
Abstract
Objectives:
The aim of this study was to search for routine blood test biomarkers in patients with physical symptoms but without a diagnosis after comprehensive routine screening diagnostic examinations.
Methods:
A total of 228 adults aged < 65 years who presented with physical complaints without known causes after comprehensive screening diagnostic examinations and 228 age- and sex-matched healthy controls without physical complaints were enrolled. The blood cell count data at the first hospital visit were compared between these groups.
Results:
Total white blood cell (p = 0.2143), red blood cell (p = 0.8954), and platelet (p = 0.7716) counts did not differ between the groups. The monocyte count (p = 0.0014) and resultant monocyte-to-lymphocyte ratio (p < 0.0001) were higher in the symptomatic group, while the other white blood cell subtypes did not differ significantly between the two groups. In the symptomatic group, patients with a monocyte-to-lymphocyte ratio > 0.25 were likely to have unexplained nonfocal physical symptoms (p < 0.0001). The characteristic findings included fatigability (p < 0.0001), prolonged slight fever (p = 0.0005), and widespread pain (p < 0.0001). The monocyte-to-lymphocyte ratio level was correlated with the proportion of patients with unexplained nonfocal symptoms.
Conclusion:
The blood cell count profile was largely the same between healthy individuals and patients with unexplained physical symptoms. However, patients with unexplained nonfocal physical complaints were likely to show an elevated monocyte-to-lymphocyte ratio, typically > 0.25.
Introduction
Patients with physical complaints without known causes often experience severely annoying physical conditions that can lead to long-term distress. Patients with these complaints and without a diagnosis after comprehensive screening diagnostic tests are often not sufficiently managed, 1 possibly due to the absence of reliable laboratory markers for the diagnosis and follow-up of patient conditions. Patients with these complaints are often given a diagnosis of exclusion, such as psychosomatic disorder, somatoform disorder, chronic fatigue syndrome, fibromyalgia, psychogenic fever, irritable bowel syndrome, autonomic nervous system dysfunction, or panic disorders.2–4 Most of these exclusion diagnoses currently lack established disease-specific diagnostic laboratory markers or specific disease mechanisms. Furthermore, some diseases with unknown causes may overlap in a single patient,5–7 complicating patient management. This study aimed to search for potential routine laboratory biomarkers for use in evaluating and managing the patients with unknown diagnoses after comprehensive screening diagnostic examinations. Thus, we evaluated blood cell counts and their derivatives in patients with unexplained physical symptoms.
Methods
Enrollment
This study was a retrospective, case-controlled observational study. The design of this study is illustrated in Figure 1. Patients with physical complaints lasting for more than 1 month and who visited the Department of General Medicine of Tohoku University Hospital between April 2018 and March 2021 were initially recruited. From these patients, those who were suffered from unexplained physical complaints lasting for more than 1 month without certain causes after subsequent comprehensive screening tests and diagnostic examinations were included in the following analyses. The exclusion criteria include (1) patients who were later given definite diagnoses based on disease-specific diagnostic objective findings (e.g. laboratory diagnostic markers or organic lesions identified with imaging tests), (2) patients with elevated serum C-reactive protein (CRP) levels ⩾ 0.30 mg/dL, and (3) patients who had been already treated by steroids or other immunosuppressants before being consulted to our hospital. Those who were with elevated CRP levels or treated by immunosuppressants were excluded to avoid potential bias in the subsequent analyses using white blood cell (WBC) count could due to possible systemic inflammation of uncertain clinical significance. 8 To compare blood test data, age- and sex-matched healthy volunteers whose blood samples were evaluated at the same university hospital, selected from 2492 healthy volunteers who fulfilled the enrollment criteria in this study, were recruited as the healthy control (HC) group. Propensity score matching was used to select matched control participants, and the age and sex were used as explanatory variables. Propensity scores were calculated using a multivariate logistic regression model. The profile of the entire population of healthy volunteers was reported previously.9,10

Flow diagram of the study design. Hemogram data were compared between 228 adult patients with unexplained physical complaints and 228 age- and sex-matched HCs. The data were further evaluated within the former group to identify associations between hemogram data and unexplained prolonged symptoms.
