
Abstract
Objective:
Metabolic syndrome is a collection of metabolic abnormalities that increase the risk of cardiovascular disease and diabetes. Therefore, this study investigated the effect of dietary and physical activities counseling on components of metabolic syndrome in school-age children with metabolic syndrome.
Methods:
This study is a randomized clinical trial on children aged 6–12 years (n = 60) that was conducted with metabolic syndrome. The participants were divided into three groups, the intervention group (including dietary counseling, physical activity counseling, and diet and physical activity counseling group) and a control group. The data collection method in this study was based on interviews with parents and completing a physical activity and nutrition questionnaire appropriate to the group, measuring blood pressure, blood sugar, high-density lipoprotein, triglycerides, and anthropometric indicators including height, waist, and weight. The intervention was carried out for 4 months. Data analysis was performed using SPSS21.
Results:
The results showed that there was a statistically significant difference between the means of abdominal obesity, hypertension, fasting blood sugar, high-density lipoprotein, and triglycerides in the three experimental groups (diet, physical activity, diet, and physical activity) and the control group (p < 0.001).
Conclusion:
According to the results of this study, counseling on diet and physical activity program execution is an essential base for controlling components of metabolic syndrome in children.
Introduction
Metabolic syndrome, insulin resistance syndrome, or X syndrome are terms used to describe a set of metabolic disorders that increase the risk of cardiovascular disease and diabetes. These disorders include insulin resistance, high blood pressure, hyperlipidemia (decreased high-density lipoprotein, elevated triglycerides), central or visceral obesity, type 2 diabetes, and exacerbated cardiovascular disease. 1 This syndrome was first described in 1988 and its diagnostic criteria were determined. Since then, its definition has changed several times and now there are various definitions of it. 2 It should be noted that the presence of two or more metabolic disorders along with abdominal obesity suggests metabolic syndrome in children and adolescents. 3 Obesity is a key risk factor for metabolic syndrome, especially abdominal obesity, which is a major accelerating factor in preventing cardiovascular disease and type 2 diabetes. 4 Overweight and obesity are the main features, along with abnormal metabolism of glucose, blood lipids, and high blood pressure. 5 In addition, it occurs due to abdominal obesity, hypertriglyceridemia, and decreased high-density lipoprotein levels. 6 As the proportion of the obese population continues to rise, the prevalence of metabolic syndrome in both children and adolescents is increasing. 7
The prevalence of metabolic syndrome using the International Diabetes Federation (IDF) criteria is 1%–7% for all communities and 16%–44% for the population of obese or overweight children. 8 On the contrary, metabolic syndrome is increasing in low- and middle-income countries. 9 According to another study, the prevalence of metabolic syndrome was between 0.3% and 26.4%. As a result, the increase in the number of children and adolescents with metabolic syndrome depends, in part, on the definition used. The IDF definition generally has the lowest prevalence (0.3%–9.5%), while the de Ferranti et al. Classification had the highest prevalence (4.0%–26.4%). 10 In this regard, according to the study results by Ahmadi et al., 11 the prevalence of metabolic syndrome according to IDF criteria in children and adolescents aged 10 to 18 years was 7.6% (9.4% in boys and 6% in girls).
