
Abstract
Objective:
We compared mental health service utilization among older, depressed Veterans (60 years or older) with and without coexisting dementia.
Methods:
This retrospective study examined data from the 2010 Veterans Health Administration National Patient Care Database outpatient treatment files of Veterans with a newly recognized diagnosis of depression (N = 177,710).
Results:
Approximately 48.84% with coexisting depression and dementia and 32.00% with depression only received mental health services within 12 months of diagnosis (p < .0001). Veterans with coexisting depression and dementia were more likely to receive medication-management appointments (33.40% vs 20.62%), individual therapy (13.39% vs 10.91%), and family therapy (3.77% vs 1.19%) than depressed Veterans without dementia.
Conclusion:
In general, Veterans with recently diagnosed depression are significantly underusing Veterans Affairs mental health treatment services. Those Veterans who have comorbid dementia are more likely than those with just depression to be enrolled in mental health treatments. Systemic improvements are needed to increase use of mental health services for older, depressed Veterans.
Depression and dementia are both common mental health conditions in older adults. Older adults aged 65 years and above have an 8% lifetime prevalence of major depressive disorder 1 and an 11% prevalence of Alzheimer’s disease. 2 Depression is also one of the most common neuropsychiatric comorbidities for persons with dementia (PWD), 3 with depression diagnosed in 20%–55% of PWD.4,5 Depression is associated with additional clinical, economic, and health-care burden for PWD. For example, coexisting depression is a risk factor for morbidity, 6 mortality, 7 and premature institutionalization of PWD. 8
Despite the existence of effective treatment for late-life depression, 9 only about 30% of older adults with mood and anxiety disorders seek mental health services. 10 Co-occurring depression and dementia makes treatment planning more complicated because of the limited availability of well-established treatment guidelines. Antidepressant medication is a common treatment practice, 11 despite meta-analytic evidence suggesting little to no benefits in PWD.12,13 However, reviews have shown psychological interventions to be effective at reducing depressive symptoms in PWD.14,15 These findings indicate that depression in PWD is treatable; yet, little is known about the rates at which older adults with comorbid depression and dementia are using nonpharmacologic treatments.
A prospective, small-scale (N = 99) study by Kunik et al. 16 examined the longitudinal relationship between health-care service utilization and treatable comorbid conditions (pain, aggression, depression, and psychosis) among Veterans with dementia. The researchers found that coexisting depression significantly contributed to the use of outpatient psychiatric services. 16 This study hopes to expand on this study by using a large national dataset, examining utilization rates of different modalities of outpatient psychiatric treatment, and comparing mental health utilization rates of Veterans with comorbid depression and dementia to Veterans with depression only. Conducting such comparisons will allow researchers to explore the additive effect of dementia on mental health service utilization.
The aim of this study was to better understand differences in mental health service utilization (medication management and psychotherapy sessions) between depressed older Veterans with and without dementia. Given the clinical and neuropsychiatric complexities associated with comorbid depression and dementia, it was hypothesized that comorbid dementia and depression would be associated with decreased mental health service utilization (i.e. lower rates of medication management, individual psychotherapy, group therapy, and family therapy) relative to depressed Veterans without dementia.
Method
A retrospective Veterans Health Administration database was chosen for this study because it is a unique, large data source that stores information on mental and physical health characteristics. Data for older Veterans (60 years or older) receiving care during the 2010 fiscal year (FY10, 1 October 2009–30 September 2010) were collected from the outpatient treatment files of the National Patient Care Database. We chose to use FY10 data for this study because it was the most recent data file available. This database contains encrypted patient identifiers linked to broad patient and service characteristics, including mental health services, and the Veterans Affairs (VA) Information Resource Center 17 monitors the accuracy and validity of its information. This study was approved by the Institutional Review Board at Baylor College of Medicine and the Research and Development Committee at the Houston VA Medical Center.
