
Abstract
Objective:
Diabetic retinopathy is an evident complication of diabetes on eye and contributes for significant portion of blindness worldwide. In Ethiopia, data are lacking on awareness and knowledge of diabetic retinopathy in diabetic patients. This study desired to assess knowledge of diabetic retinopathy and it is relating factors among diabetic patients attending at a General Hospital in Ethiopia.
Methods:
We have interviewed 306 diabetic patients who were attending at Debre Tabor General Hospital. Binary logistic regression model was used to recognize associated factors to good knowledge of diabetic retinopathy. Adjusted odds ratio was used to show the power of association. A p-value of less than 0.05 was set to determine its statistical significance.
Result:
The diabetic patients had a median age of 45 (range = 30) years. From the total diabetic patients, 242 (79.10%) knew that diabetes could affect the eye and 81 (26.50%) were aware of diabetic retinopathy. From those who were informed of diabetic retinopathy, 32 (39.50%) (95% confidence interval = 27.90–51.20) had good knowledge of diabetic retinopathy. High educational status (adjusted odds ratio = 4.08, 95% confidence interval = 1.00–16.50) and non-government employee (adjusted odds ratio = 0.19, 95% confidence interval = 0.05–0.70) were significantly associated with good knowledge of diabetic retinopathy. Physicians and eye doctors were the most frequent source of information for the awareness of diabetic retinopathy.
Conclusion:
From the total diabetic patients recruited in the study, 39.5% of them obtained information about diabetic retinopathy and the overall knowledge was poor among them. Knowledge of diabetes can affect the eye and it causes blindness was good among majority of the participants. Higher educational status and being a non-government employee were determined to be important predisposing factors of good knowledge. It is also better to involve diabetic educators and counselors in educating diabetic patients on the serious complication of diabetes on eye.
Introduction
Diabetic retinopathy (DR) is a usual long-term microvascular complication of diabetes on eye, and remains one of the leading causes of preventable blindness in middle aged and elderly people in the world. 1 Worldwide, the prevalence of DR in adult diabetic patients was reported to be 27% and it makes up 4.8% of cases of blindness.2,3 In reference to a recent systematic review made based on aggregation of various studies in Ethiopia, the prevalence of DR was estimated to be 19.48% in the nation. 4 Grievous visual impairment due to DR curbs patients’ capacity to manage their disease properly; hence, it will significantly impair their quality of life and diminish productivity and life expectancy. 5
In its early development, DR is asymptomatic in most of the cases. Therefore, timely screening, detection, and treatment are crucial to lessen grieve visual impairment associated with it. Early prevention helps to curb other diabetic complications and this is supported with randomized control trials which have shown that, early treatment can reduce an individual risk of grieve visual impairment by 57%. In this regard, awareness and good level of knowledge of DR play a significant role. It helps diabetic patients to have good practice on diabetic self-management, watching potential risk factors and allowing them to develop a positive attitude for an early screening and timely treatment. Furthermore, studies on the knowledge of DR help to influence policy makers for a strategic intervention for the diseases.
The major risk factors for the development DR in diabetic patients are longer diabetes, poor blood glucose control, inflammation, hyperlipidemia, obesity, and hypertension.3,6,7 Protection of sight from DR can be achieved through effective screening, timely laser treatment, intraocular injection of steroids and antivascular endothelial growth-factor agents, and intraocular surgery.8,9 In this regard, the high level of awareness and knowledge about DR plays a significant role in the overall management of DR and prevention of severe visual impairment.
In spite of the fact that, Ethiopia experiences a surge in the prevalence of diabetes and its major complications, there is a lack of evidence addressing the knowledge and eye checkup practice of diabetic patients toward DR. Therefore, this study aimed to assess the knowledge of diabetic patients about DR and its related factors at a General Hospital in Northwest Ethiopia.
