
Abstract
Objective:
Maternal colonization or infection with drug-resistant Group B streptococcus is a serious disease that affects mother, fetus, and infant. The knowledge of maternal colonization and antimicrobial susceptibility test is substantially needed for a nation to formulate a policy or change the already existing one to reduce maternal, fetus, and infant mortality. As a result, the goal of this review was to determine the pooled prevalence Group B streptococcus colonization and antimicrobial susceptibility among Ethiopian pregnant women.
Methods:
Literature searches were carried out in the electronic biomedical databases and indexing services such as PubMed/MEDLINE, Scopus, Science Direct, Web of Science, and Google Scholar. Original records of research articles, available online from 2014 to December 2020, addressing prevalence and antimicrobial-resistance pattern of Group B streptococcus in pregnant women were identified and screened. Endnote citation manager software version X9 for windows was utilized to collect and organize search outcomes and for removal of duplicate articles. The relevant data were extracted from included studies using a format prepared in Microsoft Excel and exported to STATA 14.0 software for the outcome measures analyses and subgrouping. The I2 index was used to measure heterogeneity between studies and median, and interquartile (25%, 75%) was used to assess antimicrobial susceptibility rate.
Results and conclusion:
Sixteen original articles were found in both qualitative and quantitative analyses. Group B streptococcus colonization was recorded in 979 of the 5743 pregnant women, resulting in a 16% overall frequency (95% confidence interval: 13%−20%). The estimated prevalence varied significantly between studies with significant heterogeneity (χ2 = 154.31, p = 0.001, I2 = 90.28). Ampicillin (97.8%; interquartile range = 89.5%−100%), penicillin G (95.5%; interquartile range = 89.5%−100%), and vancomycin (100%; interquartile range = 89.5%−100%) susceptibility were all high in Group B streptococcus, whereas tetracycline (29%; interquartile range = 89.5%−100%) susceptibility was low. Group B streptococcus colonization rates in Ethiopian women during pregnancy were virtually similar to those in many underdeveloped countries, and Group B streptococcus isolates were highly sensitive to ampicillin, penicillin G, and vancomycin.
Introduction
Within the genus Streptococcus, Group B streptococcus (GBS) or Streptococcus agalactiae is one of numerous serologically different species. 1 It is an encapsulated diplococcus exhibiting ß-hemolysis on blood agar, facultative anaerobe, nutritionally fastidious, catalase, and mannitol salt negative. 2 Recognized by Lancefield classification as GBS in the 1930s and classified into 9 serotypes, a 10th serotype of it was recently identified. 3 GBS is a leading cause of serious infection and sepsis in both mothers and babies. Chorioamnionitis, endometritis, and urinary tract infections are among the maternal diseases linked to GBS. 4 GBS colonizes the vaginal and rectum of 10%−30% of pregnant women, and it is predicted that 50% of newborns will be colonized if exposed to GBS during delivery, with just 2% developing an invasive infection. 5 Every year, GBS causes between 114,000 and 204,000 invasive cases, as well as 147,000 stillbirths and infant deaths across the world. 6 Neonatal death rates in industrialized and poor nations, respectively, range from 10% to 15% and 40% to 58%, demonstrating that vertical transmission of S. agalactiae remains a global issue. 3 Infection with GBS causes sepsis and meningitis in newborns, which can lead to severe sickness, long-term disability, and death. 1
The Center for Diseases Control (CDC) suggests two approaches for preventing GBS infection in newborns. Between 35 and 37 weeks of pregnancy, all pregnant women were tested for vaginal and rectal GBS colonization using a culture-based screening technique. 7 The alternative method is risk-based, which comprises identified candidates for intra-partum chemoprophylaxis based on the presence of any of the following intra-partum risk factors, and intra-partum antibiotics are suggested for those with positive culture results 8 : intra-partum fever of 38° centigrade, membrane rupture in 18 h, and birth at less than 37 weeks. Risk-based screening is utilized in areas where culture-based screening is not accessible, and it is most commonly employed in low-resource settings. Chemoprophylaxis is still the most efficient way to prevent infections in mothers and babies. 8 The antibiotics of choice for GBS prophylaxis include penicillin, ampicillin, erythromycin, and clindamycin. 8 However, reports of medication resistance have made susceptibility testing a crucial part of the GBS management approach.8,9 Ethiopia is a developing nation with a high newborn mortality rate of 33 per 1000 live births, accounting for 52% of under-5 mortality and 30% of neonatal death due to infection or sepsis. 10 Despite significant newborn mortality owing to infection, regular culture-based screening is not implemented as a national policy in Ethiopia.