On the contrary, the results of another study in Iran showed that the prevalence of metabolic syndrome in children is 1%–22%. 12 In this regard, according to the results of a study, the prevalence of metabolic syndrome among adolescents attending public schools in Dubai was 3.7%. 13 Also, the results of a study showed that the prevalence of metabolic syndrome in the population of Arab children is increasing, so this disorder increased to 11.8% in 2010, 20.1% in 2015, and 20.6% in 2019. 14
Early detection of metabolic syndrome components, especially among obese adolescents, is important for preventing cardiovascular complications in adulthood. 15 Many studies have confirmed that physical inactivity is an important factor in the development of chronic diseases such as metabolic syndrome, obesity, cardiovascular disease, and type 2 diabetes. 16 In this regard, according to the results of a study, family history of heart disease, living in urban areas, having a higher body mass index (BMI), and male gender were the main determinants of metabolic syndrome in adolescents. 11 On the contrary, the main reasons for the increase in the obesity epidemic and the subsequent components of the metabolic syndrome in childhood are excessive consumption of fats and fried foods, low fiber intake, overeating, and low levels of physical activity. 17
The results of the study showed a relatively high prevalence of metabolic syndrome in Beijing primary school students, and the researchers also stated that proper nutrition education could reduce the prevalence of the syndrome and improve its components. 18 In this regard, the results of another study showed that a 12-week intervention program based on physical activity, mental awareness, and nutrition for obese children (between 6 and 16 years old) is effective in improving blood sugar and triglyceride levels. 19 Research findings also show that multivitamin zinc supplementation with lifestyle intervention (diet and exercise counseling) has a more positive effect on metabolic syndrome risk factors in overweight children than lifestyle intervention alone. 20
However, the results of another study showed that short-term (2 weeks) but accurate diet and exercise can eliminate the components of the metabolic syndrome in children. 21 Managing a patient with metabolic syndrome requires an integrated approach with involvement, a team providing care including physicians, nurses, nutritionists, pharmacists, and social workers. In this, the nurse plays a pivotal role in implementing patient-centered treatment strategies with realistic goals and expectations. 22
Due to the increasing prevalence of metabolic syndrome in the world and in Iran and the lack of implementation of the researcher-selected technique in other studies (based on the time steps and the necessary follow-up when conducting research), researchers decided, in this study, to evaluate the effectiveness of physical activity and nutrition counseling on the components of metabolic syndrome in children with this disorder.
Materials and methods
This study is a Randomized Clinical Trial study (IRCT2013110815318N1) that was performed on children aged 6 to 12 years with metabolic syndrome referred to a specialized pediatric clinic in one of the teaching hospitals affiliated with Ahvaz Jundishapur University of Medical Sciences. Samples were based on inclusion criteria (minimum age of child 6 years and maximum 12 years, with the child of primary caregivers, the willingness of the child and his parents to participate in the study and not to use drugs affecting lipid metabolism, glucose, and blood pressure) and diagnosis of the metabolic syndrome as defined according to the definition of the IDF and according to the diagnosis of the relevant physician. To conduct this research, after obtaining the code of ethics (IR.AJUMS.REC.1392.141/CDCRC-9204) from the relevant university committee and written consent from the parents, as well as obtaining oral consent from the child in the presence of two witnesses based on voluntary participation in the research, collecting data over 4 months by providing information on the details, objectives of the study, and how the interventions were conducted.
Stratified random sampling was performed based on age and sex. First, according to the educational levels of the primary school, six age groups including 6–7, 7–8, 8–9, 9–10, 10–11, and 11–12 years were determined and then based on the sample size of 60 people. Considering three intervention groups (physical activity counseling group, diet counseling group, diet counseling group, and physical activity) and a control group, and using mini-tab software, 15 people for each group and a total of 60 people Sample title (including 50% drop in each group) were selected.
It should be noted that the design and implementation stages of this study are shown in the concert flow diagram (Figure 1).

Steps of design and implementation of the study.
The power calculation is as follows:
Sampling was based on 95% confidence and high power 99% with effect size and with 50% drop in each group according to Minitab tool 15 people in each group were considered. After power analysis, it is 99%

For each category, 10 people, including 5 boys and 5 girls, were selected in three intervention groups (diet counseling group, physical activity counseling group, diet counseling group, and physical activity) and 15 people in the control group.
The data collection method in this study was based on interviews with parents and completing a physical activity and nutrition questionnaire appropriate to the group, measuring blood pressure, blood sugar, high-density lipoprotein, triglycerides, and anthropometric indicators including height, waist, and weight.
