
Abstract
Background:
Youth faces various sexual and reproductive health problems in developing countries like Ethiopia. Major health problems like unintended pregnancy, unsafe abortion, and sexually transmitted infections are common among youth in Ethiopia. This study aimed to determine the level of utilization of youth-friendly reproductive health services and associated factors among youth in Aleta Wondo town, southern Ethiopia, from 20 to 30 June 2020.
Methods:
A community-based cross-sectional study was conducted among youths of Aleta Wondo town from 20 to 30 June 2020. A total of 421 study participants were selected from households of selected kebeles in the town by using a systematic random sampling method. Data were collected using structured pretested face-to-face interviewer-administered questionnaires. The data were entered using Epi-data version 4.4.2 and exported to SPSS version 25 for analysis. Bivariate and multivariate logistic regression models were used to determine factors significantly associated with the utilization of youth-friendly reproductive health services. Adjusted odds ratio and 95% confidence interval with p value of <0.05 were considered to declare statistical significance.
Results:
The level of utilization of youth-friendly reproductive health services was 32.8% (95% confidence interval = 28.0%–37.0%). Youth-friendly service utilization was significantly associated with being female gender (adjusted odds ratio = 2.20, 95% confidence interval = 1.34–3.62), living alone (adjusted odds ratio = 2.99, 95% confidence interval = 1.48–5.77), who had not ever discussed with their parents (adjusted odds ratio = 0.46, 95% confidence interval = 0.27–0.81), have visited service required and missed service (adjusted odds ratio = 1.96, 95% confidence interval = 1.19–3.24), and have sexual partner (adjusted odds ratio = 4.52, 95% confidence interval = 2.75–7.44).
Conclusion:
Youth-friendly reproductive health service utilization among youth Aleta Wondo town was low. Factors like gender, current living place, have ever discussed in reproductive health issues with their parents, have visited health facility and missed service, and having sexual partner were predictors of youth-friendly service utilization. It is better to work in collaboration with youth clubs and schoolteachers to scale up youth-friendly service.
Introduction
Youth-friendly services (YFSs) are services that are accessible, equitable, comprehensive, efficient, acceptable, and appropriate for the youth. They are in the right place at the right price (free where necessary) and delivered in the right style to be suitable to young people, and are effective, safe, and affordable. They include counseling, family planning, voluntary counseling and testing (VCT), and treatment of sexually transmitted infection (STI) as defined by the World Health Organization (WHO). 1
Young people (age 10–24 years) are main population group with a great potential for physical, mental, and psychological development. Every year, an estimated 1.7 million youths lose their lives early due to reproductive health (RH) problems. Due to these reasons, adolescents’ RH is becoming an ever more vital component of global health. 2
Ethiopia is a nation of young people, above 65% of its population is below 25 years of age, and is a country whose youth have strong RH needs. Among the many sexual and RH problems faced by youth in Ethiopia are gender inequality, sexual coercion, early marriage, polygamy, female genital cutting, unplanned pregnancies, closely spaced pregnancies, abortion, STIs, and AIDS. Lack of education, unemployment, and extreme poverty exacerbate and perpetuate the RH problems faced by Ethiopian youth. 3
Young people aged 15–24 years accounted for almost half (42%) of the infection reported worldwide, of whom 80% are living in sub-Saharan Africa. There are only 28% women and 36% men who have knowledge about HIV in this region. 4
The WHO stated that about one-half of all HIV infections occur globally among people aged 25 years and less than 25 years. In addition, up to 100 million youths become infected with curable sexually transmitted diseases. In Africa, it was estimated that 60% of all new HIV infections occur among the youth aged 15–19 years. 5
According to the Ethiopian Demographic and Health Survey (EDHS) of 2016, among the age group of 15–24 years, HIV prevalence was 0.3%. The utilization of family planning services in the existing health care system by youth was also very low (14%). As a result, there is a high rate of unwanted pregnancies which often result in unsafe abortions and their complications.6,7
According to the national study done by the federal ministry of health on selected urban areas of Ethiopia, Sidama region was one of them which showed that youth couldn’t appropriately utilize the available health service. 8 Moreover, currently, there is no nongovernmental organization (NGO) working on YFS and there is also only one Health institution in the town.
