
Abstract
Background:
Visual impairment is a functional limitation of the eye(s) or the visual system manifested as reduced visual acuity. At least 2.2 billion people have visual impairment worldwide, and 90% of people with visual impairment have either preventable or treatable causes with cost-effective interventions.
Objectives:
To assess magnitude of visual impairment and associated factors among primary school children in Ambo Town, Ethiopia, in 2021.
Methods:
A cross-sectional study was conducted in selected primary schools of Ambo Town. A simple random sampling technique was used to select schools and study participants. Data were collected using an interviewer-administered structured questionnaire and entered into Epidata version 3.1 for analysis by using SPSS version 23. Binary logistic regression was adopted to identify statistically significant factors which were associated with visual impairment. The Hosmer-Lemeshow test was used to evaluate how well the logistic regression model fits to the data.
Results:
About 780 out of 838 primary school children were enrolled in the study, yielding a response rate of 93.07%. The estimated prevalence of visual impairment was 8.8% with 95% CI: 6.81–10.79. The main risk factor for visual impairment among primary school children were Students’ grade level, exposure to mobile screen, family history of visual problems, and family awareness about the status of their child’s eye problems were significantly associated with visual impairments (AOR = 2.375, 95% CI: 1.079–5.226; AOR = 2.44, 95% CI: 1.401–5.01; AOR = 2.41, 95% CI: 1.071–5.42; and AOR = 4.503, 95% CI: 2.12–9.55, respectively).
Conclusion:
A high prevalence of visual impairment was observed among primary school children. Attending higher grades, being exposed to mobile screen, and having a family history of visual problems were significantly associated with visual impairment.
Introduction
The visual system is one of the most important sensory systems in humans. It is the primary means of integration between individuals and the external environment. Childhood visual impairments are underreported in developing nations.1,2 Eye health and vision have widespread and profound implications for many aspects of life, health, sustainable development, and the economy.3,4
Childhood and adolescence are crucial periods for visual development. Visual acuity matures rapidly, reaching full development by approximately at the age of 8 years. 5 It has been estimated that 75%–90% of all learning in the classroom comes to the students’ attention either wholly or partially via the visual pathway. 1 Therefore, visual impairment can affect their school performance and other functions. Visual impairment in childhood is a developmental emergency resulting in many disability-adjusted life-years lost. 5 Early screening and visual-aid interventions offer cost-effective mechanisms for unlocking human potential and improving the long-term health of future generations.6 –9
Globally, it is estimated that approximately 2.2 billion children and adults live with some form of vision impairment, and this figure is projected to increase unless appropriate measures are taken. The prevalence of visual impairment among children living in a developing country is related to the nutritional status in health, and socioeconomic status of that country.2,10
Ethiopia is believed to have one of the world’s highest rates of blindness (1.6%) and low visual health (3.7%) in the general population. Majority of visual problems (80%) is either treatable or preventable.2,11
Regarding regional differences, it is estimated that the prevalence of visual impairment is four times higher in low- and middle-income countries than it is in developed countries.6,12,13 There is extensive evidence showing that improving eye health contributes directly and indirectly to reducing poverty and improving work productivity.4,13
The majority of visual impairments can be corrected easily with early diagnosis and treatment to prevent long-term effects on human life. Most children with visual impairment do have uncorrected refractive error which is asymptomatic and usually overlooked by their parents and care givers. School-based eye screening programs are important for early detection and timely interventions. If early diagnosis and treatment are made, majority of visual impairment can be corrected easily to prevent long-term visual disability and improve the overall quality of life.4,14,15
There is limited data about the magnitude of visual impairment in school children in Ethiopia. Particularly in the study area, there is little to no study, which shows the prevalence of visual impairments among primary school students. It is critical to understand the magnitude and factors associated with visual impairments among school children. Therefore, this study aimed to assess the prevalence of visual impairment and associated factors among primary school children in Ambo Town, Ethiopia, in 2021.