Methods
The source population was diabetic patients attending at a General Hospital in Ethiopia. The hospital is situated in the capital city of South Gondar Zone of the Amhara National Regional State located 667 km from the country’s capital, Addis Ababa. Data obtained from the Debre Tabor Hospital Planning and Information Department showed that, the hospital is providing preventive and curative health care services for about ~2.7 million people in the zone and surrounding area. 10 The hospital has specialty chronic illness clinics where patients with diabetic patients have linked for regular follow-up. On average around 15 diabetic patients are visited in the two diabetic clinics per day during the working hours. General practitioners, internists, and nurses are involved in the clinical service of diabetic patients. Also in the hospital, ophthalmologists, optometrists, cataract surgeon, and ophthalmic nurses are giving eye care service in the eye care clinic. A cross-sectional study was carried out from 24 August 2020 to 24 September 2020.
Exclusion criteria
Diabetic patients who were severely ill admitted in the inpatient department.
Diabetic patients with mental health problems who are unable to be administered for the questionnaire.
The sample size was determined based on a simple proportion formula with 50% level of good knowledge on DR, 5% degree of precision, and two-sided 95% confidence interval (CI). Accordingly, the calculated sample size was 384. Considering reduction formula for 1200 total diabetic patients attending in the hospital and 10% non-response rate, the final sample size would become 322. Hence, the total population during the data collection period was expected to be around 330, all of the diabetic patients who fulfilled the eligibility criteria were considered for participation. Therefore, when 306 samples were recruited for the study, below 10% of the total calculated sample size would remain.
Ethical consideration
Ethical clearance was obtained from University of Gondar, College of Medicine and Health Sciences, School of Medicine ethical review committee. Moreover, permission to conduct the study in the hospital was obtained from Chief Executive Officer and Medical Director Offices of the hospital. The written informed consent was waived by the Institution Review Board of University of Gondar. Generally, the study was conducted in line with the Ethical Principle of the Declaration of Helsinki.
Diabetic patients’ data on knowledge of DR
Data were ascertained through a structured interviewer-administered questionnaire, which was developed from reviewed literatures.11–14 The questionnaire consisted of 23 items (8 socio-demographic and economic variables, 5 diabetic follow-up and eye checkup, 1 source of information, and 9 knowledge questions). Pretest on 5% of the sample in Bahir Dar Referral Hospital and training of the data collector was done to maintain the quality of data collection procedure. The interview was conducted by four trained BSc nurses.
Participants’ knowledge on DR was assessed using seven questions organized on different dimensions of DR, such as, definition of DR, factors of DR, treatment option of DR, and eye checkup schedule of diabetes, that were composed to give a value of 1. Each correct answer had a value of 1 and incorrect answer had 0. The overall knowledge of the participants was labeled as good if the score was greater than the median score of knowledge-related questionnaire and, otherwise, poor knowledge of DR. 15
Statistical analysis
The data of diabetic patients were transcribed into EPI INFO 7 and converted to SPSS version 20 for analysis. The statistical analysis was then performed and the results of the analysis were presented using figure and table. Binary logistic regression model was employed to recognize important related factors for the knowledge of DR. Variables having p-values < 0.05 were taken as statistically significant factors.
Result
Diabetic patients’ socio demographic and economic characteristics
A total of 306 participants completed the study with a response rate of 95.0%. The median age of the respondents was 45 (interquartile range (IQR) = 30) years. Majority of the participants were male 166 (54.2%), Orthodox Christian 297 (97.2%), married 203 (66.3%), had no formal education 171 (55.9%), farmer 90 (29.4%) and urban dweller 193 (63.1%). The median family monthly income of the respondents was 3577 Ethiopian Birr (ETB) (IQR = 4500 Ethiopian Birr) (Table 1).
Socio-demographic and economic characteristics of study participants at Debre Tabor General Hospital, Northwest Ethiopia, 2021 (n = 306).

n: sample size; ETB: Ethiopian Birr.
Income was categorized based on quartile classification.