Youth often lack basic RH information and access to affordable and confidential health services. The study on utilization of youth-friendly reproductive health services (YFRHSs) is important for the improvement in the quality of life of the youth. The prevalence and factors associated with YFS in the study area were not well known. Thus, understanding the prevalence and associated factors of YFS utilization is important to address the problems and help local government officials and any concerned bodies to take care of and revise strategy in this area. Therefore, this study was aimed to assess the utilization of YFRHSs and associated factors among youth in Aleta Wondo town, southern Ethiopia, from 20 to 30 June 2020.
Methods
Study setting, design, and period
The study was conducted in Aleta Wondo town, southern Ethiopia. Aleta Wondo is located at a distance of 64 km away from Hawassa, the capital city of Sidama regional state, and 333 km far away from Addis Ababa, the capital city of Ethiopia. The population of the town in 2012 E.C is estimated to be 55,036. From this, youth population is 10,615.9,10 The town is divided into three kebeles. In the town, there is one government hospital, seven private medium clinics, and 17 primary schools, including private, two secondary schools, and one technical training institution/college. The number of facilities offering the YFRHS is only one hospital in the town and the health workers who have got the YFS training at the facility were six. There are no NGOs working on YFS currently.
A community-based cross-sectional study was carried out to assess YFS utilization and associated factors among youth in Aleta Wondo town, southern Ethiopia. The study was conducted from 20 to 30 June 2020.
Population of the study
The source population of this study was all youth (15–24 years) in the town where all youth who were in the town during the data collection period were the study population.
Eligibility criteria
All youth aged 15–24 years in Aleta Wondo town were included while those youths who were unable to respond and seriously ill were excluded.
Sample size determination and sampling technique
The sample size was determined using single population proportion formula: n = (z α /2)2 p (1 − p) / d2 = (1.96)2 × (0.469) × (1 – 0.469) / 0.052 = 383, where n = sample size, p = proportion of YFRHS in Bale zone (46.9%), 11 d = margin of error = (5%), α = level of confidence = 95% (1.96). Considering 10% non-response rate, the calculated sample size was 421.
The study was done in the Aleta Wondo town which has three kebeles within it. All kebeles were included in this study. The number of respondents was assigned proportionally to the household size of each kebeles in the town. A pre-survey was conducted before the actual day of data collection in order to identify the number of youths in the study area and to develop a sampling frame. The first household from each kebeles was identified using the lottery method, and then the systematic random sampling technique was used to determine the next household to be included. Youths who were available in the selected households were interviewed. For the HHs which had more than one youth, the interview was done by selecting a youth by a lottery method.
In case, if there was no youth in the selected HH, the youth in the immediate house was interviewed. Every ninth HH was selected in each kebele and then the first HH was selected by using the lottery method.
Variables of the study
Dependent variable
Utilization of YFRHSs (Yes/No).
Independent variables
Sociodemographic and cultural factors: age, gender, education, religion, and ethnicity.
Knowledge factors: awareness of RH facility, source of information.
Health care system factors: availability of YFS, convenient working time, distance from the health facility, cost of services.
Operational definitions
Youth: Participants who were at the age of 15–24 years in this study.
YFRHS utilization: It was measured by asking the respondents history of utilizing one or more RH services components (family planning, VCT, STI treatment and diagnosis, condom service, pregnancy test, pregnancy care, abortion care, and general information, education and counseling on RH issues) in the past 12 months. Eight items were used to measure the utilization of YFRHS for the last 12 months. At least one YES response among the eight items qualifies the respondent for using SRHS.12,13
Data collection methods and procedures
A pretested structured face-to-face interviewer-administered questionnaire was used to collect the data. The questionnaires were close-ended and adapted by reviewing literature, and suited to the local situation.14–16 The questionnaires were first prepared in English language and then translated to Amharic language and back into English language to ensure consistency between the two versions. The data were collected by trained clinical nurses and health extension workers, and supervised by 2 supervisors.