In this study, data collection tools included three questionnaires. The demographic and anthropometric information registration questionnaire consisted of six questions and was organized into two parts. The first part was related to the demographic information of the child and her family, which examined the age, sex, level of education of the child and parents, and other factors. The second part contained information about anthropometric measurements, systolic and diastolic blood pressure, high-density lipoprotein, triglycerides, and fasting blood sugar. The second questionnaire was related to physical activity, which used the study of Pedrosa et al. 23 questionnaire and included six questions. For five questions, the answers were set as a 5-point Likert-type, and the options were assigned from 1 to 5 points according to the correct level of the child’s performance, and for one of the questions, the answer was set as yes or no, which was answered. Yes, one point and no answer was given zero points. Physical activity scoring was adjusted as scores below 50% weak, 50%–75% moderate, and above 75% good.
The third diet questionnaire used the child nutrition questionnaire. 24 This questionnaire (which includes 7 domains and 31 questions) examined the beliefs and attitudes of parents as well as child nutrition practices, focusing on obesity susceptibility in children.25,26 The answers to the questionnaire questions were set as a five-choice Likert-type and the options were assigned from 1 to 5 points according to the correct level of parental performance for one of the questions, the answer was set as yes or no, which was answered Yes, one point, and no answer was given zero points. Diet scoring was set below 50% poor, 50%–75% moderate, and above 75% good.
To measure blood pressure in this study, a manual sphygmomanometer made by Alpikado company in Japan was used; to control the weight, a digital scale made by Seca company in Germany was used; a tape measure made in China was used to measure height; and a cardio check device made in the United States was used to monitor blood sugar, high-density lipoprotein, and triglycerides. One week before the intervention, anthropometric indices including height, weight, waist circumference, as well as blood pressure, blood sugar, high-density lipoprotein, and triglycerides were measured by the researcher as follows: Children’s blood pressure was measured from the right hand after 10 min of rest using and before fasting. Then anthropometric indices including height, weight, and waist circumference were measured.
The weighing was measured with minimum clothing and without shoes with an accuracy of 100 g. Height in standing position and without shoes so that the heels are stuck together; and the hips, back area, and shoulders are placed along a straight line in front of the meter attached to the wall; and after tangling the gonium with the head, difference with an accuracy of 0.5 cm were measured. During normal exhalation, the waist circumference was measured (between the last rib and the iliac head) while standing. Levels of triglycerides, blood sugar, and high-density lipoprotein were measured using a capillary blood sample from the fingertip after 12 h of fasting. The validity and reliability of the physical activity questionnaire were confirmed based on the study of Pedrosa et al. 23 In addition, the validity and reliability of the child nutrition questionnaire have been confirmed based on the study of Birch et al. 24 It should be noted that the questionnaire used in this study has been validated and a pilot study was used. So, these two questionnaires were handed over to 10 faculty members of Ahvaz School of Nursing and Midwifery to check the validity of the content and after making the necessary corrections, the final version was compiled.
To determine the reliability of the data collection tool, questionnaires were given to 10 samples. After data collection, the internal correlation of the data was examined using Cronbach’s alpha with a coefficient of 85%. To confirm the reliability of the blood pressure measuring instrument, another arm mercury sphygmomanometer with the Alpikado brand was used and the two pressures obtained from each device were compared daily.
To measure the reliability of the scales, a standard 1 kg control scale was used daily. To confirm the reliability of the instrument for measuring blood lipids and blood sugar, after measuring blood lipids and blood sugar once, the same indicators were measured again 20 min later and the two digits obtained from the measurement of each item (such as blood sugar, high-density lipoprotein, and triglycerides) were compared for similarity. Then, an individual questionnaire for each child was completed by the researcher.
The intervention groups included three groups (diet counseling group, physical activity counseling group, diet counseling group, and physical activity) and a control group of 15 pairs (each pair includes a child and one of his parents) called A, B, C, D, respectively.
