
Abstract
Objectives:
The aim was to explore how the time to the first fall and 6-month fall incidence relates to rapidly and easily collected data in persons with acute stroke.
Methods:
Out of consecutively admitted patients with stroke at three stroke units, 284 with at least one follow-up were included in this prospective cohort study. During 6 months following discharge, participants reported falls using a diary and monthly phone calls. Data about participants’ characteristics, functions, and activities were collected during hospital stay and analyzed in relation to time to first fall by Cox regression and fall incidence by negative binomial regression.
Results:
Use of ⩾9 medications, paresis in arms, paresis in legs (National Institutes of Health Stroke Scale), impaired protective reactions in sitting (Postural Reactions Test), and limitations in self-care (Barthel Index) were decisive risk factors for time to first fall. Limitations in mobility (Step Test, 30-s Chair Stand Test) were decisive risk factors for high fall incidence (p < 0.0005).
Conclusion:
Several easily collected participant characteristics, functions, and activities were identified as risk factors for falls. The findings emphasize the width of assessments that can be used for the identification of individuals at risk for falls and that the risk factors vary in different strata of the population. These results are important when developing multivariate risk models. The risk factors differed in part when analyzing the time to the first fall and 6-month fall incidence.
Introduction
In persons with stroke, fall incidence rates between 1.3 and 6.5 falls per person-year have been reported, as compared to 0.7 falls per person-year in the general elderly population, 1 and risk factors differ in part from age- and sex-matched controls. 2 Therefore, studies of fall risk factors are needed for persons with stroke exclusively.
The risk of falls is multifactorial, and in persons with stroke, for example, impaired balance and mobility, disability in self-care, depression, cognitive impairment, use of sedative and psychotropic medications, and a history of fall have been suggested to be risk factors for falls. 3 In community-dwelling older persons, it has been shown that multifactorial interventions, including individual risk assessments, can reduce the rate of falls. 4 Due to the heterogeneous acute stroke population and multifactorial nature of fall risk, there is a need to study a wide range of possible fall risk factors. Such results are important both for individualized assessment of fall risk in clinical practice and for the development of multivariate risk models in different strata of the population.
Several studies have reported that the fall incidence after stroke is the highest soon after discharge.1,5,6 Therefore, to reduce the number and consequences of falls, it is important to identify the persons at risk as early as possible.
Some previous studies have data collection within a few up to 14 days after stroke onset and a prospective follow-up of post-discharge falls ranging from 6 weeks to 10 years.5–13 The methods for collecting falls differed, but most studies used only one method, such as a questionnaire or an interview. The statistical methods also differed between studies, but logistic regression was the most common. None focused solely on the assessments that are rapid and easy to use in clinical practice. Also, none analyzed falls with negative binomial regression (Nbreg), which has been recommended by Robertson et al. 14 Both Cox regression and Nbreg, the statistical methods used in this study, are analyses that allow for the fact that falls are frequent, recurrent events with a non-normal distribution and adjust for the follow-up time of individual participants. However, especially Nbreg is recommended since it allows for analyzing number of fall incidents in relation to time at risk. 14 This means that also participants not completing the entire follow-up period could be included in the analysis on the same terms as those with complete follow-up. Neither did any of the previous studies collect data on falls by daily recording and monthly reporting as recommended for satisfactory external and internal validity. 15 The aim of this study was to explore how the time to the first fall and 6-month fall incidence, relate to rapidly and easily collected data in persons with acute stroke.
Methods
Data availability
Requests for access to data can be submitted to the corresponding author.
Participants
Participants were consecutively enrolled in this prospective cohort study between 25 January 2016 and 10 February 2017. Inclusion criteria were a diagnosis of stroke (International Classification of Diseases codes I61, I63, or I64) and onset of symptoms within 2 weeks prior to testing; being resident in the catchment area; and with placement at the stroke unit of one of the three included hospitals: Ryhov County Hospital, Jönköping, University Hospital, Linköping, and Sunderby County Hospital, Luleå, Sweden. Exclusion criteria were risk of impaired health from being asked to participate in the study or professional interpreter needed for informed consent.