Evaluated data
Blood cell count data obtained at the first hospital visit, including the total WBC, red blood cell (RBC), platelet, and differential WBC counts for five WBC subtypes (neutrophils, lymphocytes, monocytes, eosinophils, and basophils), were evaluated. Using these specific and differentiated WBC counts, the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR) were determined according to the following formulas

In addition to these blood test data, detailed clinical manifestations of patients in the symptomatic group were further investigated. The most common unexplained complaints included fatigability, slight fever (37.0°C–37.9°C), widespread systemic pain, abnormal bowel habits, and cough. Based on the combinations of unexplained physical complaints, the symptomatic group was further divided into patients with unexplained single focal physical complaint, localized to one organ system, and those with nonfocal physical complaints.
Statistical analyses
Based on a priori sample size calculation, a sample of 200 participants in each group was required to detect the weak effect size of d = 0.20 with a power (1−β) of 0.80 and α = 0.05. The same to detect the moderate effect size of d = 0.50 with a power of 0.80 and α = 0.05 was 34 participants in each group. Comparisons of the quantitative variables between the two groups were performed using Student’s t-test or Mann–Whitney U test according to the distribution patterns of the variables. Comparisons of qualitative data between the two groups were performed using the chi-square or Fisher’s exact tests. Comparisons of MLR values for the common nonfocal complaints among the symptomatic patients, together with age- and sex-matched HCs, were performed using analysis of variance (ANOVA), followed by Tukey’s post hoc tests. The correlations between two quantitative variables were evaluated using Spearman’s correlation coefficient (ρ), followed by the tests of no correlation. As approximately 10 types of blood cell count and derivatives were simultaneously compared, p < 0.005 was considered statistically significant. 11 To visually confirm the different profiles of the differential WBC counts between the groups, discriminant analysis was performed using the five differential WBC counts as covariates and the disease groups as the categorical variable, followed by a canonical plot of the WBC differential counts by disease groups. Statistical analyses were performed using R Statistical Software (version 4.0.5; R Foundation, Vienna, Austria) and JMP Pro 16.0 (SAS Institute Inc., NC, USA).
Ethics
This study was approved by the Institutional Review Board of the Tohoku University Hospital School of Medicine (Approval No. 2020-4-072). All procedures were performed in accordance with the current version of the Declaration of Helsinki, revised in 2013. Written informed consent from the HCs was obtained from all enrolled volunteers. Written informed consent from the patient group was waived by the Institutional Review Board, and informed consent was secured by an opt-out manner.
Results
Participants
A total of 2852 patients (1271 men and 1581 women) who visited our department with miscellaneous complaints during the study period were initially recruited. After excluding ineligible patients based on the inclusion criteria, we enrolled 228 adult patients aged < 65 years (67 men and 161 women) without disease-specific objective diagnostic findings after comprehensive screening diagnostic tests and who were subsequently diagnosed with one or more of the aforementioned exclusion diagnoses. More specifically, patients with prolonged fatigability were confirmed to be negative for serum immunoglobulin M (IgM) antibodies for Epstein–Barr virus and cytomegalovirus, 12 while patients with prolonged slight fever were confirmed to be negative for blood cultures. Data were also obtained from 228 age- and sex-matched HCs (67 men and 161 women) without notable medical histories from among the whole 2492 healthy volunteers.
The demographic features and measured counts for each blood cell subtype in the symptomatic and HC groups are summarized in Table 1. Using the statistical significance of p < 0.005, only circulating monocyte count (p = 0.0014), basophil count (p = 0.0023), NLR (p = 0.0042), and MLR (p < 0.0001) differ significantly between the groups. Spearman’s ρ value between age and MLR was −0.06 (p = 0.3304) in HCs and + 0.03 (p = 0.6307) in the symptomatic group, suggesting that MLR was not influenced by age. The histograms for the MLR values in the 2492 healthy patients (Figure 2(a)) and 228 patients with unexplained physical complaints (Figure 2(b)) showed a higher range of values in the symptomatic group. Among the 2492 healthy population, 94.1% had MLR < 0.25.
Demographic and laboratory features of the symptomatic and HC groups.