Methods and materials
Study setting and design
A cross-sectional study design was conducted from September to November 2021 among 838 students in a primary school located in the Ambo Town West Shoa Zone, Oromia regional state. Ambo is the capital of the West Shoa Zone located at a distance of 114 km from Addis Ababa, the capital city of Ethiopia. In 2021, the Ambo Town Education Bureau reported that there were 16 primary schools, including seven private and nine public ones. Of the 22,335 students enrolled, 12,110 were male and 10,225 were female. 5
STROBE guidelines followed to prepare this manu-script.
Study population
All students who met the inclusion requirements in the primary schools chosen at random were included.
Inclusion criteria: All daytime learners, both in public and private primary schools, were included in the study.
Exclusion criteria: Nighttime students were excluded from the study. Two public and two private schools were randomly selected from 16 primary schools in Ambo Town.
Sample size determination and sampling techniques
The sample size was calculated using a single population proportion. Assuming 8.7% prevalence of visual impairments estimates which was taken from the study conducted in North West Ethiopia, a 3% margin of error, and a 95% confidence level, the computed sample size was 762. Considering a 10% nonresponse rate, the final sample was calculated to be 838. A simple random sampling technique was used to select both students and schools. Two public and two private schools were selected randomly by using lottery methods. Sample size was allotted proportionally based on a total number of students in each selected school.
Study variables
The outcome variable of the study is visual impairment.
Independent variables include: Environment-related variables, and Family-related variables.
Visual acuity is defined by National institute of health as a measure of the ability of the eye to distinguish shapes and the details of objects at a given distance.
Vision impairment is failure to see objects and its detail at 6 m what other normal people can see at a distance of 12 m.
Refractive error is a type of vision problem that makes it hard to see clearly. It happens when the shape of your eye keeps light from focusing correctly on your retina (a light-sensitive layer of tissue in the back of your eye).
Astigmatism is a condition in which an abnormal curvature of the cornea can cause two focal points to fall in two different locations, making objects up close and at a distance appear blurry.
Amblyopia is also known as lazy eye. It develops when there is a breakdown in how the brain and the eye work together, and the brain cannot recognize the sight from lazy eye.
If a child has amblyopia, one of his or her eyes has blurry vision and the other has clear vision. The brain starts ignoring the blurry eye and only uses the eye with clear vision to see. As the brain relies more on their stronger eye, the weaker eye’s vision becomes even worse over time.
Amblyopia is defined as the reduction of best-corrected visual acuity (BCVA) of one or both eyes that cannot be attributed exclusively to a structural abnormality of the eye. Amblyopia develops during childhood and results in the interruption of normal cortical visual pathway development. It is clinically defined as a difference in BCVA of two or more lines of acuity between the eyes.
Children having only one eye were excluded from the study because amblyopia is diagnosed by covering one of the child’s eyes and watch how well they can follow a moving object.
Hyperopia (Farsightedness) is the refractive error in which an image of a distant object becomes focused behind the retina, either because the eyeball axis is too short, or because the refractive power of the object is too weak.
Primary school children are students who are attending both first cycle primary school (grades 1–4) and second cycle primary school (grades 5–8) education (6).
Myopia (Nearsightedness) is a condition in which, an image of a distant object becomes focused in front of the retina, making distant objects appear out of focus.
BCVA is the measurement of the best vision correction that can be achieved using glasses or contact lenses.
Uncorrected visual acuity (UVA) is the visual acuity measured without correcting refractive errors or presenting VA in one or both eyes.
The better eye is the eye with superior VA on examination.
Data collection tools and procedures
Data were collected by two qualified optometrists using a standardized checklist. Data collectors conducted telephone interviews with family or guardians using structured questionnaires to gain information on the sociodemographic-, environment-, and family-related factors. Data collection tools were pretested on 5% of a final sample among primary school children in Guder Town.