Clinical profile, follow-up, and family history–related characteristics of diabetic patients
The median duration of diabetes was 4 (range = 7) years. From the total participants, 163 (53.3%) were type 1 diabetes mellitus (DM), 228 (74.5%) visited the DM clinic every month, 72 (23.5%) had family history of DM, and 126 (41.2%) had no prior eye checkup (Table 2).
Clinical and behavioral characteristics of study participants at Debre Tabor General Hospital Northwest Ethiopia, 2021 (n = 306).
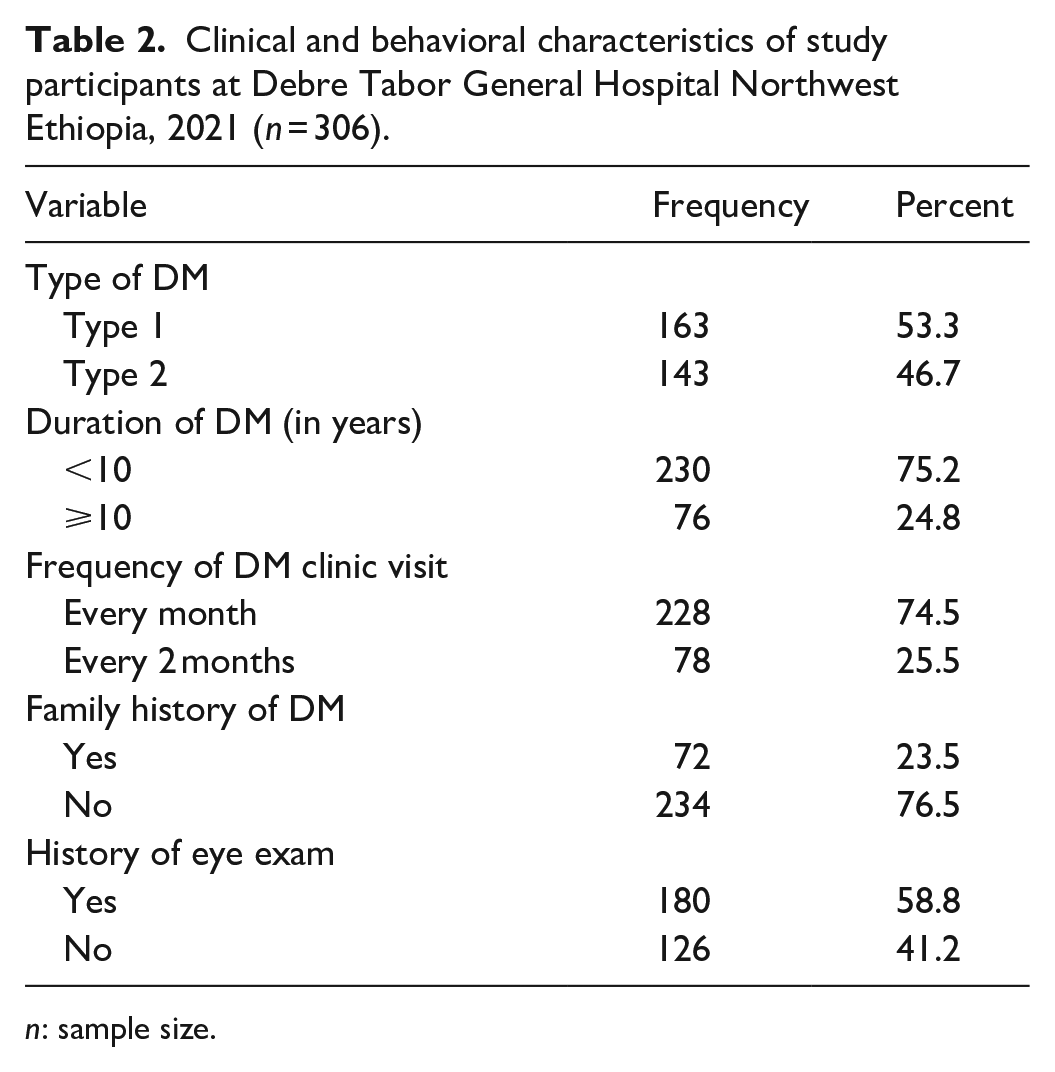
n: sample size.