The study was approved by the Regional Ethical Review Board in Linköping (dnr: 2015/353-31 and dnr: 2018/199-32), and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained.
Data collection
Trained physiotherapists and occupational therapists working at the stroke units assessed the participants as soon as possible within 14 days from the stroke onset, allowing a 5-day period for test completion. A checklist (Supplementary Material) was used, providing details of when, where, and how data should be collected. The checklist was not validated, but established manuals and detailed protocols were used for all assessments. Please see supplementary material for an extended description of the assessments and cut-offs used and the analyses performed. Data on stroke location and type were collected using medical imaging, and when the stroke was verified only by clinical signs this was noted. Consciousness (first item of National Institutes of Health Stroke Scale) 16 was registered.
The data described below were collected to be analyzed in relation to falls since they have been identified as potential fall risk factors in previous studies or in our clinical experience.
Participant characteristics
Information on age, sex, body mass index, length of education, 17 general dizziness, dizziness when rising, depression during the previous year, previous stroke, joint problems, decreased sensibility in the hands or feet, days from stroke onset to admission to the stroke unit, length of stroke unit stay, discharged to home/elsewhere, and living alone was collected from medical journals and standardized patient interviews. Data on falls during the previous year and during the stroke unit stay were collected from the participant, family, or caregiver and complemented by data on falls registered in the National Quality Registry for Preventive Care. After collecting all data, the assessors made a general judgment of the risk of falling within a week, and within 6 months by answering the question “Do you judge the risk of falling within a week/6 months to be high or low for this person?” Data on medications at discharge were collected from medical journals and registered by the Anatomical Therapeutic Chemical Classification code. Medications were analyzed as the use of antidepressants, sedatives, antihypertensives, benzodiazepine-related drugs, beta receptor blockers, narcotics, number of medications, number of medications ⩾ 9, 18 and number of medications ⩾ 5 with N05BA, N05CD, N05CF or N06A included. 19
Functions
Several global and specific mental functions (International Classification of Functioning, Disability, and Health (ICF) code b110-b189) were assessed. Fear of falling, motor restlessness, sensory neglect, motor neglect, and visual neglect (by Star Cancellation Test (SCT)20–22) were assessed. The participants’ insights about their gait and visuospatial abilities were assessed by asking them for a Self-Reported Functional Ambulation Classification 23 (S-FAC) and if they believed they marked all stars in the SCT. Cognition was assessed using the Montreal Cognitive Assessment (MoCA),17,24 both as a total score, all the separate MoCA items by themselves, and in addition, the three visuospatial/executive items together, the three attention tasks, and the two language tasks. Impulse control 25 and latency in answers were also noted.
Touch function (ICF code b265) was assessed by touching the dorsal side of the hands/feet. Muscle power functions (ICF code b730) were assessed by the fifth and sixth items in the National Institutes of Health Stroke Scale, and handgrip strength was measured by the Jamar dynamometer.26,27 Movement functions (ICF code b750–b789) were assessed by the protective reactions in sitting and standing according to the Postural Reactions Test. 28
Activities
Self-care (ICF code d5) was assessed by items in the Barthel Index 29 and analyzed both as a total score and all items separately. Mobility (ICF code d4) was assessed by the Barthel items transfers, mobility, and stairs, and 30-s Chair Stand Test (CST), 30 Step Test (ST),31,32 ability to stand with no support for 10 s, FAC, 33 the Cone Evasion Walk Test, 34 and Timed Up and Go (TUG).8,35,36 In addition, TUG was performed with the Alternating Trail Making, and the Serial 7s attention task from MoCA added. Walking aids and wheelchair use were noted.
Follow-ups
The participants were given a fall diary for daily reporting of the number of falls and were contacted by telephone once a month for 6 months after discharge to report falls as recommended. 15 In cases where a monthly report was missing despite several attempts, data about potential falls were collected at next follow-up. Family or staff members reported falls when the participant could not. Falls registered in the National Quality Registry for Preventive Care were added. A fall was defined as “an unexpected event in which the participants come to rest on the ground, floor, or lower level.” 15 All falls were equally analyzed, regardless of underlying reasons, such as extrinsic and intrinsic factors, and if the fall was judged to be a consequence of the stroke or not.