Data quality management
Data collectors and supervisors were trained and a questionnaire guide was prepared. The pre-test was carried out 2 weeks before the actual data collection period at 5% of youths in Yirgalem town and based on the findings of the pre-test the questionnaires were modified. On every night of data collection day, the collected data were checked for completeness and consistency by the principal investigator and supervisors and communicated to data collectors.
Statistical analysis
The data obtained from each respondent were entered using Epi-data version 4.4.2.1 and exported to SPSS version 25 for analysis. Descriptive statistics (frequency, mean, and standard deviation) were used to describe the study population in relation to relevant variables. Bivariate and multivariate logistic regression models were used to assess the presence of any association between each independent variable and dependent variable. Adjusted odds ratio (AOR) was used to know and ascertain any association between the independent and dependent variables while significance was declared using a 95% confidence interval (95% CI). Those candidate variables at bivariable logistic regression with a p value of <0.25 were moved to multivariable logistic regression model for the dependent variables to control potential confounding variables. The p value of <0.05 at multivariate analysis was considered as statically significant to this study.
Results
Sociodemographic characteristics of study participants
There were a total of 429 study participants with a response rate of 100%. Among these, 226 (53.7%) were males and 251 (59.7%) were between 20 and 24 years old, with a mean age of 20 (±2.69). A majority of the respondents, 226 (53.7%) and 200 (47.5%), were Sidama by ethnicity and Protestant by religion, respectively. A total of 322 (76.5%) of the respondents were single and 81 (19.2%) were married. Among the 421 respondents, 247 (58.7%) of their parents’ residents were urban. A majority of the respondents (223 (53.3%)) live with their families.
A majority of the respondents (389 (92.4%)) had formal education, and among those, a total of 187 (48.5%) had higher education. Regarding the respondents’ fathers’ educational status, 292 (69.4%) had a secondary and above level of education. Concerning the respondents’ mothers’ educational status, 263 (63%) had secondary and above level of educational status. Only 134 (31.8%) of the participants gained pocket money and the remaining (287 (68.2%)) did not gain pocket money (Table 1).
Sociodemographic characteristics of youth in Aleta Wondo town, Sidama regional state, Ethiopia, 2020 (N = 421).

SD: standard deviation.
Wolayita, Gamo, Tigre, and Oromo.
Hawariyat, Pagan, and Jehovah Wittiness.
RH knowledge–related factors
Among 421 participants, a majority of respondents (279 (66.3%)) heard about YFS. Among those who heard about YFS, a majority of the respondents (168 (60%)) had heard about family planning, followed by VCT (55.5%). Only 87 (31.1%) had ever heard only one type of YFS and the remaining (192 (62.9%)) had ever heard about two and more types of service.
A majority of the participants (84%) knew the place where YFSs were delivered. Among the respondents, a majority (82%) thought that YFRHS could improve youths’ health. Only 140 (33%) of the study participants reported that they had a parental discussion about the issue of sexual health and RH services (Table 2).
RH knowledge–related factors in Aleta Wondo town, Sidama regional state, Ethiopian, 2020.

YFRHS: youth-friendly reproductive health service; VCT: voluntary counseling and testing; STI: sexually transmitted infection; SRH: sexual and reproductive health.
The main source of information for the study participant was friends/peers (116 (42%)), followed by health care providers (109 (39%)). Among the total respondents, a majority (241 (86%)) had 2 and more sources of information (Figure 1).

Source of information on YFRHS in Aleta Wondo town, Sidama regional state, Ethiopia, 2020.