Group A
The children and their parents were placed in a group based on a nutrition education program. Before the intervention, a nutrition questionnaire for each child was completed by interviewing the parents and filling out the questionnaire by the Researcher. Nutrition scoring was done before the intervention based on the nutrition questionnaire and then the intervention began. The pieces of training consisted of four consecutive sessions with an interval of 1 week and lasting 120 min, which were determined by the researcher according to the studies and the implementation of the child nutrition questionnaire.
These sessions included discussions on obesity and childhood diseases, healthy eating habits, healthy cooking techniques, and reading food labels. The recommended diet included the consumption of carbohydrates and unsaturated fats along with increased consumption of vegetables and fruits. Healthy foods included whole grains, milk, yogurt, green leafy vegetables, fruits, and unhealthy foods including fast foods and sweets. 27 Educational pamphlets on healthy eating were provided to families.
Group B
Children and their parents were placed in a group based on a physical activity training program. Before the intervention, the physical activity questionnaire for each child was completed by interviewing the parents and filling out the questionnaire by the researcher, and the physical activity was scored before the intervention based on the physical activity questionnaire. The pieces of training consisted of four consecutive sessions with an interval of 1 week lasting 120 min, which were determined by the researcher according to the studies and the implementation of the physical activity questionnaire.
In these sessions, the importance of exercise for children and their parents was expressed. They were encouraged to use stairs instead of elevators and play outdoors. Attractive charts, including 45 min physical activity programs, were distributed among families, and parents were given educational counseling in training sessions. The exercise intervention regimen included 45 min of activity, which included the following. (1) Morning exercise regime: 10 min to warm up (stretching and strengthening exercises) and then 20 min of intense activity such as brisk walking, aerobics, cycling or club activities, and other sports activities. (2) Evening exercise regime: 20–25 min of outdoor play or any other sport. Children and parents were also asked to limit television viewing and video games to reduce sedentary behavior during the intervention program. 20
Group C
The children and their parents were placed in a group based on a nutrition education program and a physical activity education program. Before the intervention, the nutrition and physical activity questionnaire for each child was completed by interviewing the parents and filling out the questionnaire by the researcher. Diet and physical activity scoring were considered before the intervention based on the diet and physical activity questionnaire. The training consisted of eight consecutive sessions (lasting 4 weeks and lasting 120 min), with two sessions per week (one session on nutrition training and the second session on physical activity training). In these sessions, children and their parents received both group A and group B training. Of course, during these sessions, the child’s parents were taught how to fill in the child’s diet and physical activity checklists.
Group D
Children and their parents did not receive any formal education during this period, only the five risk factors of metabolic syndrome were measured at the beginning, during, and after the intervention. In addition, after receiving the results and completing the study in all three intervention and control groups, an educational session was held for the control group (providing attractive physical activity charts and educational pamphlets on having a healthy diet). After completing the educational pieces, to implement the educational pieces in daily life, the three test groups were given 4 months of opportunities. 25 During these 4 months, the researcher made telephone calls to the child and his or her family twice a week, on two special days previously informed, and answered any questions they might have. In addition, a telephone number was provided to them to contact the researcher in case of any problems in implementing the diet and physical activity program (formative evaluation). Parents of children were also asked to fill out a checklist for their child every week according to the test group.
It should be noted that the researcher during the intervention (45 days after the start of the intervention) and after 3 months of the intervention, at the beginning of the fourth month again anthropometric indices including height, weight and waist circumference, blood pressure, triglyceride levels, high-density lipoprotein, and fasting blood glucose were measured from the three intervention groups and the control group by the previous method. Also, the child-related questionnaire (for each group) was completed by the researcher through interviews with parents. The scoring of diet and physical activity after the intervention was evaluated according to the diet and physical activity questionnaire and also according to the group of each child. Data analysis was performed using SPSS software version 21 and all variables were tested for normality using Kolmogorov–Smirnov test before any statistical comparison. Also, the analysis of variance with repeated measures including sphericity test, epsilon correction factor, and Greenhouse Geiser test was used.