Furthermore, several researches have been done in various parts of the country, albeit in a disjointed manner. As a result, the goal of this review is to aggregate and comprehensively report the prevalence of GBS colonization based on culture-based approach and antibiotic susceptibility testing, so that the data may aid future national protocol formulation for GBS screening.11,12
Methods
The PRISMA 20 (Preferred Reporting Items for Systematic Reviews and Meta-analysis) standard was used to conduct these systematic reviews and meta-analyses. 13
Search strategy
A literature search of PubMed/Medline, Science Direct, Scopus, Web Science, and Google scholar databases was identified for potentially relevant papers. GBS, streptococcus agalactiae, streptococci, group B streptococcus, vagina colonization, Ethiopia, prevalence, proportion, antibiotic, antimicrobial resistance, and antimicrobial sensitivity test were all searched using a mix of free text and thesaurus phrases. The following key phrases were combined using “AND” and “OR” Boolean operators to obtain research from an Internet database. Pregnancy AND Ethiopia AND GBS, GBS AND Ethiopia, Pregnancy AND Ethiopia AND group B streptococcus, pregnancy AND group B streptococcus AND Ethiopia, pregnancy AND streptococcus agalactiae AND Ethiopia, antibiotic susceptibility OR antibiotic resistance AND GBS OR streptococcus agalactiae AND Ethiopia. To find the relevant original papers in PubMed, we employed medical topic headings (MeSH words). Three authors (D.L., T.K., and L.C.H.) conducted the search and the most relevant papers were chosen based on established inclusion and exclusion criteria. The final author double-checked the consistency of the search method, research selection, and inclusion and exclusion criteria.
Inclusion and exclusion criteria
We included published and unpublished (Addis Ababa Universities) studies that reported the prevalence of GBS colonization and their antimicrobial-resistance from inception to July 2021 in pregnant women. We also included studies published in English, human studies, and conducted only in Ethiopia. We excluded qualitative studies, review paper, commentaries, case series, case reports, conference proceeding, and abstracts.
Data extraction
Data abstraction was conducted by two authors (D.L., T.K.) utilizing an Excel spreadsheet form. Using inclusion criteria, the two authors separately assessed titles, abstracts, full-text publications, and abstracted data. Discrepancies between the two authors who largely abstracted the data were arbitrated by the third author (L.C.H.). The following parameters were extracted from each study: the name of the first author, year of publication, study sites (regions), age, the specimen collection site, gestational age, the number of pregnant women who participated in the study, the number of moms positive for GBS, the prevalence/proportion, and the antibiotic susceptibility test.
Methodology quality assessment
The assessment of methodological quality was carried out independently by two reviewers using the Newcastle-Ottawa scale (NOS). A quality scale was calculated based on three categories.
Selection (maximum 4 stars);
Comparability between groups (maximum 2 starts);
Outcome assessment (maximum 3 stars). A maximum of 1 star could be awarded for each item in the group selection and outcome assessment categories. A maximum of 2 stars could be awarded for comparability. Therefore, the maximum possible score was 9 stars, which represented the highest methodological quality. Studies were labeled as having high quality if the score was above the average (8 stars). Disagreements between the reviewers were resolved through discussion.