Statistical analysis
Statistical analyses were performed using the software IBM SPSS Statistics for Windows (Version 26.0. Armonk, NY: IBM Corp).
Cox proportional hazard regression was used for analyses of relationships between the independent variables and number of days to the first fall incident, expressed as hazard ratio (HR) in the models. Cox regression is based on time-to-event data, where the event in this study is first fall incident within the study period. The time variable in the models is calculated as number of days to first fall incident or number of days to the end of study period for “surviving” participants (right-censoring). For categorical independent variables, an HR of 2 indicates that the risk of falling is twice as high in Category A compared to Category B over the entire period of the study. For continuous independent variables, a HR of 1.1 indicates that the risk of falling increases by a factor of 1.1 for every unit increase in the variable in question over the entire period of the study.
The proportional hazard assumption of Cox regression was tested with log-minus-log plots, entering each covariate as a stratum in the models, and by analyzing time-dependent covariates as a product of the time variable and each covariate. The proportional hazard assumption was assumed to be met if the curves in the log-minus-log plot were considered parallel and the time-covariate interaction had a p-value > 0.05. The assumption was not met for 12 independent variables. For these variables, analyses with 0–3 months and 4–6 months follow-up were performed and the risk for falls was found to be different for these two periods of time. The results for the 3-month follow-up analyses are presented in the supplementary material.
Nbreg was used for the analyses of relationships between the independent variables and fall incidence, expressed as incidence rate ratio (IRR) in the models. Fall incidence is calculated as number of fall incidents in relation to number of months in the study, expressed as falls per person-month. Nbreg was performed as a custom model with a negative binomial distribution and log link function. A robust estimator was used, with the natural logarithm of the number of months in the study as the offset variable. For categorical independent variables, an IRR of 3 indicates that the fall incidence is three times higher in Category A compared to Category B. For continuous independent variables, an IRR of 0.9 indicates that the fall incidence decreases by a factor of 0.9 for every unit increase in the variable in question.
All categorical and continuous independent variables used in the Cox regression models and Nbreg models are described in the three sections: Participant characteristics, Functions, and Activities.
In this explorative study, multivariable analyses were not performed since our aim was to present generalizable results of the fall risk connected to all single variables studied, including all participants in analyses.
A pre-study sample size calculation was based on the association between sex (men/women) and being a faller (yes/no). The sample size was calculated as for being able to detect a 10% difference in prevalence between two equally sized categories, using an alpha level of 5% and a beta level of 20%. A study with a power of 80% requires a total sample of 220 participants to test the association at 5% levels using chi-square test. To adjust for the estimated proportion of dropouts based on similar studies (up to 27%),6,8 300 subjects were finally included.
The persons who were eligible for the study but did not participate were compared with the participants using the independent samples t-test (age and days since stroke onset) and Pearson’s chi-square (sex). A p-value of less than 0.05 was considered significant.
Results
A total of 478 persons met the inclusion criteria, 178 of whom were not included for reasons described in Figure 1. Out of 300 persons consecutively enrolled in the study, 284 participated in at least the first follow-up and were included in the final analyses (Figure 1). No significant differences were found between the 284 participants and the 178 non-participants with respect to age, sex, or time since stroke onset. In mean, participants were included and assessed 5 days from stroke onset, and due to dropouts, the follow-up time was in mean 5.7 months. Numbers of participants at each follow-up and reasons for missing data are shown in Figure 1. Demographic characteristics of participants are presented in Table 1.

Flowchart of the recruitment process.
Demographic characteristics of participants.

SD: standard deviation; antidepressants corresponding to the Anatomical Therapeutic Chemical Classification code N06A; antihypertensives, C07, C08, and C09; Barthel, Barthel Index; benzodiazepine-related drugs, N05CF; beta receptor blockers, C07; BMI: body mass index; narcotics, N02A; SCT: Star Cancellation Test; Sedatives, N05A (but not N05AN), N05B, N05BA, N05CD, N05C (but not N05CF); TUG: Timed Up and Go; MoCA: the Montreal Cognitive Assessment.
