
Abstract
Objective:
To investigate the demographic and clinical characteristics of fall-related deaths in Chinese communities and provide clinical insights for fall prevention strategies.
Methods:
A retrospective study was conducted on decedents (n = 1455) from a deeply aging urban community (Kaiyuan, Quanzhou, China) between 2020 and 2024. Fall-related deaths were identified by screening death certificates for specific keywords, with confirmation documented in the cause of death. Demographic, clinical, and temporal trend analyses were conducted. Kaplan-Meier and multivariate Cox proportional hazards regression were used to identify factors associated with survival time from fall to death.
Results:
Fall-related deaths constituted 5.5% of community deaths, predominantly affecting individuals aged ⩾60 years (93.8%). Significant gender differences were observed in marital status, occupation, and education level (all p < 0.05). Age-standardized mortality rates fluctuated from 9.17 to 16.29 per 100,000 population (2020–2024) with no significant temporal trend (Z = 0.490, p = 0.624). Univariate survival analysis revealed a notably shorter median survival in patients with comorbidities (1.0 vs. 6.0 months, p = 0.116). Multivariate analysis identified age of fall (Hazard ratio (HR) = 1.023, 95% Confidence interval (CI): 1.001–1.046, p = 0.044) and comorbidities (HR = 1.793, 95% CI: 1.022–3.147, p = 0.042) as independent predictors of shorter survival.
Conclusion:
Fall-related mortality is a major public health issue among older adults in the community. Advanced age of fall and comorbidities are key factors independently associated with shorter post-fall survival. Evidence-based multidimensional prevention and management interventions are essential to alleviate the fatal burden of falls.
Introduction
Falls represent a critical global public health challenge as the second leading cause of unintentional injury death worldwide. It was surpassed only by road traffic injuries, with more than 80% of these deaths occurring in low- and middle-income countries. 1 From 1990 to 2021, the global number of fall-related cases increased significantly from 326.9 million to 540.88 million. 2 During the same period, the mortality rate per 100,000 population first decreased from 23.21 to 11.01 (in 2009) and then rebounded to 12.50 (in 2021), with a projected further rise to 19.48 by 2040. 3 Additionally, it is estimated that nearly 300 million people worldwide will experience falls by 2045. 2
Falls often necessitate long-term care and institutionalization, imposing substantial economic burdens on healthcare systems and families.4,5 In China, injuries rank as the second leading cause of death among older adults (⩾60 years), with mortality rates increasing exponentially with age, particularly beyond the age of 80. 6 Fear of falling further restricts activity and diminishes physical function. 4 While overall injury mortality in China declined during 2010–2019, age-standardized mortality rates (ASMRs) from unintentional falls have recently risen. 7 Regional variations in the epidemiology of falls exist due to geographical, lifestyle, and healthcare disparities.
Research on falls leading to mortality in community settings in China remains limited, which hampers the development of targeted prevention strategies. Addressing this gap is urgent given the accelerating demographic shift to an older population. This study analyzes fall-related deaths within a single Chinese community to inform localized prevention strategies.
Materials and methods
Study setting and population
Kaiyuan Community, located in the Licheng District of Quanzhou City, is a representative “deeply aging” urban community. The registered permanent population is approximately 61,000, with over 14.2% aged 65 years and above. The community health center serves the area with 30 beds, 30 physicians, and 14 nurses. For this study, “community deaths” are operationally defined as deaths registered at the community health center. Data were obtained from death registration records and linked resident health archives held by the Kaiyuan Community Health Service Center between 1 January 2020 and 31 December 2024. The data sources were reviewed for completeness. Cases with missing critical information (as defined in the exclusion criteria) were not included in the final analysis.
