Allograft procurement in the first successful combined face and bilateral hand transplant: Timing and sequence
Bruce E Gelb, Gustave K Diep, Zoe P Berman, Ricardo Rodriguez Colon, Jorge Trilles, Daniel Boczar, Bachar F Chaya and Eduardo D Rodriguez
NYU Langone Health, New York, NY, USA
Introduction: Vascularized composite allotransplantation provides a reconstructive option for patients with otherwise irreparable defects. Despite significant advances in the field, successful multi-vascularized composite allotransplantation has yet to be reported. We herein describe our experience with the first successful combined face and bilateral hand transplant, focusing on the sequence and timing of allograft procurement.
Methods: The recipient was a 22-year-old male who presented for multi-vascularized composite allotransplantation evaluation after sustaining a motor vehicle accident resulting in 80% total body surface area burns, including his full face and bilateral upper extremities. Following multidisciplinary team evaluation and institutional review board approval, he was deemed an appropriate candidate for combined face and bilateral hand transplant. In defining his expectations for the transplant, the recipient wished to prioritize recovery of hand function above all else.
Results: Combined face and bilateral hand transplant was performed over 23 h and 3 min in two adjacent operating rooms. Given the recipient’s right-hand dominance, we opted for procurement and transplantation of the right upper extremity first, followed by the left upper extremity, with the facial allograft procured last. The vascular pedicles in the donor left upper extremity allograft were only divided once vascular inflow and outflow was re-established in the right upper extremity. Similarly, the external carotid arteries were clamped and divided after the left upper extremity was reperfused. To minimize ischemia, no tourniquet was used in the donor room, while tourniquet use was limited to <2 h in the recipient room. Total ischemia times were 2 h and 30 min for the right upper extremity; 2 h and 46 min for the left upper extremity; and 2 h and 52 min for the face. Optimization of arterial inflow and venous outflow was ensured with preservation of the muscular perforators and reconstruction of both the deep and superficial venous systems. At 10 months post-transplant, the recipient is demonstrating continuous improvement in functional outcomes.
Conclusion: In this report, we describe our approach for procuring three allografts in the first successful face and bilateral hand transplant. In addition to meticulous preparation, this case highlights the importance of understanding and prioritizing the recipient’s goals for the transplant.
Pulsatile versus continuous flow in swine hindlimb preservation using subnormothermic machine perfusion
Pierre G Tawa1,2,3, Marion Goutard1, Alexandre G Lellouch1, Golda Romano1, Victor Pozzo1, Reinier J de Vries1, Casie Pendexter3, Sarah Maggipinto1, Laurent Lantieri4, Curtis L Cetrulo1 and Korkut Uygun3
1Massachusetts General Hospital, Boston, MA, USA
2Harvard Medical School, Boston, MA, USA
3Shriners Hospitals for Children, Boston, MA, USA
4Hopital Européen Georges Pompidou, Paris, France
Introduction: Multiple perfusion systems have been investigated on swine vascularized composite allografts, with various temperatures and different preservation solutions, most using continuous flow. However, the physiological flow is pulsatile and provides better outcomes in kidney and lung ex vivo perfusions. We aim to compare pulsatile flow with continuous flow in our 24-h subnormothermic machine perfusion protocol on swine hindlimbs.
Methods: Partial hindlimbs were harvested on Yorkshire pigs. Each limb was perfused with 2 L of modified Steen acellular solution at 20°C for 24 h, with 50% perfusate exchange (1 L) at 12 h. Group A (n = 3) was perfused with continuous flow through our custom-made machine perfusion, while group B (n = 3) was perfused with pulsatile flow at 60 bpm with the Liver Assist® machine. Viability parameters (arterial resistances, lactate, and potassium levels) and edema (defined by weight gain) were collected at different timepoints.
Results: Throughout the perfusion, arterial resistances remained stable around 1 mm Hg/mL/min in both groups. Lactate levels increased steadily and were depleted partially with the 50% perfusate exchange at 12 h. Potassium concentration plateaued at 5 mmol/L and remained below 5.8 mmol/L in both groups after 24 h of perfusion. Mean weight gain at the end of perfusion was higher in the continuous flow group (35%) compared with the pulsatile flow group (19%).
Perfusion parameters.
Conclusion: Pulsatile flow offers similar outcomes to continuous flow in vascularized composite allografts viability after 24 h of perfusion and demonstrates a trend in the reduction edema after subnormothermic preservation. We hypothesize that pulsatile flow is essential to preserve an optimal endothelial function, thus limiting edema after 24 h of vascularized composite allografts ex vivo perfusion.