Statistical analysis
Endnote citation manager software version X9 for windows was utilized to collect and organize search outcomes and for removal of duplicate articles. The relevant data were extracted from included studies using a format prepared in Microsoft Excel and exported to STATA 14.0 software for the outcome measures analyses and subgrouping. To give a visual summary of the data, we utilized forest plots to estimate the pooled effect size and effect of each research along with their confidence interval (CI). Because of the expected heterogeneity, a random-effect model was utilized in this meta-analysis. The p value, Cochrane test (Q-test), and I 2 were used to represent statistical heterogeneity among studies, with p value of 0.05 and I 2 values of 0%, 25%, 50%, and 75% indicating no, low, moderate, and high heterogeneity, respectively. For a quantitative examination of the likelihood of publication bias, we utilized Egger’s regression test as well as visual inspection for symmetry of the plot. We also did subgroup analysis using publication years, sample size, and study location as covariate. If p < 0.05, all stated p values were two-sided and statistically significant.
Result
Literature identification and descriptions of studies
After evaluating the titles and abstracts of the 312 studies found, 156 duplicates were removed. We also omitted 110 publications since they did not mention the prevalence of GBS in Ethiopia. Finally, the entire text of the remaining 46 papers was downloaded and thoroughly examined to ensure that they met all of the inclusion requirements. We also removed 15 publications because they were not about GBS colonization during pregnancy in Ethiopia, and 15 more studies because they were not about GBS prevalence during pregnancy. Finally 16 articles full filling inclusion criteria were included in this review9,14–27(Figure 1).
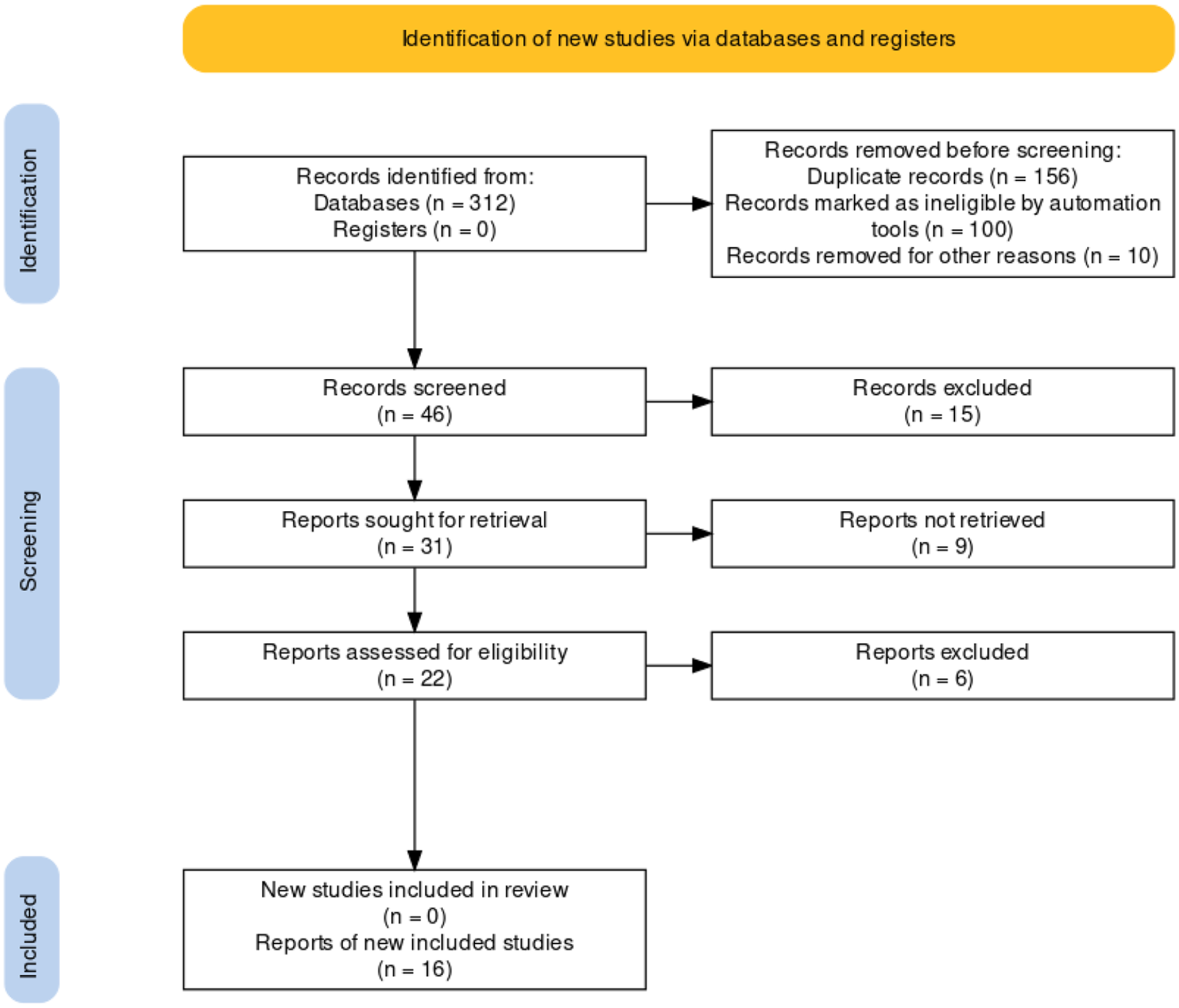
PRISMA flow diagram for study selection.