For those who did not have telephone, data were collected moving house to house. Optometrists measure visual acuity, by using Snellen’s charts which is used to identify the smallest letters you can read on a standardized chart at a distance of 6 m. Each eye was tested separately at a distance of 6 m. Children with visual acuity less than or equal to 6/12 in one or both eyes were identified for further evaluation by an ophthalmologist. The ophthalmologist has used Retinoscopy (examination of retina by shining a light to eye so that it will be reflected off a retina) to objectively measure visual acuity (VA). Evaluation of ocular motility, refraction under cycloplegia, examination of the external eye, media, and fundus were done by ophthalmologist. Eight students were diagnosed to have visual impairments secondary to retinal detachment, corneal scar, and amblyopia. Surgery was done for one child at Minilik II hospital. Medical treatment and non-pharmacological counseling were given for the rest of children with eye problems in private and public health facilities located in Ambo Town.
Statistical analysis
Data were first checked manually for completeness and then entered into Epi-info version 7. Data are exported to SPSS version 25 for further analysis. Descriptive statistics and logistic regression were computed. The association between each independent variable and the outcome variable was analyzed by bivariate logistic regression. Variables with p-values less than 0.25 in bivariate logistic regressions were considered as a candidate for multivariable logistic regression a to adjust for the confounding effects. The Hosmer‒Lemeshow goodness of fit was used to test model fitness. A multicollinearity test was performed to check the correlation between independent variables by using the variance inflation factor (VIF), and variables with VIF > 10 were excluded from analysis. Finally, adjusted odds ratios with 95% confidence intervals were estimated to assess the strength of the association, and statistical significance was declared at p-value < 0.05 in the final model.
Ethical approval and consent to participate
The study was conducted following the declarations of Helsinki. Ethical approval was obtained from the Ambo University College of Medicine and Health Sciences Ethical Review Committee (Approval Number PGC/202/2021). The purposes of the study and study protocol were explained to the study participants. The risks, burdens, and benefits of participating in the study were fully explained to the study participants. The source of support for the study and institutional affiliations of the authors mentioned for the study participants. The participants were informed their right to refuse to participate in the study or to withdraw from the study at any time without reprisal. The study participant’s privacy and confidentiality were protected at the highest possible level. Written Informed consent was obtained from legally authorized representatives before the study. Respondents who were identified to have visual impairments during the study were given appropriate medical care with the support of individual volunteers and public facilities working on eye care in the study area. Referral linkage was facilitated to the next higher level of eye care center for those in need of further investigations and treatments accordingly.
Ethical Approval Committee members: Dr. Eshetu Ejeta, Mr. Gizachew Abdissa Mr. Getu Melese, Dr. Tadase Ejeta, and Mr. Edosa Kebede.
Results
Sociodemographic characteristics of the children
The study included about 780 out of 838 primary school children, with a response rate of 93.07%.
About 6.93% were refused to participate in the study. The children’s ages ranged from 7 to 17 years, with a median age of 12 years. Nearly half (50.5%) of the respondents were female, and 50.3% of them were attending grades 5–8. The majority of the participants 505 (64.7%) were selected from public schools (Table 1).
Sociodemographic characteristics of primary school children of Ambo Town, 2021.

The study reported that 652 primary school students had a history of exposure to television light and 63 (9.7%%) of them were visually impaired. The majority of the students 438 (67.3%) spent their time watching television for 2–4 h, whereas only a few of them 35 (5.8%) spent their time watching television for more than 4 h. The majority of respondents 484 (74.2%) sat at a distance of 2–4 m while watching a television. Only 104 (16%) primary school students watch television at a distance of less than 2 m. In this study, 359 (46%) participants reported a history of mobile exposure, with 22 (31.9%) of them being visually impaired. In contrast, 47 (68.1%) respondents who reported visual impairments had not any exposure to television or mobile devices.
Sociodemographic characteristics of parents or guardians
The median age of the parents was calculated to be 40 (SD ±10), and nearly half (413, 52.9%) of them were 35–46 years of age. The majority of the parents 669 (85.8%) were married, with 29 (3.7%) single, 41 (5.3%) divorcing, and 41 (5.3%) widowed. Significant proportion of parents/guardians 231 (29.6%) have attended college and above educational level, and only a few of them 51 (6.5%) were unable to read and write. The majority of the parents 338 (43.3%) who participated in the study were biological mothers, 302 (38.7%) were fathers, and the remaining 140 (17.9%) were legally authorized guardians of the children (Table 2).