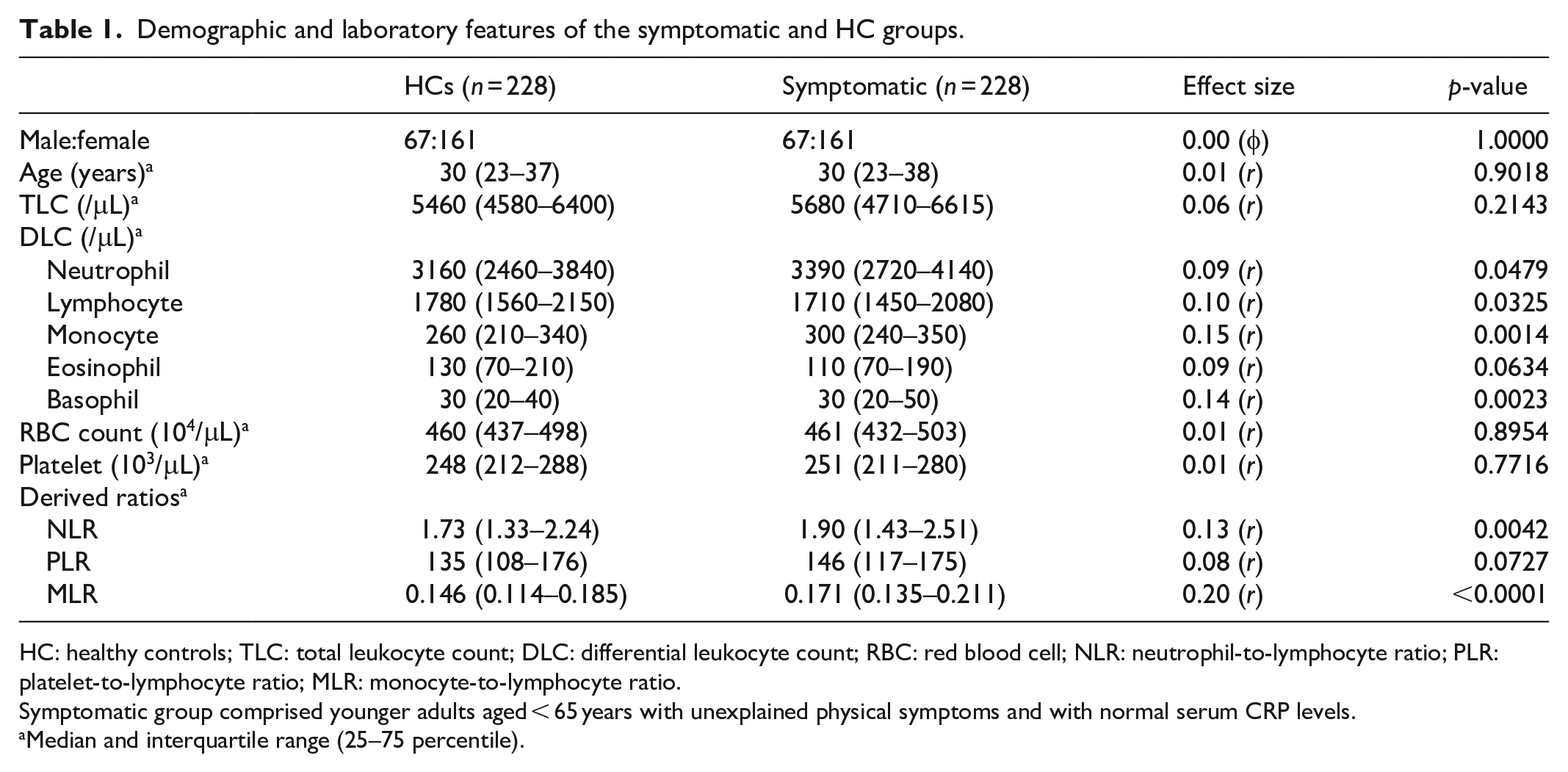
HC: healthy controls; TLC: total leukocyte count; DLC: differential leukocyte count; RBC: red blood cell; NLR: neutrophil-to-lymphocyte ratio; PLR: platelet-to-lymphocyte ratio; MLR: monocyte-to-lymphocyte ratio.
Symptomatic group comprised younger adults aged < 65 years with unexplained physical symptoms and with normal serum CRP levels.