Since 15 persons had two, three, or four stroke locations, the sum of persons having cerebellar-, brainstem-, left-, and right-hemisphere stroke is not 225.
Since 12 persons had both ischemic and hemorrhagic stroke, the sum of ischemic and hemorrhagic stroke is 12 persons more than 225.
During the 6 months of follow-up after discharge from the stroke unit, the fallers experienced in median 1 (1–18) fall (range) and 48 (0–178) days passed from discharge to the first fall. Only 20 (7%) of the participants experienced more than three falls. However, 118 (42%) participants fell, yielding an incidence rate of 2.22 (95% CI 1.73–2.86) falls each person-year.
The results are presented as risk factors and predictive assessments for early falls (number of days to first fall analyzed with Cox regression) and multiple falls (fall incidence analyzed with Nbreg). Variables with a p-value of ⩽0.01, in one or both analyses, are presented in Tables 2–4, and the most decisive risk factors for falls with p < 0.0005 are presented in the text below.
Participant characteristics in relation to the number of days to the first fall (Cox regression) and fall incidence (negative binomial regression) in persons with acute stroke (only variables with p ⩽ 0.01 in one or both analyses).

SD: standard deviation; HR: hazard ratio; CI: confidence interval; IRR: incidence rate ratio.
Stroke unit stay length (number of days), the number of days at the stroke unit was logarithmized using ln since there was a positive skewness in the variable.
Assumptions for Cox regression not met.
Function factors in relation to number of days to the first fall (Cox regression) and fall incidence (negative binomial regression) in persons with acute stroke (only variables with p ⩽ 0.01 in one or both analyses).

SD: standard deviation; HR: hazard ratio; CI: confidence interval; IRR: incidence rate ratio; MoCA: the Montreal Cognitive Assessment; S-FAC: Self-Reported Functional Ambulation Classification; SCT: Star Cancellation Test.
Assumptions for Cox regression not met.
Activity factors in relation to the number of days to the first fall (Cox regression) and fall incidence (negative binomial regression) in persons with acute stroke (only variables with p ⩽ 0.01 in one or both analyses).