All studies were facility-based cross-sectional. The age of included pregnant women ranged from 14 21 to 40 years.15,21,27–29 Twelve of the studies reported antimicrobial susceptibility test,9,15–18,20–22,25,27,29,30 nine of them used the Kirby–Bauer disk diffusion method for susceptibility test,9,20–22,25,27,29,30 and one used Agar diffusion technique. 17 Only three of the studies reported Serotype of GBS isolates and three of them reported type II most common followed by type V.23,26,27 Sample size of included studies ranged from 126 to 1688.9,14–27 and the prevalence of GBS during pregnancy ranged from 7.2% to 26.8%.14,17 Five minimum antibiotics used for susceptibility test and 12 maximum antibiotics for susceptibility test were used.9,15–18,20–22,25,27,29,30 Year of publication was from October 20149,26 to January 202020,24,26,27,29,30 and there were five studies from Oromia region,16,17,20,24,26 four studies from Addis Ababa city administration,9,22,27,29 three studies from SNNP region,15,23,28 two from Tigray region,21,25 and one each from Amhara 18 and Harari regions. 14 No study reported from Somalia, Afar, Gambella regions, Dire Dawa city administration and Benishangul-gumuz region. Twelve studies reported as sample were taken from Recto-vaginal,15–18,25,27,29,30 three studies from lower vagina alone,17,22,25 and one study from anal and vagina. 21 Five studies did not report the gestational age14,24,23,26,27 while eight studies reported that the sample was taken at gestational age 35–37 weeks and one study reported a gestational age of 37–40 weeks. 29 Most of the studies were of high quality, but few were of low quality according to the authors’ judgment (Table 1).
Characteristics of studies included in systematic review and meta-analysis.

CD: age mentioned in categorical description; NA: not available; SNNP: southern nation and nationalities peoples; GA: gestational age.
Pooled prevalence estimate and heterogeneity
In Ethiopia, the prevalence of GBS during pregnancy was reported in 16 studies including 5734 pregnant women. As shown in Figure 2, among the 979 pregnant women colonized by GBS, the pooled prevalence was estimated to be 16% (95% CI: 13%−20%). The prevalence estimate differed significantly between studies (χ2 = 154.31, p = 0.001, I 2 = 90.28) (Figure 2).

Forest plot showing pooled prevalence of GBS colonization during pregnancy in Ethiopia women, 2021.