Sociodemographic characteristics of parents/guardians of school children in Ambo Town, 2021.

Prevalence of visual impairments
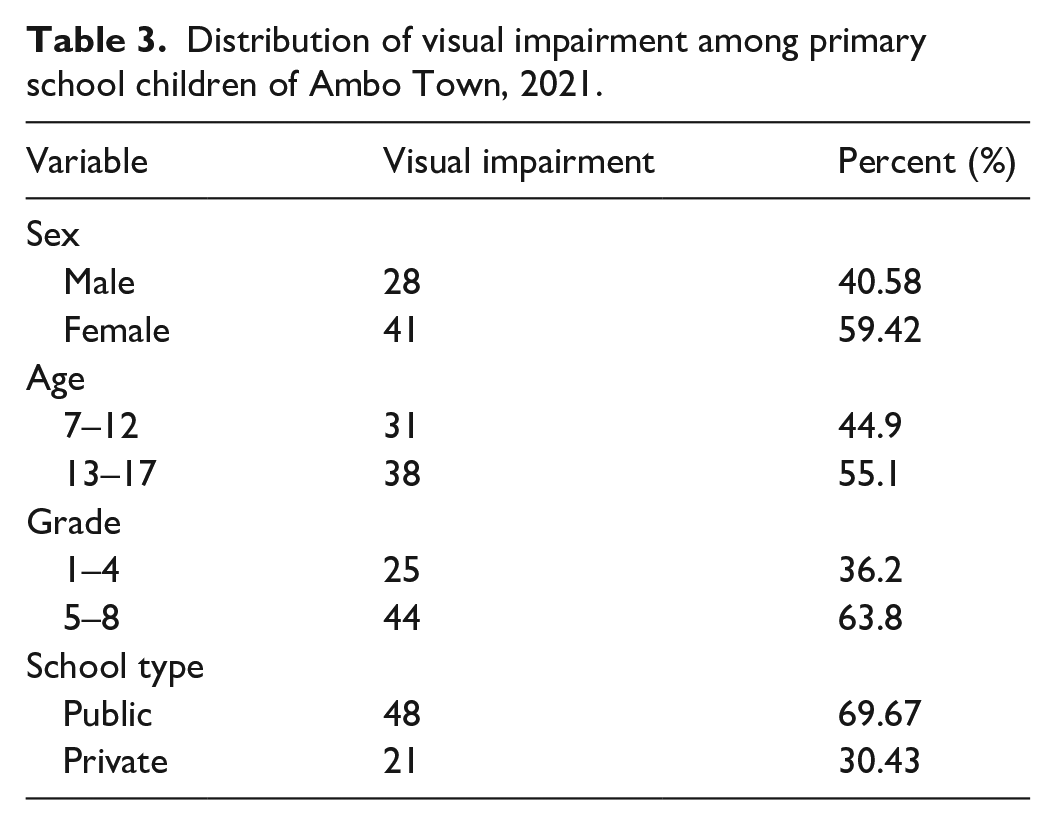
The prevalence of visual impairment among primary school children was determined to be 69 (8.8%) (95% CI: 6.81–10.79). Visual impairment was higher among female students compared to male students. The study also revealed that visual impairment differs by age and level of education. More than half (55.1%) of the students in the age range of 13–17 years and attending grades 5–8 were identified to have visual impairments. The majority of the students (69.9%) with visual impairments came from public schools (Table 3).
Distribution of visual impairment among primary school children of Ambo Town, 2021.
Refractive error was found to be the most common cause of visual impairment among 46 (55.4%) of the study participants followed by Amblyopia 16(19.27%), corneal scar 8 (9.3%), cataract 4 (4.8%), retinal detachment 2 (2.4%), and other cause 8 (9.64%) (Figure 1).

Risk factors of visual impairment among primary school children of Ambo Town, 2021.