Machine perfusion of vascularized composite allografts in small animal model
Dor Yoeli1, Yong Wang1, Bing Li1, Joy L Huang1, Swati Jain1, Zhaohui Wang1, Niyati Nakra1, Jerry Yang1, Kelsey Rampalski2, An-Jey Su1, David W Mathes1, Kia M Washington1, Evan Farkash2, Alkesh Jani1 and Christene A Huang1
1University of Colorado Anschutz Medical Campus, Aurora, CO, USA
2University of Michigan School of Medicine, Ann Arbor, MI, USA
Introduction: Machine perfusion may improve vascular composite allograft transplantation outcomes by mitigating ischemia reperfusion injury. The aim of this study was to evaluate the capability of preserving a small animal hind limb graft for 24 h with hypothermic machine perfusion in comparison with static cold storage preservation.
Methods: Six male Brown Norway rats (14–18 weeks old) were used as hind limb donors, with one limb subjected to 24 h of hypothermic machine perfusion (flow rate of 0.2 mL/min with heparinized KPS-1® solution) and the contralateral limb subjected to 24 h of static cold storage. Continuous variables are presented as mean (±standard deviation) and compared using two-sample or paired Student’s t test. Edema scores were compared using the Wilcoxon matched-pairs signed-rank test.
Results: On average, hypothermic machine perfusion limbs gained 1.58 (±0.98) g and static cold storage limbs gained 0.15 (±0.77) g after 24 h, representing a statistically (p = 0.02) but not clinically significant change. There was no significant difference in the skin or muscle histological edema score between treatment groups (p = 0.5 and 0.2, respectively). In total, 50% of the hypothermic machine perfusion limbs demonstrated moderate or severe nerve edema in comparison to only 17% in the static cold storage group (p = 0.03) (Figure 1). Among the hypothermic machine perfusion limbs, there was no significant change in vascular resistance from baseline (181.43 ± 46.59 mm Hg*min/mL) and 24 h (249.18 ± 257.62 mm Hg*min/mL) (p = 0.5).
Discussion and Conclusion: Rodent hind limb vascular composite allografts can be preserved up to 24 h with hypothermic machine perfusion with minimal edema and stable vascular resistance. Greater nerve tissue edema was observed with hypothermic machine perfusion, but the clinical significance of this finding will need to be investigated in future studies.
(a) Static storage muscle with moderate edema, (b) perfused muscle with mild edema, (c) static storage nerve with moderate edema and (d) perfused nerve with severe edema.
Bruce E Gelb, Daniel Boczar, Jorge Trilles, Zoe P Berman, Bachar F Chaya, Ricardo Rodriguez Colon, Gustave K Diep and Eduardo D Rodriguez
NYU Langone Health, New York, NY, USA
Introduction: Acute rejection is exceptionally common in the first year after vascularized composite allotransplantation. Recipients with burns are at increased risk of developing donor-specific antibodies due to sensitization. Lymphocyte depleting induction with rabbit antithymocyte globulin is commonly utilized. We hypothesized that combination B- and T-cell depletion induction therapy is more efficacious in preventing acute rejection in the early post-transplant period.
Methods: Our induction protocol calls for intraoperative administration of methylprednisolone (1000 mg) and rabbit antithymocyte globulin beginning intraoperatively (1.5 mg/kg, cumulative dose 6 mg/kg over the first postoperative week) and rituximab (1000 mg administered on postoperative day 1) for thorough T and mature B-cell depletion. Standard infection prophylaxis is utilized. Donor-specific antibodies are monitored postoperatively with Luminex® single-antigen microbeads (mean fluorescence intensity ⩾ 1000 considered clinically significant).
Results: Our latest recipient was a 22-year-old male with 80% total body surface area burns. The donor was an ABO-identical, 47-year-old brain dead male. Human leukocyte antigen (HLA) mismatch was 0, 1, 0 (A, B, DR), and 2 HLA-DPB1. Donor-recipient complement-dependent cytotoxicity and flow cytometric T- and B-cell crossmatch were all negative. Abrupt rise in donor-specific antibodies on postoperative days 7 and 8 was treated with two rounds of plasmapheresis and intravenous immunoglobulin. Persistent wound colonization (Acinetobacter baumannii) was treated with meropenem, polymyxin, and tigecycline. The recipient experienced a single episode of acute rejection 9 months post-transplant, successfully treated with pulse doses of methylprednisolone (500 mg intravenous, daily) over 3 days. We suspect this may have been triggered by inflammation induced by revision surgery of all three vascularized composite allotransplantation components in the preceding month.