Subgroup analysis by region
GBS colonization was found in 18% (95% CI: 11–24) of pregnant women in Oromia, 15% (95% CI: 8–21) of pregnant women in SNNP, and 17% (95% CI: 9–25) of pregnant women in Addis Ababa city administration (95% CI: 9–25) (Figure 3).

Forest plot depicting subgroup analysis by region on pooled prevalence of GBS colonization during pregnancy in Ethiopian women, 2021.
Subgroup analysis by year of publication
Before 2016, the estimated pooled prevalence of GBS colonization was 14% (95% CI: 9–19), and between 2017 and 2020, the estimated pooled prevalence of GBS colonization was 18% (95% CI: 14–21), with no significant difference between groups (p = 0.274), (Figure 4).
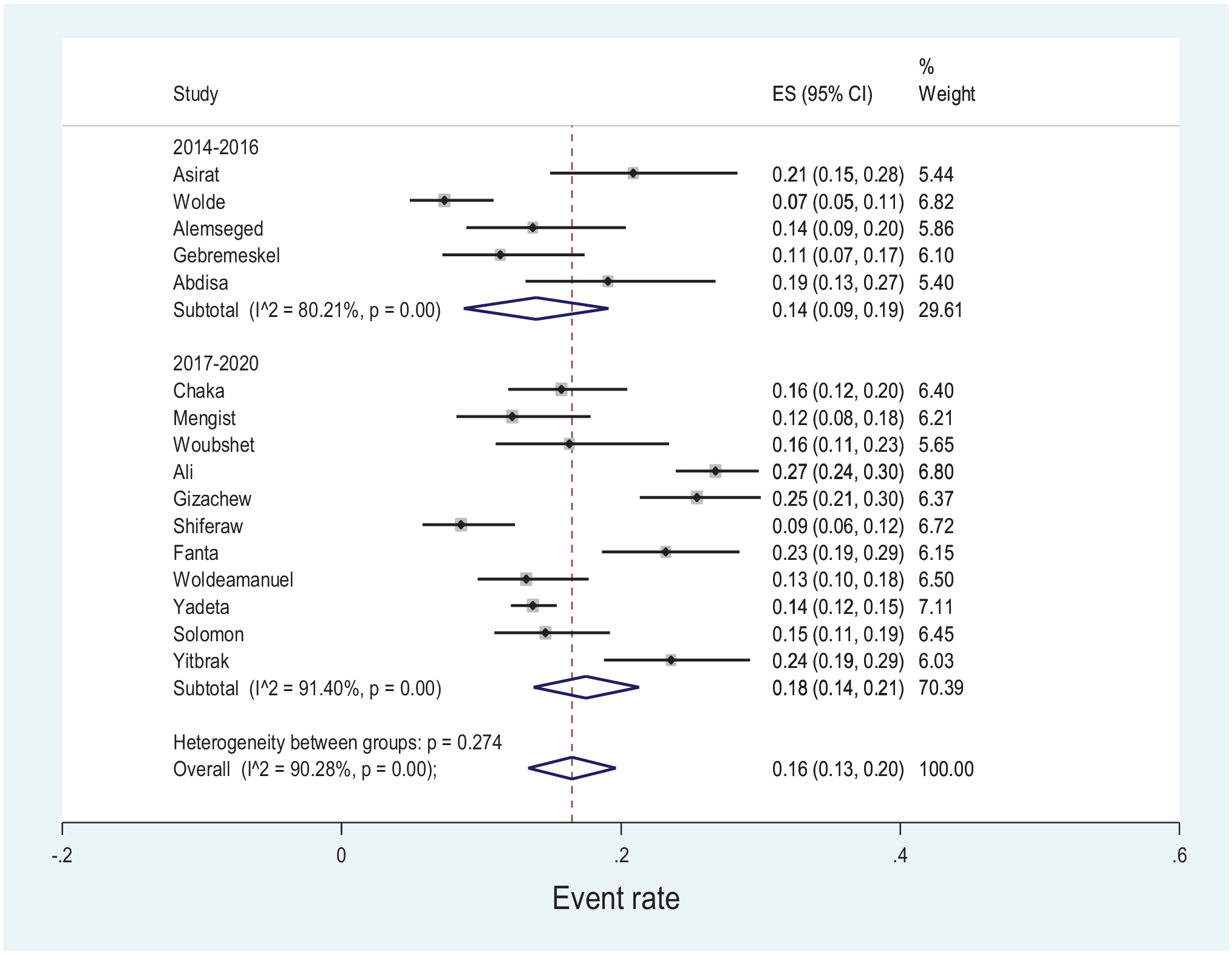
Forest plot depicting subgroup analysis by year of publication on pooled prevalence of GBS colonization during pregnancy in Ethiopian women, 2021.