Patient population
This study focused on Veterans with a newly recognized depression diagnosis, identified using the International Classification of Diseases—Ninth Edition—Clinician Modification (ICD-9-CM codes: 293.83, 296.20–296.36, 300.4, and 311). A condition was defined as newly recognized when there had been no related diagnosis recognized in the 6 months immediately preceding the index date (the date of first diagnosis during the study period). The cohort was restricted to newly recognized depression to standardize the extracted cohort and ensure mental health utilization was not under-counted. Veterans with a coexisting dementia diagnosis at the index date were identified, using the following dementia ICD-9-CM codes: 046.1x, 046.3, 290.xx, 291.2, 292.82, 294.1x, 294.8, 331.xx, and 333.x. To ensure Veterans had adequate opportunity to access outpatient mental health services, Veterans that had 60 or more inpatient days in the 180 days following depression diagnosis were excluded from the sample.
Patient characteristics
Patient characteristics included age, gender, race, marital status, yearly income, distance to the nearest VA medical center, VA service-connected disability, receipt (yes/no) of medical or psychiatric inpatient hospitalization, and receipt (yes/no) of outpatient medical services. Yearly income was estimated, using the average adjusted gross income for each Veteran’s zip code, which was based on 2008 Internal Revenue Service data. In addition, the distance to the nearest VA medical facility (in miles) was calculated, using the Veteran’s zip code. Because of the increased access to care provided to Veterans with service-related disabilities, Veterans were categorized into disability groups, including 0%, 1%–49%, and 50%+. Additionally, outpatient diagnoses for a variety of medical conditions were used to calculate a Charlson Comorbidity Index score, 18 with higher scores indicating greater global illness severity. Excluding the presence of depression and dementia, researchers also calculated the average number of comorbid mental health diagnoses (e.g. posttraumatic stress disorder, substance abuse, anxiety, personality disorders, and bipolar disorder). Outpatient health service use included the number of patients who received medicine/primary care, surgical, urgent care, and ancillary/other services.
Mental health services
Current Procedural Terminology (CPT) codes were used to categorize mental health services into the following groups: medication management (CPT codes: 90805, 90807, 90809, 90811, 90813, 90815, and 90862), individual psychotherapy (CPT codes: 90804, 90806, 90808, 90810, 90812, 90814, 90845, 90875, 90876, and 96152), family therapy (CPT codes: 90846, 90847, 96154, and 96155), and group therapy (CPT codes: 90849, 90853, 90857, and 96153).
Deriving the analytic sample
All Veterans with coexisting depression and dementia were included in the sample, whereas a 2:1 ratio was used to randomly select age-matched depressed Veterans without dementia. A 2:1 ratio allowed us to control for age without consequence to power or scientific control. For example, Dumville et al. 19 reported that the use of unequal patient groups reduces power only if the ratio is 3:1 or more.
Statistical analyses
Analyses were conducted using Statistical Analysis System (SAS) version 9.2 (SAS Institute, Inc., Cary, NC). Analyses of variance (ANOVA) and chi-square tests were used to identify any significant differences in demographics between depressed Veterans with and without coexisting dementia. Descriptive analyses examined the proportion of depressed Veterans with and without dementia using mental health services for each treatment type during the 12 months following each Veteran’s index date. Due to the large number of analyses, a more stringent p value (p < .01) than usual was chosen to determine significance.
Results
The final cohort comprised 177,710 older Veterans with a newly recognized diagnosis of depression in FY10 (n = 8258 with coexisting depression and dementia and n = 16,516 with depressed Veterans without dementia). Due to implementation of a 2:1 age-matching ratio, a total of 152,936 depressed Veterans without dementia were excluded from the analyses. Table 1 presents the demographic and clinical characteristics for the combined cohort, as well as separately, for depressed Veterans with and without comorbid dementia. The full sample was, largely, men who were White, married, and had an average age of 79.03 years (standard deviation (SD) = 7.99). Results revealed that depressed Veterans with dementia, compared with those without dementia, were more likely to have received inpatient medical and psychiatric services, to have undergone neuropsychological testing and assessment interviews, and to have received outpatient urgent care. Depressed Veterans with dementia were less likely to be VA service-connected, to have a coexisting anxiety disorder, and to have received outpatient medicine/primary care, surgical services, and other/ancillary medical services than depressed Veterans without dementia. In addition, depressed Veterans with dementia were more likely to be Black and married than depressed Veterans without dementia.
Demographic and clinical characteristics of depressed older Veterans without and with comorbid dementia.

VA = Veterans Administration; PTSD = posttraumatic stress disorder; SD: standard deviation.
2:1 matched pairs design was used to randomly select pairs of subjects matched on age.