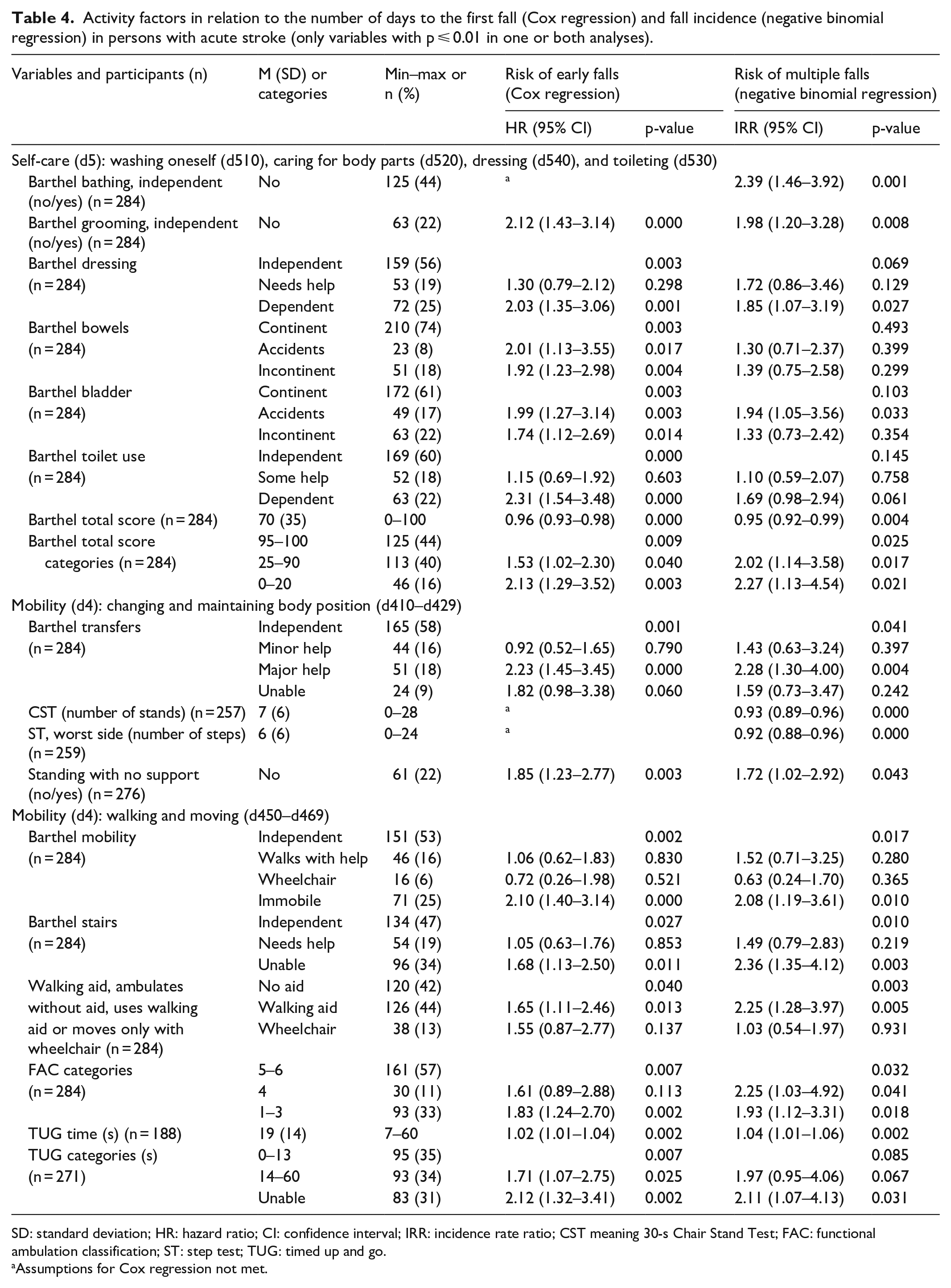
SD: standard deviation; HR: hazard ratio; CI: confidence interval; IRR: incidence rate ratio; CST meaning 30-s Chair Stand Test; FAC: functional ambulation classification; ST: step test; TUG: timed up and go.
Assumptions for Cox regression not met.
Please see supplementary material for the complete results of all variables included in the study.
Participant characteristics
Use of ⩾9 medications was a decisive risk factor for early falls, and the assessors’ judgment of risk of falling within 6 months was particularly well suited for the identification of individuals at high risk for multiple falls (Table 2).
Functions
Among the functions assessed in this study, the most decisive risk factors for falls were seen among the neuromusculoskeletal and movement-related functions (b7). In Cox regression paresis in the arms, paresis in the legs, and impaired protective reactions in sitting were decisive risk factors for early falls (Table 3).
Activities
Activities concerning self-care had a higher impact on the risk for early falls than on high fall incidence. A low Barthel total score, and dependency in the Barthel items grooming and toilet, can be used for the identification of individuals at high risk for early falls. Low numbers of repetitions in the CST and low number of steps on the worst side in ST can be used for the identification of individuals at high risk for multiple falls (Table 4).
Discussion
This study is the first to analyze falls both by time to first fall and fall incidence in relation to rapidly and easily collected data on persons with acute stroke. Such results are useful for advancing knowledge of clinical instruments and of how they can be used to identify high fall risk individuals and areas for prevention. Other valuable information obtained is that the risk factors for falls differ in part when analyzing time to first fall and 6-month fall incidence. The assessor’s judgment of risk of falling within 6 months was particularly well suited for the identification of individuals with a high risk for multiple falls. This also emphasizes the value of comprehensive risk analysis of a multifactorial phenomenon.