Knowledge of DR in diabetic patients
From the total of 306 participants, 242 (79.1%) knew that diabetes could affect the eye and 81 (26.5%) were aware of DR. The median knowledge score point for those who were aware of DR was 5.00 ± 1.87. From those participants who were aware of DR, 32 (39.5%) (95% CI = 27.9–51.2) participants had good knowledge of DR. Regarding the detailed knowledge of DR, 73 (90.1%) knew that diabetes can causes blindness, 60 (74.1%) knew that poor control of glucose affects the progression of DR, 14 (17.3%) knew that surgery was the treatment option of DR, and 75 (92.6%) knew that patients should have a periodic dilated eye checkup for possible DR. Only 12 (14.8%) of participants believed that a person with DR could have a normal vision (Table 3).
Knowledge of diabetic retinopathy among adult diabetes at Debre Tabor General Hospital North West, Ethiopia, 2021 (n = 306).

DR: diabetic retinopathy; DM: diabetes mellitus.
Majority of the participants heard about DR from physicians, media, and eye doctors, while most of the other participants used books and friends as a source of information for their awareness of DR and very few others heard from friend and other source (Figure 1).

Source of information for DR among diabetes at Debre Tabor General Hospital, Northwest, Ethiopia, 2020.
Related variables with knowledge of DR in diabetic patients
Following a multivariable logistic regression analysis, educational and occupational status were found to have been significantly related with the good knowledge of DR. Diabetic patients with a higher level of education (college and above) were 4.08 times more likely to have a good knowledge of DR compared to those who had a lower level of education or no formal education (adjusted odds ratio (AOR) = 4.08, 95% CI = 1.00–16.34). Diabetic patients who were government employee were 81% less likely to have good knowledge as compared to diabetic patients who did not have any job (AOR = 0.19, 95% CI = 0.05–0.70) (Table 4).