Median and interquartile range (25–75 percentile).

Histograms of MLR values in the symptomatic and HC groups. Histograms of MLR values in the (a) healthy population (n = 2492), (b) age- and sex-matched HC and symptomatic patients, and (c) symptomatic group divided by the presence of nonfocal physical complaints, are shown. The distributions are positively skewed in both the symptomatic and HC groups and are higher in the symptomatic group. Within the 228 patients in symptomatic group, 63 patients with unexplained nonfocal physical complaints show higher MLR values compared to 165 patients with a single unexplained focal symptom.
MLR and nonfocal physical symptoms
Next, the clinical symptoms of symptomatic patients with elevated MLR levels were investigated. In total, 26 patients in the symptomatic group were with an MLR of ⩾0.25. The symptoms in these 26 patients included prolonged fatigability (10 patients, 38.5%), prolonged slight fever (7, 26.9%), widespread pain (8, 30.8%), and abnormal bowel habits with frequent diarrhea (6, 23.1%). The clinical profiles of the symptomatic patients with MLR ⩾ 0.25 (n = 26) are listed in Table 2. In contrast to the patients with elevated MLR, none of the 13 patients with low MLR values (< 0.10) showed fatigability, slight fever, widespread pain, or abnormal bowel habits (0.0% for all symptoms).
Characteristics of 26 patients with unexplained physical symptoms and with MLR > 0.25.

MLR: monocyte-to-lymphocyte ratio; ANSD: autonomic nervous system dysfunction; BPD: borderline personality disorder.
These three patients were classified into those with unexplained single focal physical symptom.
The histograms of MLR in symptomatic patients with unexplained single focal complaints and those with nonfocal physical complaints are shown in Figure 2(c). Patients with unexplained nonfocal physical symptoms showed higher MLRs. The prevalence of nonfocal physical symptoms in the subgroups with MLR values ⩾ 0.25, 0.20–0.25, 0.15–0.20, 0.10–0.15, and < 0.10 was 88.5% (n = 23/26), 39.0% (16/41), 23.1% (18/78), 8.6% (6/70), and 0.0% (0/13), respectively. The distributions of MLR in the presence of the aforementioned characteristic conditions are shown in Figure 3. The basophil count in 228 symptomatic patients was not associated with any of the above symptoms.

Dot plots for MLR by the presence of each popular symptom. Among the 228 patients with unexplained physical symptoms, significant differences in MLR values were confirmed by the presence of fatigability, slight fever, and widespread systemic pain. The presence of cough symptoms did not result in a difference in the MLR. Consequently, the MLR values were significantly higher in patients with unexplained nonfocal physical symptoms. The shown p-values are the results of Tukey’s post hoc test after the ANOVA.
Canonical plot with differential WBC counts
Based on the above findings that the profiles of the differential WBC counts may differ according to the clinical manifestations of symptomatic patients without known disease causes, a two-dimensional canonical plot was derived from discriminant analysis, which employed differential WBC counts as covariates and disease group as the categorical variable (Figure 4). The results did not differ between linear and quadratic discriminant analysis. The canonical plot showed a clear separation of the 95% confidence ellipse for symptomatic patients with nonfocal physical symptoms (n = 63) from those for symptomatic patients with a single focal complaint (n = 165) and for HCs (n = 228).