Subgroup analysis by site of sample taken
In our study, we discovered that those studies that took samples from the recto-vaginal had a higher prevalence of GBS of 18% (95% CI: 14–22) followed by samples taken from lower vagina at 14% (95% CI: 11–16) (Figure 5) (Table 2).

Forest plot depicting subgroup analysis by site of sample taken on pooled prevalence of GBS colonization during pregnancy in Ethiopian women, 2021.
Summary of prevalence of GBS colonization among pregnant women in Ethiopia, 2021.

CI: confidence interval.
Subgroup analysis by sample size
We also performed subgroup analysis by sample sizes (<200 vs. ⩾200). Accordingly, the prevalence of GBS colonization in studies with sample size <200 was 15% (95% CI: 12–18 and it was 17% (95% CI: 13–21) in studies involving sample size of 200 and above (Figure 6).

Forest plot depicting subgroup analysis by sample size on pooled prevalence of GBS colonization during pregnancy in Ethiopian women, 2021.
Publication bias assessment
The visual assessment of the asymmetry of the funnel plot revealed no publication bias, which was statistically verified by Egger’s regression test (β = 2.03, 95% CI: 2.2–6.3) p = 0.322) (Figure 7).

Assessment of publication bias.
Antimicrobial susceptibility test
Antimicrobial susceptibility tests for identified GBS isolates were reported in 12 studies. Vancomycin had the highest prevalence of susceptibility (median 100%, interquartile range (IQR) = 89.18%−100%), followed by ampicillin (median 97.75%, IQR = 89.45%−100%), while tetracycline had the lowest prevalence of susceptibility (median 29%, IQR = 13.85%−43.73% (Figure 8 and Table 3).
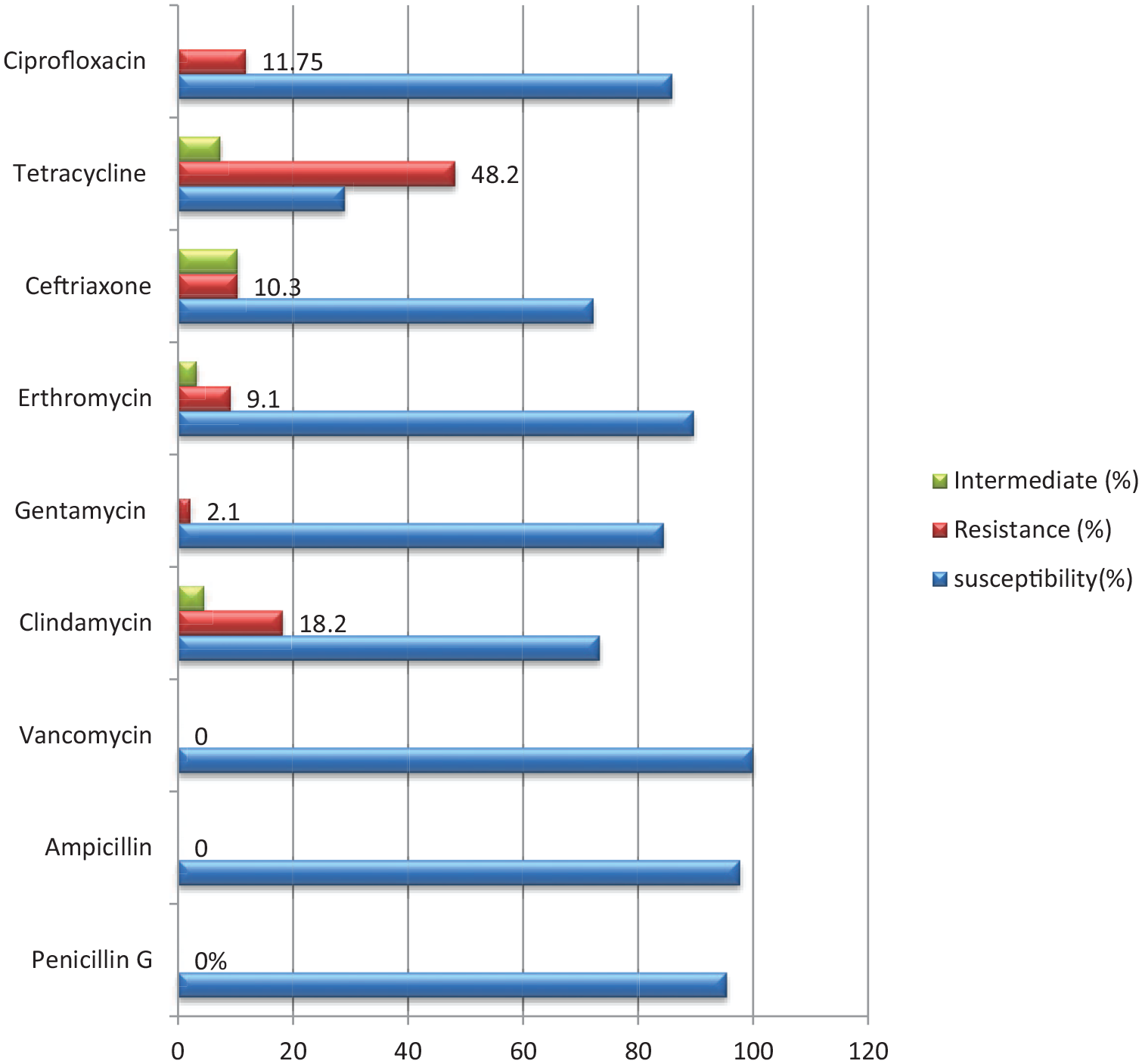
Antimicrobial susceptibility testing pattern among pregnant women of Ethiopia for those colonized by GBS, 2021.
Antibiotics susceptibility test for GBS during pregnancy among Ethiopian women, 2021.