Results
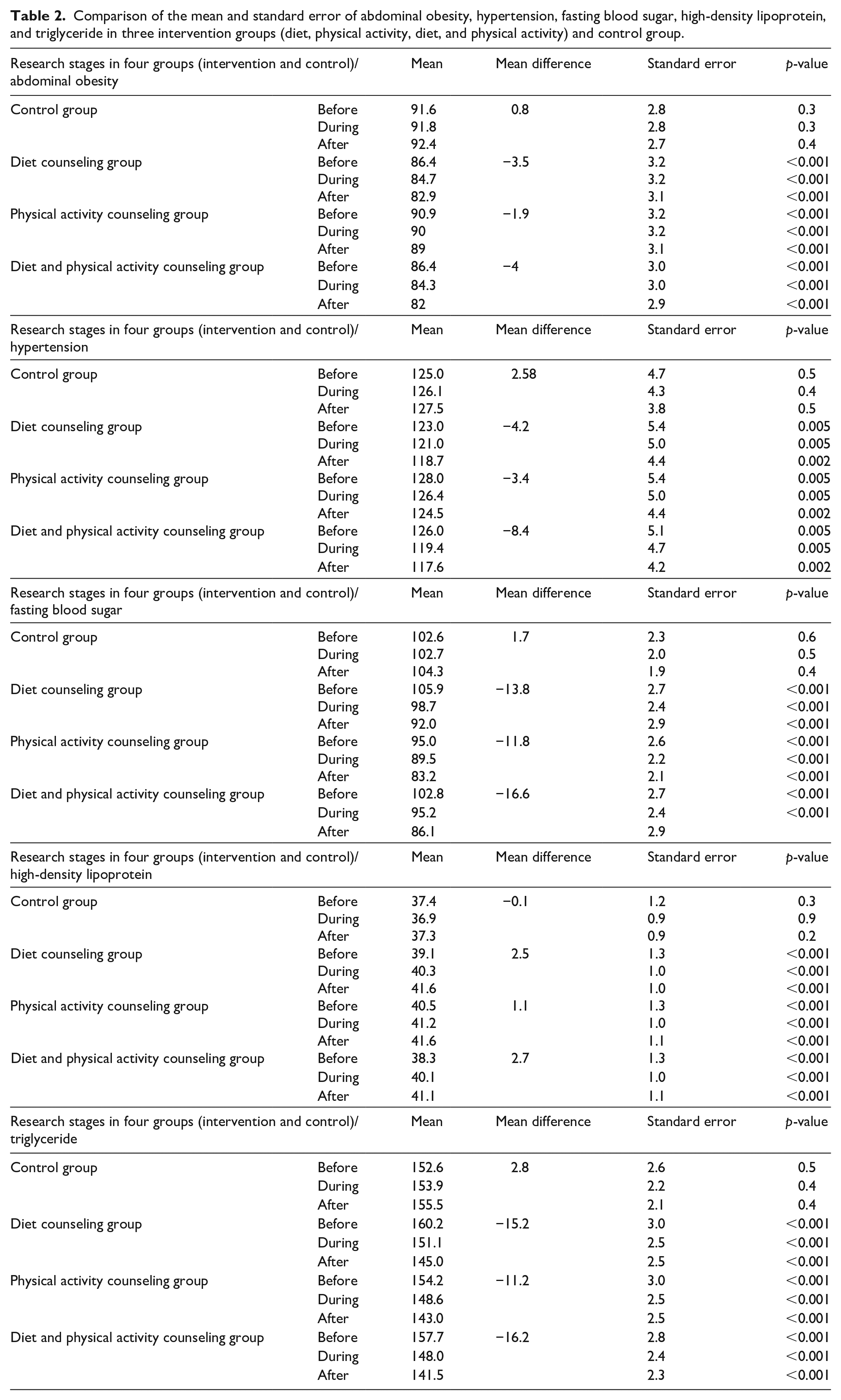
The results of the study showed the comparison of age, sex, and duration of breastfeeding in the three intervention and control groups, respectively, with p = 0.998, p = 0.997, and p = 0.352. No statistically significant difference was observed. Therefore, the four groups are homogeneous in terms of age, sex, and duration of breastfeeding (Table 1). The results of this study showed that the mean abdominal obesity of children in the diet counseling and physical activity group had the highest decrease compared to the control group after the intervention (p < 0.001).