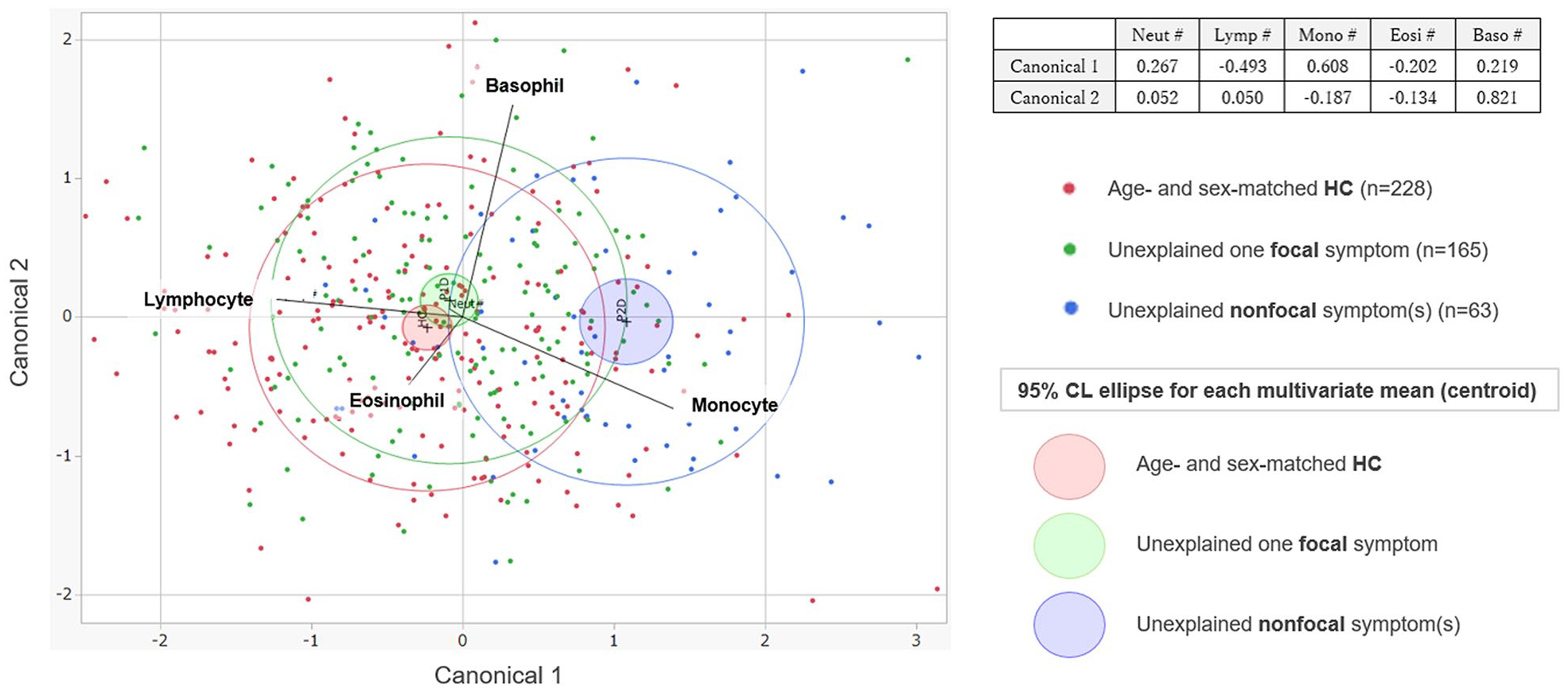
Canonical plots for discriminant analyses of WBC differential counts by disease group. Canonical plots by discriminant analysis, using the five differential leukocyte counts as covariates and disease groups as the categorical variable. The obtained plot shows a clear separation of the 95% confidence ellipses between patients with focal and nonfocal complaints. Each plot represents data from individual enrolled participants, while the filled ellipse represents the 95% confidence ellipse for the multivariate mean in each of the disease groups. The variable vectors show the correlations between the response variables and two dimensions of the canonical space.
Discussion
This study examined the WBC count profiles of patients with physical complaints without certain causes after comprehensive screening diagnostic examinations. The results showed that the counts of most types of blood cells did not differ between healthy volunteers and patients with unexplained physical complaints. Only MLR was slightly higher in the patient group. In particular, patients with an MLR > 0.25 (n = 26, 11.4%) were likely to also show nonfocal physical complaints with uncertain causes, with characteristic symptoms including fatigability, prolonged slight fever, and widespread pain. In contrast to the symptomatic patients, only 5.9% of the 2492 healthy participants showed MLR values > 0.25. Although the statistical difference was not strong, these findings implied that a high MLR value may be associated with the development of unexplained nonfocal physical complaints.