Not married includes divorced, never married/single, separated, and widowed.
Unknown includes missing or unknown race data.
Mental health service utilization
Table 2 presents mental health service utilization for the sample during the 12-month follow-up period. Less than half of Veterans with coexisting depression and dementia (48.84%) and even fewer with depression only (32.00%) received mental health services within 12 months of diagnosis (p < .0001). Veterans with depression and dementia were more likely to receive medication-management appointments (33.40% vs 20.62%), individual therapy (13.39% vs 10.91%), and family therapy (3.77% vs 1.19%) than depressed Veterans without dementia (p < .0001 for all comparisons). Although depressed Veterans without dementia (1.96%) used group therapy more often than depressed Veterans with dementia (1.57%), this finding was not significant (p = .03). Overall, depressed Veterans with and without dementia received medication management more often than psychotherapy services. When depressed Veterans with and without dementia sought psychotherapy, individual therapy was the most commonly used modality.
Mental health service utilization over the 12-month follow-up period.
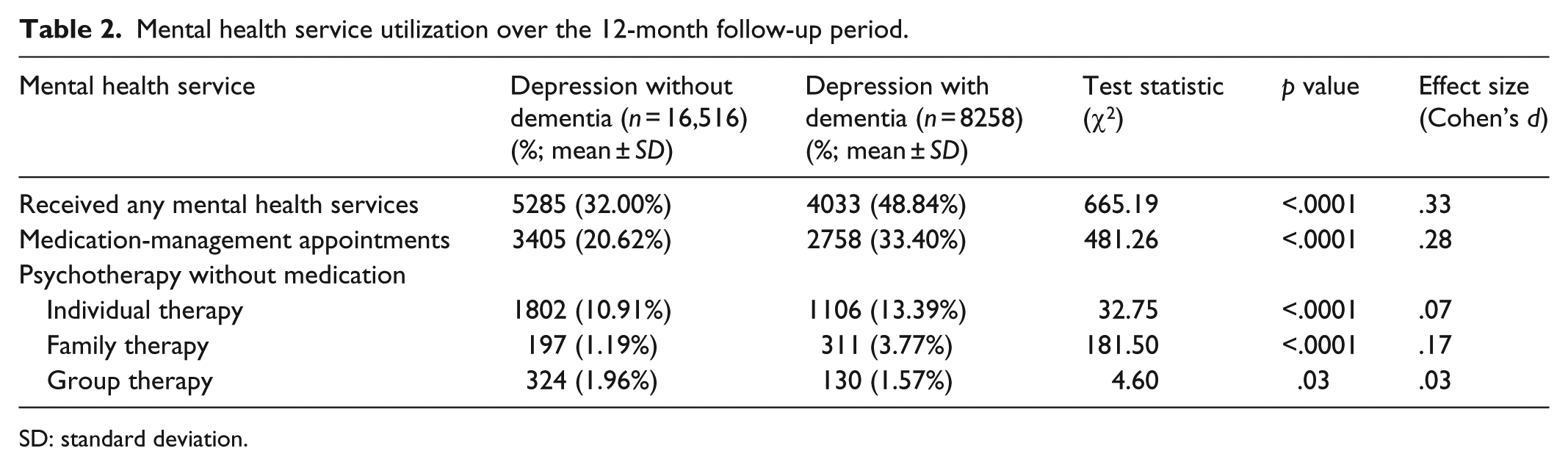
SD: standard deviation.
The frequency with which these two groups received mental health services also was examined. Depressed Veterans with dementia had more medication-management appointments (2.79 ± 1.89 visits vs 2.66 ± 1.83 visits) and family therapy sessions (2.48 ± 2.17 visits vs 2.27 ± 1.96 visits) during the follow-up period and fewer number of individual (2.42 ± 2.13 vs 2.66 ± 2.28 visits) and group therapy sessions (4.01 ± 3.02 vs 4.72 ± 2.98 visits) than Veterans with depression only.
Discussion
Contrary to our hypothesis, this study found that Veterans with coexisting depression and dementia are more likely to receive any mental-health-care services (medication-management appointments or psychotherapy without medication) than depressed Veterans without dementia. Despite the added complications that cognitive impairments may bring to treatment, providers are delivering services to Veterans with coexisting depression and dementia. As found in prior studies, 20 a significant number of newly diagnosed depressed Veterans with and without dementia are still not receiving specialty mental health services. It is notable that this study did not directly examine rates of antidepressant medication use which could have been provided by primary care or other nonmental-health providers.