Conclusion: We present our third consecutive vascularized composite allotransplantation recipient utilizing this novel immune strategy. In the context of the most extensive vascularized composite allotransplantation performed to date, acute rejection was prevented until 9 months post-transplant in this highly sensitized patient. Two previous recipients remained rejection-free for greater than 1 year post-transplant and have experienced only one rejection episode each to date. Acute rejection in vascularized composite allotransplantation may be better prevented by including rituximab in the induction immunosuppression strategy, and the risk of metabolic or severe infectious complications appears to be manageable.
The FDA has cleared all pharmaceuticals and/or medical devices for the use described in this presentation.
Accelerated functional recovery following combined face and bilateral hand transplant
Bruce E Gelb, Zoe P Berman, Gustave K Diep, Daniel Boczar, Jorge Trilles, Ricardo Rodriguez Colon, Bachar F Chaya and Eduardo D Rodriguez
NYU Langone Health, New York, NY, USA
Introduction: Vascularized composite allotransplantation has redefined the frontiers of plastic and reconstructive surgery. The field has seen considerable advancement since its inception, with the first successful hand transplant in 1998 and the first partial face transplant in 2005. To date, over 40 bilateral hand transplants have been reported in the literature, along with 47 face transplants. Due to still limited available evidence and the heterogeneity of the sample population, little consensus exists on the anticipated timeline of functional recovery following vascularized composite allotransplantation. We hereby report on the early and accelerated functional recovery of a combined face and bilateral hand transplant recipient.
Methods: A 21-year-old male was referred with sequelae of an 80% total body surface area burn sustained in a motor vehicle accident 1 year prior. The patient had extensive facial and bilateral upper extremity injuries. Serial debridement and split thickness skin grafting procedures left the patient with proximal digital syndactyly and distal digit amputations. Procurement and transplantation of the face and upper extremities was performed over a 23-h period in August of 2020. Postoperative functional assessment at predetermined time points included active range of motion, grip strength, sensory assessment, Carroll’s Upper Extremity Function test, and the Disabilities of the Arm, Shoulder, and Hand questionnaire.
Results: Functional assessments were performed at 3 and 6 months post-transplant. Range of motion, grip strength, Carroll’s test scores (left = 58 at 6 months post-transplant vs 13 pre-transplant, right = 61 at 6 months post-transplant vs 20 pre-transplant) and Disabilities of the Arm, Shoulder, and Hand evaluation (37 at 6 months post-transplant vs 90 pre-transplant) showed substantial improvement. The patient remained rejection-free during the first 9 months post-transplant and has had steady and progressive functional improvement. He is highly motivated and consistently demonstrates functional independence in activities of daily living.
Conclusion: Combined face and bilateral hand transplant is a feasible, comprehensive reconstructive solution for composite face and bilateral hand injury in the appropriately selected recipient. Patient motivation, psychosocial support, intensive physical and occupational therapy, and vigilant clinical and immunologic surveillance are essential features of postoperative recovery.
Upper limb transplant patients with a history of life-threatening sepsis experience significantly deeper post-transplant renal impairment than patients with non-sepsis limb loss
David A Leonard1, Amr M Elbatawy2, Sarah Taplin2, Richard J Baker2 and Simon PJ Kay2
1University of Glasgow, Glasgow, Scotland
2Leeds Teaching Hospitals NHS Trust, Leeds, UK
Background: Nephrotoxicity is a well-recognized complication of tacrolimus. Pre-transplant assessment of all patients includes evaluation by a transplant nephrologist and serial assessment of renal function by blood biochemistry. We highlight the potential for severe post-transplant renal impairment in upper limb transplant patients with a history of severe sepsis.
Methods: This is a longitudinal observational study of patients under the care of Hand Transplant UK. Clinical parameters were gathered from the electronic patient records. Analysis was performed in Graphpad Prism. Comparison was made between patients with post-sepsis amputation, and those with non-septic limb loss.