Currently, the exact role and clinical significance of circulating monocytes in peripheral blood remain largely uncertain. Circulating monocytes and differentiated cells in peripheral tissues protect the host from intruding microbial pathogens and clear waste products on tissue damage.13,14 Thus, invasion by undiagnosed microbial pathogens may explain the elevated MLR in some patients with unexplained physical complaints. However, all enrolled patients in this study had normal serum CRP levels and had normal findings on comprehensive diagnostic screening tests, including antibody tests for Epstein–Barr virus, blood cultures, whole-body CT imaging, and other relevant diagnostic tests. Thus, systemic infectious diseases were less likely. Additional studies are needed to determine whether an elevation in MLR could play a role in the development of the aforementioned nonfocal conditions, such as fatigue, slight fever, or widespread pain.
Another thing to be discussed is the potential roles of elevations in the NLR and basophil count, both of which were observed in this study, among patients with chronic complaints. An elevated NLR has been considered to reflect the presence of systemic inflammation from before, but the exact role and interpretation of an elevated NLR remain undetermined. A previous study suggested that elevated NLR might be associated with increased mortality rate among medical inpatients with multiple chronic conditions. 15 Furthermore, elevated NLR has been also reported to be present among patients with some psychiatric conditions, such as schizophrenia, bipolar disorders, bipolar disorders, and anxiety disorders. 16 These facts imply that elevated NLR may have a transdiagnostic pathophysiological effects that may be associated with a broad spectrum of clinical manifestations. The exact pathophysiological roles of basophils also remain largely uncertain. The least abundance of the basophils among WBC subpopulations and its phenotypic resemblance to mast cells could have made research on basophils difficult. 17 Meanwhile, there are several reports mentioning the potential roles of basophils in the early stage of some allergic, inflammatory, and autoimmune-related conditions.18–21 Most of the previous studies agree that the primary role of basophils would be modulatory actions, rather than effector actions. These facts may imply the possible presence of a prolonged mild inflammation that is undetected by the serum CRP levels in patients with unexplained prolonged physical or mental conditions. Future studies are needed to determine the potential roles of elevated NLR and basophils in the development of unexplained transdiagnostic conditions and the deterioration in the outcomes of physical and mental conditions.
A limitation of this study was that it did not evaluate the subtypes (i.e. classical/intermediate/non-classical) or levels of receptor expression in blood monocytes. Thus, whether the observed monocyte predominance was derived from inflammatory or anti-inflammatory subsets of monocyte remains unknown. 22 Another limitation was that a reasonable theory explaining the possible relationship between MLR and physical complaints is uncertain. A recent study reported that blood monocyte levels increased after acute physical stress in healthy volunteers, independent of monocyte subtypes. 23 Thus, the MLR may have been secondarily elevated due to physical distress. Meanwhile, higher blood monocyte and normal WBC counts are correlated with the course in some diseases, including cardiovascular and neurological diseases.24–27 Intervention studies may be needed to allow causal inferences between these variables.
Conclusion
The blood cell count profiles did not differ significantly between healthy volunteers and patients with physical complaints without known causes. However, some patients with unexplained nonfocal physical symptoms, such as fatigability, slight fever, or widespread pain, were more likely to show an elevated MLR of ⩾ 0.25. Further studies are needed to determine the possible role of elevated MLR in the development of unexplained nonfocal physical complaints.
Footnotes
Acknowledgements
The authors appreciate the volunteers who participated in the ToMMo project. The authors also thank the medical and administrative staff who participated in the collection of the data needed for this study.
Author contributions
T.A. performed statistical analyses and drafted the article. All authors contributed to data collection and critically revised the article. T.I., N.N., M.A., and A.H. supervised the study. All authors have read and approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the Institutional Review Board of the Tohoku University Hospital School of Medicine (Approval No. 2020-4-072). All processes were performed in accordance with the current version of the Declaration of Helsinki, as revised in 2013.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent from the HCs was obtained from all enrolled volunteers. Written informed consent from the patient group was waived by the Institutional Review Board, and informed consent was secured by an opt-out manner. Reason for obtaining opt-out informed consent from the patients group: This study enrolled all patients who visited the Department of General Medicine between 2018 and 2021, but written informed consent from the patients was started to be obtained from April 2019. Thus, the patients who visited the department between 2018 and 2019 were not obtained the written informed consent of this study. However, excluding these patients will make the sample size smaller and make the results of this study less reliable. Thus, the Institutional Review Board waived the written informed consent from the patient group for this study. We secured an opt-out period with the study protocol released on the homepage of the university for 6 months before starting this study.