Bivariable and multivariable logistic regression analysis of factors associated with knowledge of diabetic retinopathy among adult diabetes at Debre Tabor General Hospital, Northwest Ethiopia, 2021 (n = 306).
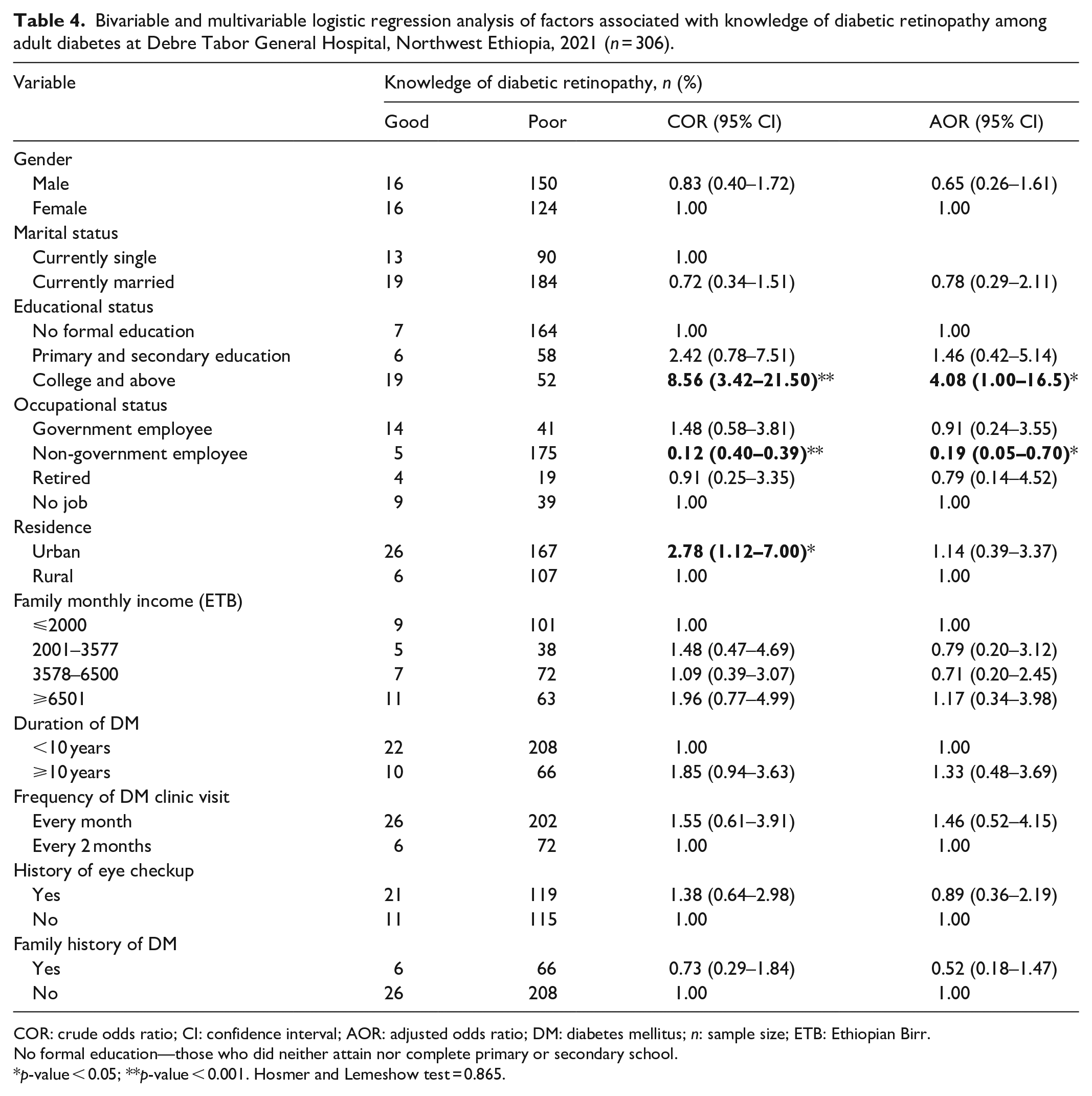
COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; DM: diabetes mellitus; n: sample size; ETB: Ethiopian Birr.
No formal education—those who did neither attain nor complete primary or secondary school.
p-value < 0.05; **p-value < 0.001. Hosmer and Lemeshow test = 0.865.
Discussion
This study was attempted to obtain evidences on the knowledge of DR and its related factors in a diabetic population attending at a general hospital in Ethiopia. Nearly 80% of the diabetic patients believed that diabetes can affect the eye, this finding was corroborated with a similar studies conducted in Goa, India (78.8%), 16 Jeddah, Saudi Arabia (82.6%), 17 and llorin, Nigeria (76.4%). 13 However, the finding was higher than the study in Pakistan (67.0%), 18 and lower than studies in United States (91.2%), 19 Syria (93.8%), 20 Jordan (98.3%), 21 and Iraq (95%). 22 The disparity might be attributed for the difference in study settings, sample size, and inclusion criteria.
The knowledge of DR was good among 39.5% of the diabetic population in the general hospital, the figure was consistent with that of Goa, India (34.1%), 16 and higher than Peshawar, India (24.5) 23 yet lower than Tamilnadu, India (87%). 24 Difference in the study set-up, and the nature of study populations involved might be responsible for the observed discrepancy in the knowledge figures. For instance, study in Tamil Nadu India was on patients who were presented to ophthalmology department and teaching center where the patient’s knowledge of DR could be improved through better health education.