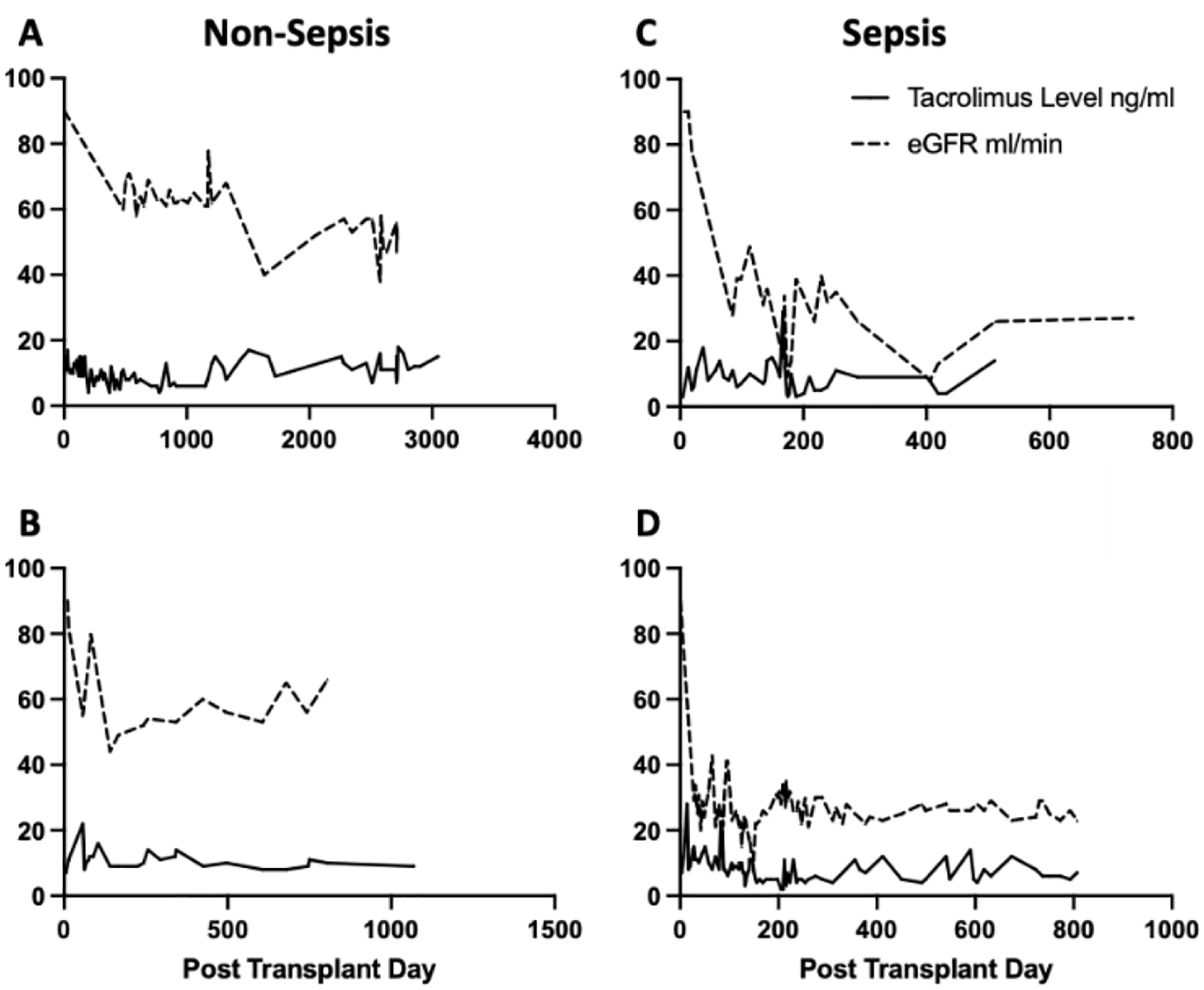
Results: All patients had nominal pre-transplant renal function (estimated glomerular filtration rate > 90 mL/min/1.73 m2). Post-transplant, all patients experienced renal impairment. For post-sepsis patients this resulted in mean post-transplant estimated glomerular filtration rates of 33 (range 8–78) mL/min/1.73 m2 and 26 (range 11–43) mL/min/1.73 m2. Patients with non-sepsis limb loss experienced less pronounced impairment with mean estimated glomerular filtration rates of 60 (range 38–80) mL/min/1.73 m2 and 62 (range 44–82) mL/min/1.73 m2. Mean trough tacrolimus levels did not differ significantly between the two groups (8.9 vs 10.5 ng/mL, respectively).
Conclusion: Despite normal pre-transplant blood renal biochemistry in all patients, post-sepsis patients experienced significantly more severe post-transplant renal impairment. While this has been well tolerated by both patients, it remains a cause for concern. We hypothesize that such patients may harbor subclinical renal parenchymal scaring which is unmasked on induction of immunosuppression. We are considering inclusion of 99mTc-DMSA renal cortical scintigraphy for subsequent post-sepsis patients, and would suggest that, at minimum, candidates for reconstructive transplantation post-sepsis should be specifically counseled regarding the potential for severe post-transplant renal impairment.
Post-sepsis patients experience more severe renal impairment post-transplant than non-sepsis amputees.