Health system factors in Aleta Wondo town, Sidama regional state, Ethiopia
Of the respondents who heard about YFRHS, 214 (76.7%) had known about the availability of the YFRHS facility in their living surroundings. A total of 144 (67.2%) of the study participants said that they were requested to pay for the service. More than half (53%) were convenient to use YFS. Among those who were asked the option of their convenient time to use the service, 70 (47.6%) mentioned that in the hour users were not around as a convenient time, followed by 56 (38.1%) late the afternoon and 21 (14%) early in the morning. Of the total of 214 respondents, a majority (113 (53%)) responded as it needs 30–60 min, 77 (36%) responded as it needs less than 30 min, and 24 (11%) responded that it needs more than an hour for a single journey to reach the health centers to utilize YFS services by walking from residence.
YFS utilization in Aleta Wondo town
Of the total respondents, 138 (32.8%, 95% CI = 28.0%–37.0%) reported that they have ever used the YFRHS service in the past 12 months (Figure 2). Among those who had ever used the services, 82 (59.4%) used VCT service, making it the most utilized, followed by condom (77 (55.7%)) and family planning (71 (51.4%)). Ninety-six (69.5%) of the study participants had used more than one type of service, whereas 42 (0.5%) used only type one service (Figure 3).

Youth-friendly service utilization in Aleta Wondo town, Sidama regional state, Ethiopia, 2020.

The type of services utilized by the study participants in Aleta Wondo town, Sidama regional state, Ethiopia, 2020.
Among the participants who had ever used the YFRHSs, a majority (86 (62%)) received the services from Hospital found in the town, followed by youth club (24 (25%)) and private clinics (18 (13%)). Among the respondents who had ever used the services, a majority (65 (47%)) described that the providers welcome them moderately, followed by good friendly welcoming (Figure 4).
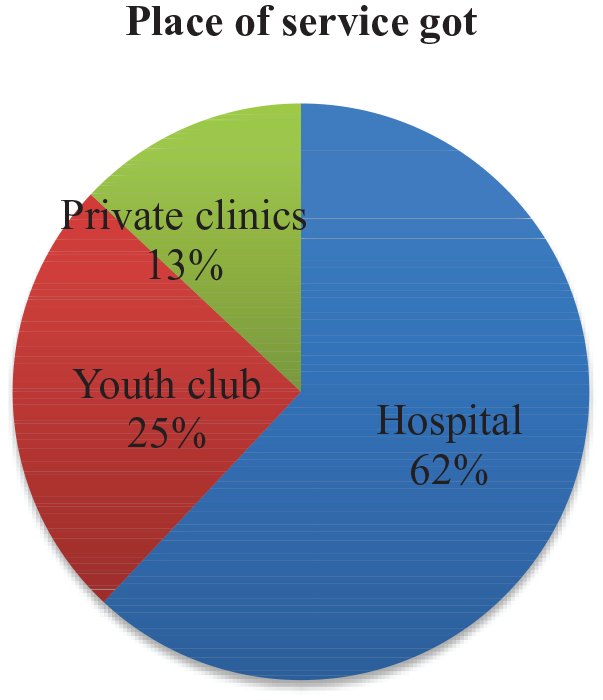
Health institutions that respondents received service in Aleta Wondo town, Sidama regional state, Ethiopia, 2020.
Among those participants who did not utilize the services, 163 (57.5%) of the respondents reported that the reason not to use YFRHS was “Have no encountered the problem,” followed by 17.6% who said, “don’t have SRHS information.” A majority of them (196 (69%)) responded more than one reason why they didn’t use the services (Figure 5).

Reason not to be used youth-friendly sexual and reproductive health service by youth in Aleta Wondo town, Sidama regional state, Ethiopia, 2020.
Among the respondents, only 140 (33.2%) had ever visited YFS facility but missed the service they required. Among the respondents, those who had sexual partners were 192 (45.6%).