Comparison of age, sex, and duration of breastfeeding in children under three intervention groups (diet, physical activity, diet, and physical activity) and control group.

The results showed that the mean of hypertension in children in the diet counseling and physical activity group had the highest decrease compared to the control group after the intervention (p < 0.001). The results showed that the mean fasting blood sugar of children in the diet counseling and physical activity group had the highest decrease compared to the control group after the intervention (p < 0.001).
The results showed that the mean of high-density lipoprotein in children in the diet counseling and physical activity group had the highest increase compared to the control group after the intervention (p < 0.001). The results showed that the mean of pediatric triglycerides in the diet counseling and physical activity group had the highest decrease compared to the control group after the intervention (p < 0.001).
Generally comparing the mean of all four groups, it was found that the diet and physical activity counseling group had the greatest effect on reducing abdominal obesity, reducing hypertension, lowering fasting blood sugar, increasing mean lipoprotein, and lowering triglycerides. After that, the diet counseling group and the physical activity counseling group are placed (Table 2).
Comparison of the mean and standard error of abdominal obesity, hypertension, fasting blood sugar, high-density lipoprotein, and triglyceride in three intervention groups (diet, physical activity, diet, and physical activity) and control group.
Discussion
In this study, the effect of both dietary intervention and physical activity for 4 months on different components of metabolic syndrome was performed. The results of this study showed that the implementation of both intervention methods, that is, diet counseling and physical activity, have a significant effect on the components of the metabolic syndrome in children of school age. Since the risk factors for metabolic syndrome in children are increasing, this study was performed on children aged 6–12 years. As soon as possible, the families of affected children with sufficient information should start the necessary changes to improve their children’s lifestyles. In this regard, Xu et al. 28 also chose their study in this age range and the results of their study also show the early onset of metabolic syndrome in children.
Based on the results of this study, it was found that in the three experimental groups (diet group, physical activity group, and diet and physical activity group) and control group, the number of boy patients was not much different from girl patients. The study by Friend et al. 8 noted the association between metabolic syndrome and other factors including obesity, age, and gender.
Perhaps one of the reasons for this discrepancy is the small number of samples in this study. A comparison of the frequency distribution of breastfeeding duration in the three intervention groups and control group shows that there is no significant difference in the duration of breastfeeding in the four groups. The results of several studies confirm that breastfeeding in infancy is an important protective factor against metabolic syndrome in childhood and adolescence. 26 A comparison of the mean abdominal obesity between the three intervention groups (diet group, physical activity group, and diet and physical activity group) and control group before, during, and after the study shows the diet and physical activity counseling group had the greatest effect on reducing abdominal obesity And then the diet counseling group and the physical activity counseling group are placed, respectively. Therefore, the results of this study in this regard are consistent with the results of research by Kamal and Ragy. As the results of their research also showed that 3 months of exercise in two groups of healthy obese children with metabolic syndrome reduces abdominal obesity and body weight and increases the amount of high-density lipoprotein. 16
A comparison of the mean score of hypertension between the three intervention groups (diet group, physical activity group, and diet and physical activity group) and control group before, during, and after the study shows that the mean of hypertension in children in the group of diet and physical activity counseling had the highest decrease and after that, the diet counseling group and then the physical activity counseling group are placed, respectively. It should be noted that according to the opinions of researchers so far, the treatment of MetS in childhood and adolescence is largely based on lifestyle intervention. 29
A comparison of mean fasting blood sugar between the three intervention groups (diet group, physical activity group, and diet and physical activity group) and control group before, during, and after the study shows that the diet and physical activity counseling group had the greatest effect on lowering fasting blood sugar and then, the diet counseling group and the physical activity counseling group are placed, respectively. Accordingly, the results of this study are consistent with the study by Khadilkar et al., 20 which showed that diet and exercise modification often have synergistic effects on fasting blood sugar and blood pressure.