Case inclusion was based on death certificates. Specifically, we identified potential fall-related deaths by searching for keywords (“fall,” “tumble,” “knock down,” “run down”) within the narrative section describing “history and signs/symptoms before death” in the death investigation records. Fall-related deaths were strictly defined as fatalities in which either a fall was confirmed as the underlying cause of death (per International Classification of Diseases, 10th Revision (ICD-10) codes W00-W19), or the death certificate’s causal inference section explicitly verified a direct link between the fall-related incident and the fatal outcome. 8
Exclusion criteria were: (1) records with incomplete key variables (age at death, gender, or underlying cause of death); or (2) cases where the fall event was not assessed to be a direct or major contributing cause of death upon standardized independent review by two researchers of the full death certificate narrative. Any discrepancies between reviewers were resolved through consensus or by a third senior researcher. The study was approved by the Ethics Committee of Kaiyuan Community Health Service Center (Approval No: 2025-KY-002-01). Given the retrospective design and the use of anonymized, de-identified data from routine death registration records that cannot be linked to individual participants, the requirement for written informed consent was formally waived by the above-mentioned Ethics Committee. All procedures were performed in accordance with the Declaration of Helsinki.
Data collection and variables
A retrospective analysis was conducted in this study to collect the following variables: demographic characteristics (age of death, age at the time of fall, gender, marital status, education level, and occupation), documented comorbidities, and other relevant information. These comorbidities were coded as present or absent (binary) based on a predefined list (including hypertension, diabetes, coronary heart disease, stroke, and chronic obstructive pulmonary disease).
Mortality rate calculation
Crude Mortality Rate (CMR): number of annual fall-related deaths in the community divided by the total community population in the same year.
ASMR: computed via direct standardization, with reference to the WHO 2000–2025 World Standard Population and official age weights applied for standardization. 9
Statistical analysis
Continuous variables were summarized as mean ± standard deviation if normally distributed, or median (25th, 75th percentiles) if non-normally distributed. Categorical variables were presented as counts (percentages). Group comparisons (including gender-based analyses) were performed using Chi-square tests. Temporal trends in crude and ASMRs were analyzed, with significance assessed using a non-parametric test for trend. Survival analysis was performed using Kaplan-Meier estimates with Log-rank tests for univariate assessment. A multivariate Cox proportional hazards model was constructed to adjust for potential confounders, including age of fall, gender, marital status, education level, and occupation. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated. Statistical significance was set at p < 0.05 (two-tailed). Analyses were performed using SPSS 25.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic characteristics
Among 1455 community deaths, 80 (5.5%) deaths were fall-related deaths (Male: 35, 43.8%; Female: 45, 56.3%). The mean age at death was 87.0 (79.3, 91.0) years; 93.8% were ⩾60 years (Figure 1). Most (83.7%) were born before 1949.

Age of death distribution of fall-related deaths.
The median time from fall to death was 5.0 (1.0, 22.5) months. Statistically significant gender-based differences were observed in marital status, occupation, and education level (Table 1): females had a higher proportion without spousal status, while males were more likely to be retired and have education levels above junior high school. Age of death (predominance of females in the >87 years group, p = 0.067) and comorbidity status showed no significant differences for gender.
Comparison of clinical characteristics by gender in fall-related deaths.

All percentages represent the proportion within each gender group.
Temporal trends (2020–2024)
Annual fall-related deaths were 14, 20, 16, 14, and 16, corresponding to CMR of 20.25, 28.83, 23.08, 20.31, and 23.28 per 100,000 population, respectively. The ASMR was 9.17, 16.29, 11.67, 12.07, and 14.30 per 100,000 population, respectively. Mortality exhibited an initial decline followed by a recent increase (Figure 2). Statistical analysis of the 5-year mortality trends revealed no significant ordered trend over the 5-year period (Z = 0.490, p = 0.624), indicating the absence of a consistent upward or downward pattern in fall-related mortality rates.