Factors associated with YFS utilization
On multivariable analysis, the respondents’ gender, current living place of respondents, have ever discussed with parents, have ever visited facility but missed service required, and have sexual partner were found to be statistically significant to youth-friendly sexual and reproductive service utilization.
Females were 2 times more likely to use YFS than male counterparts (AOR = 2.20, 95% CI = 1.34–3.62). Participants who currently lived alone were relatively 3 times more likely to utilize YFRHSs than those who currently live with their family, boy/girlfriends, and husband/wife (AOR = 2.99, 95% CI = 1.48–5.77).
The respondents who had not ever discussed with their parents were 54% times less likely to utilize YFRHS utilization than those who had ever discussed with their parents (AOR = 0.46, 95% CI = 0.27–0.81). The respondents who had ever visited the facility but missed the services they required were relatively 2 times less likely to utilize YFRHS than their counterparts (AOR = 1.96, 95% CI = 1.14–3.24). The respondents who had sexual partners were 4 times more likely to use YFRHSs than their counterparts (AOR = 4.52, 95% CI = 2.75–7.4262) (Table 3).
Bivariate and multivariate analysis of factors affecting youth-friendly sexual and reproductive service utilization among youth in Aleta Wondo town, Sidama regional state, Ethiopia 2020.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; YFS: youth-friendly service; RH: reproductive health.
Discussion
This study was conducted to determine YFS utilization and associated factors among youth in Aleta Wondo town, southern Ethiopia, 2020. The utilization of YFS in the study area was 32.8%. This finding is also lower than the community-based study conducted in Mandalay City, Myanmar (67%) and an institutional-based study done in Ghana (55.8%) and Nigeria (51%). The difference in result may be due to the socioeconomic, infrastructure, availability, and accessibility of health facilities, urban–rural residence, and transportation differences among these countries with this study area which can influence the health delivery system.17–19
This finding was lower compared with the similar studies conducted in Bale zone (46%), Awabel district in Amhara Region (41%), Mareka district in Dawuro zone (69.7%), Hadiya zone (38.5%), Goba town (71.4%), Mekelle (69.1%), and Harare (64%).6,20–24 This difference might be due to the availability and accessibility of youth-friendly RH facilities or the availability of youth centers, parenting situations, and individual/personal characteristics of the study participants.
But it was higher compared with the study conducted in Nekemte town (21.2%) and Machakel District, East Gojjam, Amhara Region (21.5%).12,25 This variation might be due to the difference in sociocultural factors and openness of the study participants between these two study areas and periods of the study conducted. This finding is in line with the studies conducted in Debre Berhan town (33.8%), Albuko Woreda South Wolo zone, Amhara region (34%), Badawacho district, Hadiya zone (29.4%), and Bahr Dar town (32%).13,26–28 This might be due to individual/personal characteristics of the study participants and age similarities.
The commonly utilized SRH service component in this study was voluntary testing and counseling service (59.4%) which is almost similar to the findings of studies done in Goba town, Nekemte town, and Gondar town.12,23,29 Condom services, family planning, information on SRH issues, pregnancy test, and STI services were also commonly received by 55.7%, 51.4%, 45.6%, 42%, and 37.6% of the SRH service seekers, respectively.
The main source of information in this study was friends/peers (42%). This finding somewhat goes in line with a study at Hadiya zone (54%). 22 On the contrary, health provider was the main source of information in a study of Machakel district, East Gojjam zone (80.4%). 30 This disparity may be explained by the setting in which the studies were conducted.