Factors associated with visual impairments
The results of multivariable logistic regression analysis showed that students’ grade level, history of exposure to mobile screen, parent awareness about the eye status of their children, and family history of eye problems were significantly associated with visual impairments.
Based on the multivariable binary logistic results, student’s grade from 5 to 8 were associated with visual impairment (AOR = 2.37, 95% CI: 1.079–5.22). This suggests that the odds of developing visual impairments were 2.37 higher among students attending grades 5–8 compared to grade 1–4.
In addition, students who had exposure to mobile screen were 2.44 times (AOR = 2.44, 95% CI: 1.40–5.01) more likely to develop visual impairments than their counterparts. Family history of visual problems were associated with visual impairments. Students whose parents had a previous history of eye problems were 2.4 times (AOR = 2.41, 95% CI: 1.071–5.42) more likely to develop visual impairments than students without family history of eye problems.
Family awareness about health status of their children was also identified as a risk factor for visual impairments among children. The prevalence of visual impairments was higher among children whose parents were unaware of their children’s eye status. Lack of awareness by parents increased the risk of visual impairments among children by 4.5 folds (AOR = 4.503, 95% CI: 2.12–9.55) (Table 4).
Logistic regression analysis to identify factors associated with visual impairment among primary school children of Ambo Town, 2021.

COR: crude odds ratio; AOR: adjusted odds ratio.
Discussion
This study examined the prevalence of visual impairment and associated factors among primary school children in Ambo Town, Ethiopia 2021. Visual impairment has a significant effect on a child, family and country at large.15,16 The study findings showed that the prevalence of visual impairment among primary school students in the study area was 8.8%. This finding is in line with the previous study conducted in other parts of Ethiopia.15,17 In contrast, the findings of this study were lower than that of the previous studies conducted in Asia (14.5%), Bhutan (29.4%), Somalia (13.6%), and study conducted in other parts Ethiopia (12.4%).18 –21 The observed difference between the findings could be because of sample size differences, population, and timing of the study. Sample size used in those previous studies were 1204 for the study conducted in Somalia and 5060 for the study conducted in Bhutan. There are also slight socioeconomic and cultural differences between study areas.21 –23
However, the results of this study are higher than that of the previous studies conducted in South Africa (2.1%), Nigeria (7.2%), Khartoum Sudan (5.5%), and Kenya (2.4%).15,21,24,25 The difference could be attributable to the genetic and environmental differences of the study participants, sample size, and time of the study.26,27 Environmental factors include education, housing, metabolism, indoor and outdoor activities, and physical activity. Genetic irregularities in different chromosomes are highly associated with axial length and myopia.28,29 The sample size used for the study conducted in Kenya was higher (3400) compared to the current study which might be contributed to the observed difference.
Recent studies have confirmed the old observation that myopia most frequently occurs and develops during school-going age. The prevalence of myopia is particularly high in college and university students, whereas myopia rarely occurs in less educated populations.
This study showed a proportional relationship between visual impairments and student grade levels (p = 0.032). As the grade levels increase, the magnitudes of visual impairments also increase. This is consistent with a study conducted in Vietnam South Darfur State of Sudan and the Gurage Zone of Southern Ethiopia, which indicated an increased rate of visual impairments among higher-grade students.30 –32 This is probably, as the level of grade increases, additional indoor and outdoor activities and exposure including mobile screen exposure time also increases. Children who spend more time indoors are more likely to develop nearsightedness, according to a study conducted in Taiwan. 33 There is also a significant relationship between visual impairments and exposure to mobile screen. Exposure to mobile screen was found to be statistically associated with visual impairments (p = 0.003) in this study. This is supported by a study conducted among school children in Ireland and Bahir Dar16,17 showing a significant relationship between visual impairments and mobile screen exposure. This is attributable to the fact that children who were exposed to mobile screens are usually kept indoors. Children require time outside to play for the sake of their health as well as their vision because visual development starts in the womb and continues through childhood and adolescence. Each additional hour spent outdoors per week reduced the odds of having refractive errors by 2%.26,34
This study indicated that the most frequent cause of visual impairments was refractive error, which is consistent with a study conducted in the Sudan and Gurage zones of southern Ethiopia.30,31
Globally, the main cause of visual impairment was uncorrected refractive error, contributing to almost half (48.9%) of visual impairments among all people living with visual impairments. 2
Many studies have indicated the need to focus on avoidable causes of visual impairment among school students, including vision screening and awareness creation activities on a regular basis.35
We have used self-reported data to measure some variables in our study, which may either over estimate or underestimate a true value of some variables. To overcome this problem, we have pretested our data collection tools on a similar population ahead of the actual data collection. We gave also detail description about the purposes of our study for the study participants and the importance of providing genuine information.
