 4). This study was in line with the reports revealed from Borno state in Nigeria, 34 Kenya, 36 Harari regional state, and Dire Dawa City administration. 33 This might be due to the amount of knowledge conceived through their learning time, prolonged time of clinical attachments, and clinical experience may cause the difference.
Over workload was negatively associated with pressure ulcer prevention practices with two times less likely to have pressure ulcer prevention practices than nurses who were not work overloaded (Table 4), which is the same as studies in Enugu in Nigeria 29 and Kenya. 36 The reason might be due to nurses’ lack of time, tiresome, spadework to do pressure ulcer prevention practices.
Unproportioned nurse-to-patient ratios has been more than two times more negatively associated with pressure ulcer prevention practices than a proportionated nurse-to-patient ratio in the hospital (Table 4). The finding was similar to the studies reported from Enugu in Nigeria, 29 Kenya, 25 Ugandan, 14 and Gondar University Hospital. 20 The reason is a small number of nurses in the hospital may cause an overwork load on nurses, too busy, lack of time to provide, and even missing the nursing care service to all patients.
Patient cooperativeness was positively associated with pressure ulcer prevention practices, with 1.9 times more likely to have good prevention practices than non-cooperative patients (Table 4). This result resembles the researchers reported from Nairobi in Kenya 36 and Embu in Kenya. 25 The variation might be due to patients’ keeping respect and compassion to care providers and better achievement of patient-centered health care service and the overall health care practices to patients.
Having good pressure ulcer prevention knowledge was more than 1.7 times more likely to have prevention practices than nurses who have poor knowledge (Table 4). This output was mimicked with the studies conducted in Bangladesh, 33 South Africa, 15 Borno State in Nigeria, 34 and Kenya. 36 The result is also similar to the reports displayed in Umgungundlovu District in South Africa, 28 Addis Ababa, 16 Federal Hospitals in Addis Ababa, 30 Harari regional state, and Dire Dawa city administration hospital. 33 Knowledge is the lowest level of learning outcome that would produce the highest level of learning outcome is practices or skill might be the possible reason.
Strength
Standardized and valid questionnaires were used in this study.
Many variables were assessed, and new variables were also added to assess
Limitation
The study did not address the qualitative section using observational checklists.
The study was a cross-sectional study and did not show a cause–effect relationship
Conclusion
The overall level of nurses’ knowledge and practice was good. Variables such as qualification of master’s degree and above, use of the guideline, patient cooperativeness were significant factors for the knowledge of nurses, and being divorced, degree nurses, patient cooperativeness, over workload, unproportionate nurse-to-patient ratio and a good level of knowledge were statistically significant factors for pressure ulcer prevention practices. Therefore, the health managers should give capacity building through continuous professional development, and develop and distribute updated guidelines to the hospitals, which would enhance the pressure ulcer prevention knowledge and practices of nurses. Also, they should keep a proportionate nurse-to-patient ratio allocation policy and recruit nurses to reduce over workload, which enhances the health care practices system in the hospitals. Even nurses are expected to develop their knowledge on pressure ulcer prevention, which directly improves their practices.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221105571 – Supplemental material for Pressure ulcer prevention knowledge, practices, and their associated factors among nurses in Gurage Zone Hospitals, South Ethiopia, 2021
Supplemental material, sj-docx-1-smo-10.1177_20503121221105571 for Pressure ulcer prevention knowledge, practices, and their associated factors among nurses in Gurage Zone Hospitals, South Ethiopia, 2021 by Shegaw Tesfa Mengist, Haimanot Abebe Geletie, Bitew Tefera Zewudie, Agerie Ayinalem Mewahegn, Tamene Fetene Terefe, Baye Tsegaye Amlak, Betelhem Tadesse, Fisha Alebel GebreEyesus, Tadesse Tsehay, Mamo Solomon, Bogale Chekole Temere, Shegaw Geze Tenaw and Yibeltal Mesfin in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to say thanks to each hospital manager for allowing us to conduct this study in their respective health institution and study participants for their willingness. We also want to thank Wolkite University for allowing us to learn.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Wolkite University, College of Medicine and Health Science, Institutional Review Board (IRB) with ethical approval number RCSUILC/08/2021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
We have obtained verbal informed consent from each study participant, since it is not a clinical trial, it was not mandatory to obtain written informed consent, and this consent was approved by the Institutional Review Board.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.