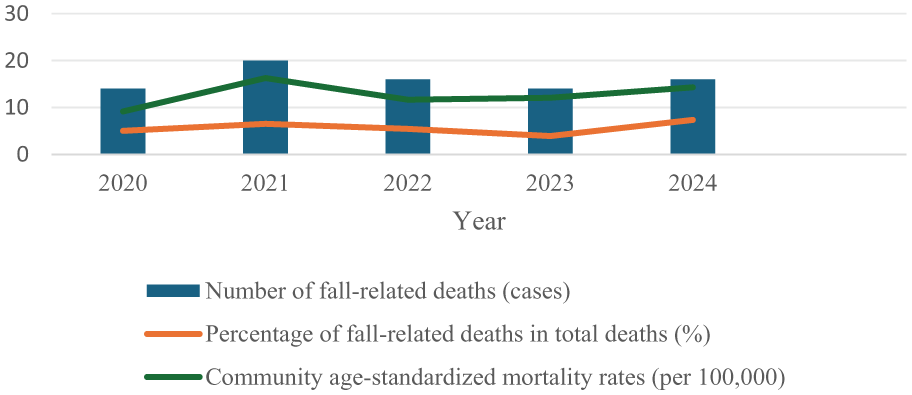
Five-year trend of fall-related deaths (2020–2024).
Patient characteristics and univariate survival analysis
Kaplan-Meier survival analysis with Log-rank tests was performed to evaluate the impact of various demographic and clinical factors (gender, marital status, occupation, educational level, and comorbidity) on survival. None of the factors reached statistical significance in the univariate Log-rank tests (p > 0.05).
However, notable trends were observed. Patients with higher education (above Junior High) had a numerically longer median survival (12.0 months) compared to those with lower education (4.0 months). Most strikingly, patients with comorbidities exhibited a markedly shorter median survival (1.0 months (95% CI: 0.0–4.9)) versus those without comorbidities (6.0 months (95% CI: 2.4–9.6)), with a p-value approaching marginal significance (p = 0.116), which are visually illustrated in the Kaplan-Meier survival curves stratified by comorbidity status (Figure 3(a)).

Multivariate Cox proportional hazards regression analysis
To identify independent prognostic factors while adjusting for potential confounders, a multivariate Cox proportional hazards model was constructed, incorporating all variables from the univariate analysis plus the age of fall. The results are presented in Table 2.
Multivariate Cox proportional hazards analysis of factors associated with survival.

SE: Standard error; CI: Confidence interval; HR: Hazard ratio.
Multivariate analysis identified two factors as independent and statistically significant predictors of mortality:
Age of fall
Each 1-year increase in age was associated with a 2.3% increase in the hazard of death (HR = 1.023, 95% CI: 1.001–1.046, p = 0.044).
Presence of comorbidity
Patients with comorbidities had a significantly higher risk of death compared to those without (HR = 1.793, 95% CI: 1.022–3.147, p = 0.042). Cox-adjusted survival curves depicting the time from fall to death stratified by comorbidity status are presented in Figure 3(b).
Other factors, including gender, marital status, occupation, and education level, did not demonstrate independently prognostic value in the adjusted model (all p > 0.05). The omnibus test for the overall model was not significant (χ² = 8.441, p = 0.208), suggesting that while specific factors are significant, the collective set of variables may not fully capture the determinants of survival. That indicated the potential influence of unmeasured confounders.
A forest plot illustrating the clinical characteristics associated with the time from fall to death is presented in Figure 4.

Forest plot.
Discussion
This study delineates key clinical characteristics of fall-related mortality in a Chinese community cohort. Our findings confirm that fall-related deaths constitute a nontrivial burden of community mortality, and predominantly affect individuals aged 60 years and older. This finding aligns with the global pattern of falls being a leading cause of injury death in the elderly. 3
Regarding social and demographic patterns, we observed notable gender-based differences. The disparity in marital status likely reflects the greater longevity of women in China, leading to a higher prevalence of widowhood. Conversely, the educational gap is largely associated with sociohistorical factors, such as limited access to formal education for women in the pre-1949 birth cohort, which constitutes a significant part of our sample. While prior studies and our data indicate a higher proportion of males among fall-related deaths, we found no significant gender-based difference in survival time from fall to death. 10 Similarly, neither retirement status nor educational level demonstrated an independent association with post-fall survival in our multivariate model. This observation is consistent with previous research suggesting that socioeconomic status may not be a strong predictor of long-term prognosis after falling. 11 Collectively, this may imply that in the context of fatal fall outcomes, the direct biological vulnerabilities conferred by advanced age and comorbid conditions outweigh the broader influence of socioeconomic factors.