The reason for not to utilize YFS for the respondents was “Have no encountered problem” (20%). This finding somewhat goes in line with the study conducted in Metekel zone, northern Ethiopia (31%). 31
In this study, females were 2 times more likely to utilize YFRHSs than males and this finding was supported by a study done in Badwachew woreda in Hadiya zone, Mekelle town, Gondar town, and Metekel zone, northern Ethiopia.6,27,29,31 This could be due to females’ fear of risk of unintended pregnancy, abortion, STI, and HIV/AIDS than males which might increase the likelihood of RH service utilization. On the contrary to this finding, males were more likely to utilize RH services than females in the study from Machakel district, Amhara region, and Nigeria.19,25
Youth who weren’t co-resided with both their parents were 2.99 times more likely to use RH services than those who live together with their parents. This finding is supported by a study conducted in Debre Berhan town. 13 But it is against the study conducted in Gondar town where adolescents/youth living with both of their parents together use VCT service more likely than their counterparts. 29 This could be due to relatively high parental monitoring in our setting. In addition to this, even though a majority of the respondents in this study were living with both their parents, the families’ habit of communication on sexual and reproductive issues was quite low (33.2%).
In this study, the respondents who had sexual partners were almost 5 times more likely to use YFRHSs than their counter parts. This finding is supported by the study conducted in Gonder town, Amhara region. 29
The respondents who had not ever discussed with their parents were 54% times less likely to utilize YFRHSs than those who had ever discussed with their parents. This finding is consistent with the study done in Jimma town. 32 This might be due to discussion about RH issues might provide access to information about RH services.
In this study, it was found that those respondents who had ever visited the facility but missed the service they required were relatively 2 times less likely to utilize YFRHSs than their counterparts. This finding is supported by the study conducted in Nekemte town, Oromia region, and Hadiya zone, southern Ethiopia.12,22
The limitation of this study was that it examined personal and sensitive issues, so obtaining honest responses among youth might have been difficult. Therefore, these data might have been prone to response bias. The quantitative study design did not allow for probing into certain areas which needed further qualitative description. In addition, measurement of some variables like provider welcoming of youths was a limitation of this study.
Conclusion
This study had showed that low proportion of the youths visited different health facilities to utilize SRH services in the last 12 months. The most frequently utilized SRH service component was voluntary testing and counseling service, followed by condoms, family planning, and information, and counseling on SRH issues. Friends/peers were the potential sources of information on SRH services for youths, followed by health professionals and youth club. Being female, living arrangements, discussing RH issues with parents, and having sexual partners were independent factors affecting utilization of YFSs. It is better to strengthen youth clubs and expand SRH services in order to meet the RH need of youths.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221088089 – Supplemental material for Utilization of youth-friendly reproductive health service and associated factors among youth in Aleta Wondo town, southern Ethiopia, 2020
Supplemental material, sj-docx-1-smo-10.1177_20503121221088089 for Utilization of youth-friendly reproductive health service and associated factors among youth in Aleta Wondo town, southern Ethiopia, 2020 by Elias Amaje, Eyasu Daniel, Kebede Tefera and Nurye Sirage in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our heartfelt appreciation to the Aleta Wondo town health office, data collectors, supervisors, and study subjects.
Author contributions
E.D. and E.A. conceived and designed the study, supervised the data collection, performed the analysis and interpretation of data, and drafted the manuscript. E.D., E.A., and K.T. assisted in designing the study and in data interpretation, and critically reviewed the manuscript. E.A. and N.S. assisted in data interpretation and reviewed the manuscript critically. All authors read and approved the final manuscript.
Availability of data and material
For those who are interested; the data sets of this study could be accessed from the ‘responding author on reasonable request.
Ethical approval
Ethical approval for this study was obtained from Pharma College Hawassa Campus Institutional Review Board (PC-HC/075/2020).
Participant consent
Participant consent was obtained.
Informed consent
The study protocol was approved by the Institutional Review Board of Pharma College Hawassa Campus. Based on the approval, an official letter of support was written by Pharma College to Aleta Wondo town health office. At last, data were collected after assuring the confidentiality of responses and obtaining informed verbal consent from the study participant. The main reason for obtaining informed verbal consent was variation in educational status of study participant and it was approved by Institutional Review Board of Pharma College Hawassa Campus. Written informed consent was obtained from the legally authorized representatives of subjects that were minor.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.