Comparison of the mean of high-density lipoprotein between the three intervention groups (diet group, physical activity group, and diet and physical activity group) and control group before, during, and after the study shows that the diet and physical activity counseling group had the greatest effect on increasing high-density lipoprotein and then, the diet counseling group and the physical activity counseling group are placed, respectively. In this regard, the findings of this study are consistent with the findings of the study by Leão et al., 30 which indicate that interventions with a low-calorie diet combined with physical activity have better results in the treatment of metabolic syndrome.
Comparison of mean triglyceride between the three intervention groups (diet group, physical activity group, and diet and physical activity group) and control group before, during, and after the study shows that the diet and physical activity counseling group had the greatest effect on lowering triglycerides and after that, the diet counseling group and the physical activity counseling group are placed, respectively. In this regard, the results of this study are consistent with the results of the research by Khadilkar et al., 20 which also showed that adding exercise to a low-calorie diet improves high-density lipoprotein and triglyceride levels.
Although there is no consensus on appropriate strategies for the treatment of metabolic syndrome in this regard, few studies have been conducted on the effect of both dietary and physical activity intervention on the indicators of metabolic syndrome, according to which, it seems that both intervention methods performed in this study, when applied together, have direct effects on the improvement of various components of the metabolic syndrome and ultimately the treatment of the metabolic syndrome. This important action refers to confirming the general aspects of lifestyle changes and following a healthy, low-calorie diet with exercise to prevent metabolic syndrome.
It should be noted that the only limitation of this study was the loss of several research samples due to non-participation in an educational session. However, the limitation would be the sociodemographic details, age groups, or sample size. Therefore, it is suggested that researchers consider more samples to conduct such studies. Also recommended to provide an educational and practical guide to school principals in recognizing this metabolic disorder and proper implementation of diet and physical activity counseling to prevent this metabolic disorder. On the contrary, citing the results of this study, a general guide must be provided to the health team and those involved in the implementation of metabolic syndrome prevention and control programs. This is because research results have shown that the prevention of any metabolic disorder is more effective than its treatment.
Conclusion
The results of this study showed that the simultaneous implementation of both intervention methods, both diet counseling and physical activity, has a tremendous effect on the components of metabolic syndrome in children with the metabolic syndrome of school age. Therefore, due to the spread of unhealthy lifestyles, including lack of effective physical activity for children, as well as the use of inappropriate eating habits, it is expected that the occurrence of such chronic diseases in childhood will increase as rapidly as possible. In this regard, it can be concluded that providing coherent and regular counseling on physical activity and proper nutrition methods appropriate for childhood, can increase knowledge and improve the performance of parents to prevent metabolic syndrome at different ages of childhood.
Footnotes
Acknowledgements
This article is taken from the master’s thesis of nursing (IR.AJUMS.REC.1392.141/ CDCRC-9204; IRCTID: IRCT2013110815318N1). We would like to express our sincere gratitude to the Vice-Chancellor for Research and Technology of Ahvaz Jundishapur University of Medical Sciences, as well as to the esteemed parents without whom this project would not have been possible.
Author contributions
A.H. wrote the text of the article and responded to the reviewers. R.B. was involved in the data collection. K.A.A. contributed to the statistical analysis of data.
Availability of data and materials
The datasets used and/or analyzed during the study are available from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted after the approval of the Ethics committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1392.141/CDCRC-9204).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.
Trial registration
Iranian Registry of Clinical Trials: IRCT2013110815318N1.