The ASMR for falls in our community was consistent with recent global estimates. 2 While several studies have projected an upward trend in fall-related mortality, our findings are inconsistent with this. This may be attributed to the fact that, in this specific context, although the disease burden caused by fatal falls is substantial, it may not be increasing systematically.3,12 This nonsignificant trend should be cautiously interpreted, given the relatively short observation window and limited sample size.
The most salient finding of this study is the confirmation that both advanced age at the time of fall and the presence of comorbidities are independently associated with significantly shorter post-fall survival. This finding starkly illustrates the heightened vulnerability from the cumulative decline in physiological function related to aging and chronic disease.13,14 Specific comorbidities such as congestive heart failure and metastatic cancer have been previously implicated in higher post-fall mortality. 15
Translating these findings into prevention, a strong evidence base supports the efficacy of structured exercise interventions—particularly strength and balance training—in improving functional capacity and reducing fall risk among older adults.16,17 Consequently, major guidelines, including those from the US Preventive Services Task Force, endorse exercise programs for fall prevention in at-risk community-dwelling seniors. 18 Broader global recommendations advise that all older adults receive counseling on falls prevention and physical activity. 19 Primary care is pivotal in this effort; opportunistic screening for fall risk should be followed by a comprehensive, multifactorial assessment for high-risk individuals, leading to codesigned, multidomain interventions. Environmental modification also remains a cornerstone of prevention. Given that falls frequently occur on roads, stairs, and within the home environment, systematic implementation of home-hazard assessments and modifications, along with the appropriate provision of assistive devices, is essential for mitigating risk in vulnerable populations. 20
However, the nonsignificant omnibus test for our final model hints at the potential influence of unmeasured confounders—including both the absence of data on key factors (e.g. medications, functional status, living arrangements, and environmental factors) that restrict mechanistic insight and unrecorded variables such as fall severity, injury type, and care quality—highlighting the need for future prospective studies incorporating these elements. The study’s other limitations include: its retrospective, single-center design and modest sample size, which limit statistical power and generalizability; lack of data on community-level fall incidence rates (due to non-seeking care or out-of-center hospitalization), which restricts the analysis of population-level fall burden; and case identification based on keyword searches, which may have introduced misclassification bias.
Conclusion
This community study confirms that fall-related mortality is a major public health concern for older adults. Advanced age at fall and comorbidities are key factors independently associated with shorter post-fall survival. In clinical practice and public health strategies, evidence-based multidimensional preventive and management interventions should be implemented to reduce the fatal burden of falls. Future research should incorporate more detailed variables related to injuries and clinical courses to more clearly identify the key factors influencing post-fall survival.
Footnotes
Ethical considerations
This research is a retrospective study and has been approved by the ethics review committee to waive informed consent. The study protocol adhered to the ethical principles of the Helsinki Declaration (1975) and was approved by the Ethics Committee of Kaiyuan Community Health Service Center (Approval No: 2025-KY-002-01).
Author contributions
H.Z., Y.D., and Z.Zhou contributed to the conception and design of the study. Z.Zhang, Z.W., and M.D. collected the necessary data. Z.Zhou performed the statistical analysis. Y.D. and H.Z. wrote the first draft of the manuscript. All authors contributed to the revision of the manuscript and approved the submitted version. All authors agreed to take responsibility for the contents.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work had the financial support of Quanzhou City Science and Technology Program (Grant Number: 2025QZNY114).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.