Regarding the detailed knowledge of DR, nearly 24% of the diabetic patients reported that, DR can cause blindness and 24.5% of the diabetic patients believed that periodic eye check would be necessary for diabetic patients. These figures were found to be lower compared to similar studies in Hong Kong, 25 Syria, 20 Jordan (81%), 26 and Karachi, Pakistan. 18 These differences might be attributable to the difference in the study population characteristics, for instance, only 22.2% of participants were illiterate in Karachi, Pakistan, as opposed to 55.9% in the present studies and this makes up a better knowledge of DR.
The knowledge of good glucose control helps to prevent DR was reported by majority of the diabetic patients 74.1% consistent with studies in Jordan, 26 and Riyadh, Saudi Arabia, 27 while it was lower than Iraq. 22 The previous study in Iraq was on a teaching hospital where a better health education and eye care service could be given to enhance the knowledge on controlling glucose and prevention of DR. A few portion of the diabetic patients believed that DR could be treated with laser (9.9%) and surgery (17.3%) lower compared to Jeddah, Saudi Arabia (25%). 17 The variation could be explained by the difference in educational status of participants, in which almost 75% of participants in Saudi Arabia had formal education as opposed to half of the study participants in this study had formal education.
This study also found out that, educational and occupational statuses were important risk factor for good knowledge of DR consistence with studies in Peshawar, India, 23 Goa, India, 16 Jordan, 26 Pakistan, 18 and Saudi Arbia. 27 Participants with higher educational status could have prioritized knowledge of DR at different stages of their education and through seminars or reading books. Highly educated diabetic patients could read more about their health than those who are not educated. This study also indicated that diabetic patients who were non-government employee had 81% times less likely to have good knowledge as compared to those who had no job. The possible reason for the association might be due to very few numbers of diabetic patients who were non-government employee heard about DR from physicians and eye doctors, who provide complete and reliable information on DR, for a good level of knowledge.
Moreover, this study identified physician followed by eye doctors and media as the most frequent sources of information for the awareness of DR. This was in accordance with studies in Malysia, 28 Goa, India, 16 Jordan, 26 Iraq, 22 and Saudi Arabia15,27 where physician, eye doctor, and media were identified as the most frequent sources of information for the awareness of DR among diabetes.
Study limitation
The study had the following limitations; it was conducted in a single hospital and included relatively a few diabetic patients. Therefore, the result of the study may not be able to reflect the overall knowledge of the condition in the general diabetic population.
Conclusion
The overall knowledge of DR was poor among majority of diabetic patients; however, majority of them believed that diabetes causes blindness. Higher educational status and being non-government employee were associated with good level of knowledge on DR. It was also found out that physicians and eye doctors were remained to be the most reliable source of information for the knowledge of DR. It is highly crucial for the hospital administration, eye care professionals, and physicians to come together for a strategic intervention to improve the knowledge of DR among diabetic patients through health education in the hospital. It is also important to involve diabetic educators and counselor to in the education of diabetic patients.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211054994 – Supplemental material for Awareness and knowledge of diabetic retinopathy in diabetic patients at a General Hospital in Northwest Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121211054994 for Awareness and knowledge of diabetic retinopathy in diabetic patients at a General Hospital in Northwest Ethiopia by Getasew Alemu Mersha, Yezinash Addis Alimaw, Asamere Tsegaw Woredekal, Aragaw Kegne Assaye and Tarekegn Chekilie Zeleke in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express our deepest gratitude to Debre Tabor General Hospital for letting the data collection at the hospital and the senior clinical nurse professionals who faced exhaustive data collection process. The authors wish to thank the study participants for their willingness to participate in the study. This study did not receive funding from any organization.
Author Note
Asamere Tsegaw Woredekal is now affiliated to Department of Ophthalmology, School of Medicine, University of Gondar, Comprehensive Specialized Hospital, Gondar, Ethiopia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the University of Gondar, College of Medicine and Health Science, Ethical Review Committee. Ethical approval was accepted from University of Gondar Ethical Review Committee with an ethical approval no. of S/N/1356/2011E.C.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
We did explain to the study subjects shortly about the purpose of the study. The written informed consent was waived by the Institution Review Board of University of Gondar.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.