NA: not available; NT: not tested; IQR: interquartile range; PEN: Penicillin; AMP: ampicillin; VAN: Vancomycin; CLM: Clindamycin; GEN: Gentamycin; ERY: Erythromycin; CEF: ceftriaxone; TTC: Tetracycline; CPR: Ciprofloxacin.
Discussion
In Ethiopia, the prevalence of maternal colonization with GBS, as well as antibiotic susceptibility testing, has only been studied in modest and fragmented ways thus far. As a result, this is the first meta-analysis of its sort to describe the total proportion of GBS colonization in Ethiopia during pregnancy. We looked at 16 distinct researches from 5 different areas and 1 administrative city. As a result, in this review, the pooled estimate of GBS colonization among Ethiopian pregnant women was 16%, ranging from 15% to 18% in different areas. The present meta-analysis findings are lower than those of a meta-analysis of 73,791 pregnant women from 37 different African nations, which found a 17.9% prevalence of GBS colonization. 31 Another meta-analysis of 22,206 pregnant women in Africa found a pooled prevalence of GBS colonization during pregnancy of 19.3%, which is greater than our present result. 1 Another comprehensive review and meta-analysis done in a Cameroonian tertiary hospital revealed a pooled prevalence of GBS colonization of 14%, which was lower than our data. 32 The pooled estimated prevalence of Group B Streptococcus in the vagina and rectum of pregnant women in Islamic and non-Islamic countries was 15% and 14%, respectively, according to a meta-analysis and systemic review. 33 Standards and laboratory diagnostic methods, differences in study location, differences in respondents’ residence, differences in previous obstetric history, bacteriological method for organism detection, statistical differences in the study population, laboratory staff skill, and health and medical policies of countries and geographic regions could all contribute to the disparity.