In this study, which included analyses of 95 factors, there are risks of type-I errors because of multiple comparisons, but there is no consensus in the use of statistical methods for adjustment of p-values.37,38 According to the Bonferroni correction, variables with p < 0.0005 should be considered significant in this study (p < 0.05/95 variables). However, strictly using the cut-off p < 0.0005 by the Bonferroni correction increases the risk of type-II errors.37,38 It is vital to bear in mind that scientific conclusions should not be based only on whether a p-value passes a specific threshold or not, and that the p-value does not measure the size of the effect or clinical importance. 39 Also, comparisons of HR/IRR and 95% CI between the different variables are not possible since both continuous and categorical variables were used, and the risk values are affected by the level of measurement and number of categories. In this article, variables with p-values < 0.0005 are presented as decisive risk factors, and in Tables 2–4, we present all variables with p ⩽ 0.01. We suggest that those are probably also factors possibly contributing to the risk of falls, and some of the factors only presented in the supplementary material. Also, the two analyses, Cox regression and Nbreg, complement each other and similar trends in both analyses strengthen the results. The two different methods provide an opportunity to study differences in fall risk factors of early or multiple falls. For example, dependence in self-care activities, paresis in the arms, and impaired protective reactions in sitting were decisive risk factors for falls when analyzed with Cox regression, indicating that assessments of arm function and activities performed at a physically less demanding level are particularly suitable for the identification of individuals at risk for early falls. In the Nbreg analyses, mobility activities assessed by tests that require performance on a physically more demanding level, such as CST and ST, were decisive risk factors for high fall incidence and might be more suitable for the prediction of multiple falls over time.
The finding that a low Barthel total score assessed in the acute phase of stroke can be used for the identification of individuals at high risk for post-discharge falls is in accordance with previous findings. 7 Noteworthy is that the most disabled individuals according to the variables Barthel transfer and walking aid were not the ones presenting the highest fall risk, which was also consistent with a previous study about impairments in acute stroke. 11 However, this emphasizes the need of considering U-shaped relations between abilities and risks.
As an alternative to time-consuming tests, often assessing more than one function or activity, our study shows that even short and specific tests, such as paresis in the arms and legs from the National Institutes of Health Stroke Scale, protective reactions from the Postural Reactions Test, and the items Barthel grooming, Barthel toilet, CST, and ST can also be used for the identification of persons at high risk for falls. The CST and ST showed similar predictive abilities, and impaired protective reactions while sitting was a determinant risk factor for early falls, whereas impairments in protective reactions in standing were not. This is clinically relevant information since patients and caregivers might be more comfortable pushing the patient to trigger a reaction by sitting than in standing.
No mental functions were seen among the risk factors for falls with p-values < 0.0005, but S-FAC, SCT, MoCA total score, and MoCA items of attention and visuospatial/executive functions seem to capture components that possibly contribute to the multifactorial risk for falls (Table 3). MoCA has previously been shown to have predictive abilities for falls in univariable, but not in multivariable analyses of falls in persons assessed in the acute phase of stroke,5,40 which is in line with the findings of this study.
Intake of a high number of medications was also a risk factor for falls in this study and is most likely a variable reflecting both general health and adverse effects of medications. The only group of medications that turned out as a possible risk factor for falls was antidepressant drugs, in line with a previous meta-analysis which identified both depression and psychotropic medication as risk factors for falls. 3
The data collection gives an extensive and detailed description of the characteristics, and the functional and activity levels of persons with acute stroke, and a presentation of their strengths as risk factors for falls. One limitation is the presence of confounding between the variables since factors, such as age, sex, previous strokes, or other diseases, were not controlled for. However, even if confounding is possible, it is valuable to know the predictive abilities for falls of commonly used assessments and to have a wide range of rapidly and easily collected assessments to choose among when assessing the individual patient in the heterogeneous acute stroke population. We aim to further analyze these data to identify risk patterns in subgroups of the acute stroke population to find predictive models.
Other possible limitations are that fatigue and natural recovery in persons with acute stroke may have influenced the results, and that the assessments were performed at different days after stroke onset. However, controlling for the number of days from stroke onset until assessment did not significantly change the results.