Medical interventions
Those children diagnosed to have visual impairments from each school were linked to eye care clinics in collaboration with Ambo general hospital. Therefore, eyeglasses prescribed for 14 (20%) children and 4 (5.7%) of them who cannot afford to buy spectacles were given for free by donation from voluntary people in Ambo Town. Eight children (11.5%) with severe form of visual impairment were referred to Addis Ababa for further management and investigation. Out of eight children who were referred to Addis Ababa, surgery was done for one child at Minillik II Hospital, and the expense was covered by community health insurance. Medical care and counseling about eye care given for 47(68.1%).
Limitations
Data were collected only from schools in urban setting and may not reflect the reality in the entire society.
– Respondents may be too embarrassed to reveal private details; various biases may affect the results, like social desirability bias.
– Ocular pathology was not identified among children which may affect the diagnosis of amblyopia.
– Diagnosis of some eye problems depends on mere self-reporting from parents and children which may affect the accuracy the diagnosis.
– We cannot establish temporal relationship because of cross-sectional nature of the study design.
– Genetic makeup of the children and ocular motility were not examined during a diagnosis of eye problems.
– Children having only one eye were excluded from the study for the diagnosis of amblyopia which may have some negative effect on the prevalence visual problems.
– Some potential confounders like age may affect the diagnosis of eye problems.
Conclusion
The findings of this study showed that the magnitude of visual impairment among primary school children in Ambo Town was high.
Student grade, family history of visual impairments, and exposure to mobile screen were found to be significantly associated with visual impairments. School-based screening should be given at regular intervals for school children.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241236136 – Supplemental material for Prevalence of visual impairment and associated factors among primary school children in Ambo Town, Ethiopia, 2021
Supplemental material, sj-docx-1-smo-10.1177_20503121241236136 for Prevalence of visual impairment and associated factors among primary school children in Ambo Town, Ethiopia, 2021 by Nigist Legesse, Bayisa Abdissa, Zenabu Begna and Dereje Lemma in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241236136 – Supplemental material for Prevalence of visual impairment and associated factors among primary school children in Ambo Town, Ethiopia, 2021
Supplemental material, sj-docx-2-smo-10.1177_20503121241236136 for Prevalence of visual impairment and associated factors among primary school children in Ambo Town, Ethiopia, 2021 by Nigist Legesse, Bayisa Abdissa, Zenabu Begna and Dereje Lemma in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank Ambo University College of Medicine and Health Science, Department of Public Health, for the opportunity to undertake this research. Our thanks extend to Ambo General Hospital and Robe Medium Clinic for the provision of free health care services. We would also like to express our very great appreciation to each school principal, data collector, and study participant. We would like to express our special thanks to Dr. Haile Gemechu, Sr. Yenenesh Debebe, Ms. Seniet Tadele, and Mr. Bruk Legese for covering medical expenses at each level. We also acknowledge a preprint submitted to other journal in a due course.
Author contributions
NL and BA contributed to the conception and design of the work, methodology, and analysis of data and drafted the manuscript. ZB and DL contributed to reviewing the manuscript, analysis, and interpretation of the data, essentially revised the manuscript and wrote the final manuscript. All the authors have read and approved the final manuscript.
Availability of data and materials
All relevant data are available within the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from legally authorized representatives of the children.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.