Because of a lack of qualified workers and the availability of essential materials, culture-based detection of GBS during pregnancy is seldom done in Ethiopia. In most health facilities, GBS was assessed using a risk-based method and ampicillin was given to all patients empirically. In our study, all GBS were sensitive to vancomycin, whereas ampicillin susceptibility was 97.75% and penicillin G susceptibility was 95.45%. All isolates of GBS were shown to be sensitive to ampicillin, vancomycin, and penicillin in a meta-analysis done in Cameroon. 34 A meta-analysis done in the province of China found that the majority of GBS isolates were sensitive to ampicillin, penicillin, and vancomycin, with a pooled tetracycline resistance of 73%. 5 A study conducted in Iranian pregnant women on antibiotic resistance for GBS during pregnancy justified that the tetracycline resistance rate was 96.2%, while for ampicillin and penicillin, this was less than 4%. 35
According to our review on antibiotic resistance and susceptibility to GBS, penicillin and ampicillin have been chosen for the prevention and treatment of GBS infections, and are typically given in early labor based on cultured discovered serotypes or those who meet the risk-based approach requirements. Instead of penicillin or ampicillin, erythromycin and clindamycin are given for pregnant women who are at risk of anaphylaxis. In most parts of Ethiopia, ceftriaxone is utilized as a second-line antibiotic in the absence of ampicillin or penicillin; however, in our investigation, ceftriaxone was found as intermediate to GBS resistance in about 20% of the cases.11,12 Vancomycin can be used in the case of drug resistance to ampicillin and β-lactam antibiotics, despite the fact that it is costly and not commonly accessible in Ethiopia. In leading nations, CDC-recommended instructions were followed and antibiotic prophylaxis was used, resulting in a 70% reduction in the frequency of infection in babies and newborns. 8
Strengths and limitations
To the best of our knowledge, this is the first study of its type to describe the countrywide prevalence of GBS colonization and antibiotic susceptibility testing for GBS among pregnant women in Ethiopia. It is critical to generate complete data for policymakers and other interested parties. This subject appears to be undervalued at the national level, with no real evidence-based strategy for detecting GBS colonization and prescribing sensitive antibiotics. The country’s risk-based strategy has a number of flaws, including ignoring the problem and contributing to antibiotic resistance and our review will provide a vital concept for revising the present procedure. We also wanted to know what was driving the considerable heterogeneity we noticed in our review. This review had some limitations. First, a few of the reviews did not mention the gestational age at which the sample was taken, which is important because the gestational age at which the sample was taken affects the prevalence of GBS. Second, the method for antimicrobial susceptibility in some studies was not well mentioned in their methodology. Third, because most studies were conducted in the country’s major cities, with the majority of Ethiopians living in rural areas, the prevalence of GBS may be underestimated. Finally, only a few studies included a history of antibiotic use 2–3 weeks prior to sampling for GBS, which could have a significant effect on the growth of bacteria on culture media.
Conclusion
Because the frequency of GBS identified in our study was high, screening all pregnant women for GBS at 35–37 weeks gestational age, as recommended by the CDC, is critical for reducing GBS-related maternal and newborn mortalities and morbidities. All serotypes of GBS identified in the reviews were highly sensitive to ampicillin, penicillin G, and vancomycin, according to our evaluation.
Footnotes
Author contributions
All authors made a significant contribution to the work reported, be it in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; they took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Data availability
All relevant data are available within the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Not applicable.
Informed consent
Not applicable.
Trial registration
Not registered.