We designed the study to be as representative of the acute stroke population as possible and the wide inclusion criteria capture the heterogeneity in the population and contribute to high external validity. Another possible limitation is that medical imaging was not an inclusion criterion for this study. However, computed tomography does not always identify the infarction if carried out within the first hours from the onset of stroke, 41 and since the diagnosis of ischemic stroke can be made accurately on the basis of the clinical presentation without a new computed tomography or magnetic resonance imaging in many patients, 42 neuroradiological verification was not required for inclusion. Moreover, since the medical diagnosis is sometimes delayed, the inclusion criteria were a diagnosis of stroke and onset of symptoms within 2 weeks prior to testing, which also can be seen as a limitation considering that acute stroke generally is defined as the first 7 days from stroke onset. 43 Another limitation is that the checklist used for the data collection had not been pilot-tested or validated.
In a previous study of persons above 60 years of age, 13%−32% did not recall a confirmed fall during the previous 3, 6, or 12 months. 44 The studious collection of falls in this study aimed to decrease the problem with recall bias. Falls were reported in 42% of the participants during the first 6 months after discharge in this study, which is higher compared to 26%−35% in three previous studies of persons with acute stroke with self-reports followed up at longer intervals.5,7,8 The findings in this study might indicate that a larger proportion of fall incidents are collected by fall diaries and monthly follow-ups since the three other studies5,7,8 collected data at sparser intervals.
Other strengths are the large sample size, the prospective design, the use of both Cox regression and Nbreg, including the time aspects in the outcome variables, the consecutive inclusion of participants, and that the participants were given spoken and written information about the fall definition used. The collection of falls within 6 months from discharge, not from stroke onset as in previous studies,5,7,8,40 is also a strength since different living environments might influence the results.
At first, analyses were performed with a 12-month follow-up period, but the risk for falls changed significantly over time in several variables and thus the proportional hazard assumptions were violated. In the presented 6-month follow-up, only 12 variables violated the assumptions. Future studies are needed investigating for how long assessments performed in the acute stage are valid risk factors for falls.
Conclusion
Several easily collected participant characteristics, functions, and activities were identified as risk factors for falls. The findings emphasize the width of assessments that can be used for the identification of individuals at risk for falls and that the risk factors vary in different strata of the population. These results will be important when developing multivariate risk models. The risk factors differed in part when analyzing the time to the first fall and 6-month fall incidence.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221088093 – Supplemental material for Exploring possible risk factors for time to first fall and 6-month fall incidence in persons with acute stroke
Supplemental material, sj-docx-1-smo-10.1177_20503121221088093 for Exploring possible risk factors for time to first fall and 6-month fall incidence in persons with acute stroke by Hanna Sjöholm, Staffan Hägg, Lars Nyberg, Jonas Lind and Ann-Sofi Kammerlind in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221088093 – Supplemental material for Exploring possible risk factors for time to first fall and 6-month fall incidence in persons with acute stroke
Supplemental material, sj-docx-2-smo-10.1177_20503121221088093 for Exploring possible risk factors for time to first fall and 6-month fall incidence in persons with acute stroke by Hanna Sjöholm, Staffan Hägg, Lars Nyberg, Jonas Lind and Ann-Sofi Kammerlind in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the participants, their families, and the dedicated staff for their valuable contribution to this study. They specially thank Christina Sellin and Sebastian Murtola for data collection, and Henrik Hedevik and Bo Rolander for statistical work. Information about falls was complemented with data on falls registered in the National Quality Registry for Preventive Care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Regional Ethical Review Board in Linköping (dnr: 2015/353-31, and dnr: 2018/199-32). Dnr: 2015/353-31 is the original application, and dnr: 2018/199-32 is an additional application regarding the permission to include falls registered in the National Quality Registry for Preventive Care.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Futurum Region Jönköping County (grant nos. FUTURUM-394751, FUTURUM-422461, FUTURUM-484411, and FUTURUM-519431), the Swedish Stroke Association, and the Medical Research Council of Southeast Sweden (grant nos. FORSS-475481, FORSS-645491, and FORSS-931033).
Informed consent
Written informed consent was obtained from the subjects before the study. Persons who could not give informed consent due to cognitive impairments were included without giving consent, as permitted by the ethical approval.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.