There are many factors that likely contribute to less than half of Veterans with newly diagnosed depression, whether or not they have dementia, from receiving mental health services. Even though the design of this study did not allow for the identification of contributory factors, we offer the following speculations. Veterans may have difficulty accessing mental health care due to delays in mental health appointments and other difficulties with linkage to care (e.g. complicated referral mechanisms). Moreover, our sample of older adults have their own unique barriers to receiving mental health care, such as concerns about the cost of treatment, lack of transportation or difficulty traveling, low confidence about treatment outcomes, stigma associated with mental illness, and limited knowledge about mental health services and resources.21–23
Exploratory findings also revealed differences in the frequency of which mental health services are being delivered to Veterans with coexisting depression and dementia and depressed Veterans without dementia. For instance, Veterans with coexisting depression and dementia had fewer number of group therapy visits than depressed Veterans without dementia. Therapy for individuals with cognitive impairments in a group setting is highly specialized and, therefore, likely not widely accessible. In addition, therapists may be hesitant to refer depressed Veterans with dementia to group therapy because of difficulties in tailoring treatment content to individual needs, such as modifying treatment pace to account for cognitive slowing. In comparison with depressed Veterans without dementia, Veterans with coexisting depression and dementia received a greater number of medication-management appointments and family therapy sessions, as well as received more inpatient medical psychiatric services, neurological testing, and assessment interviews. Furthermore, with the exception of urgent care services, depressed Veterans without dementia were more likely to have received outpatient medical services than depressed Veterans with dementia. Finally, Veterans with dementia, depression, and comorbid chronic or severe medical conditions (e.g. congestive heart failure, chronic lung conditions, etc.) often receive even greater services than Veterans without chronic medical conditions, suggesting that increased attention to health-care needs may translate into increased service use more broadly within the health-care system.
Study limitations
Several considerations and limitations should be noted: (1) the cross-sectional nature of the study precluded inference of causal relationships; (2) the study was limited to VA databases and does not examine use of non-VA care; (3) database information is based upon individual provider coding and diagnostic accuracy; (4) data describing treatment/patient outcome (e.g. depression scores, death records, etc.), patient preferences for care (e.g. treatment refusals), and timing of dementia or severity of cognitive declines were not available; and (5) quality and type of pharmacotherapy were not formally assessed, and psychotropic medications provided by nonmental-health providers (e.g. primary care) were not included in the study.
Future research
Given the frequency of medication use in Veterans with coexisting depression and dementia, future studies should continue to evaluate the quality of pharmacotherapy, such as examining how many patients receive a guideline-concordant dose. Moreover, research should explore predictors of mental health services use as well as moderators of response to psychotherapy and/or pharmacotherapy in Veterans with coexisting depression and dementia. It would also be informative for future research to identify provider characteristics (e.g. occupation, presence of geriatric mental health training, etc.) of those delivering mental health services to Veterans with coexisting depression and dementia.
Conclusion
Even though both groups are underusing mental health services, Veterans with late-life depression, with (~49%) or without dementia (32%), are more likely to get care than their civilian peers (30% reported seeing a specialty mental health provider or general medical provider for “emotional problems”). 10 Moreover, Veterans with coexisting depression and dementia are receiving mental health services more than Veterans with depression only. Providers’ willingness and attempts to provide care to Veterans with coexisting depression and dementia may be a reflection of continued national and VA initiatives focused on improving mental health care. Moving forward, it will be important to understand reasons for underutilization of mental health treatment in depressed older Veterans with and without dementia, which might facilitate development of solutions to increase referral to and use of mental health services.
Footnotes
Acknowledgements
The authors would like to thank Sonora Hudson, MA, for editorial assistance with this manuscript.
Declaration of conflicting interest
The attitudes expressed are those of the authors and do not necessarily reflect those of the Department of Veterans Affairs, US government, or Baylor College of Medicine.
Funding
This work was partially supported by the resources and facilities of the Houston VA HSR&D Center for Innovations in Quality, Effectiveness and Safety (CIN13-413).