
Abstract
Objective:
Despite the reproductive health needs of youth having been supported by different organizations, youths continue to fall victim to sexual and reproductive health problems, and utilization of those services remains low. All efforts have not been felt across the Ethiopian learning institutions as is evidenced by persistent reproductive health problems. This study was aimed to determine sexual and reproductive health service needs among preparatory school youths of Debre Tabor town, Ethiopia.
Methods:
Facility-based cross-sectional study design was conducted in Debre Tabor town from 15 to 30 February 2020. A simple random sampling technique was used to access a total of 850 preparatory school students. The data were collected using pre-tested, structured, and self-administered questionnaires. Data were entered into EpiData v. 4.6 and exported to SPSS version 25 software for analysis. Binary logistics regression was used for analysis. Adjusted odds ratio along with 95% confidence interval was estimated to measure the strength of the association. The level of statistical significance was declared at a p value of 0.05.
Results:
The overall magnitude of sexual and reproductive health service needs was found 61.5% at 95% confidence interval (58.2%, 64.8 %). Being married (adjusted odds ratio = 2.24; 95% confidence interval: 1.10, 4.55), having information about sexual and reproductive health (adjusted odds ratio = 2.56; 95% confidence interval: 1.85, 3.55), youth discussion with families on sexual and reproductive health (adjusted odds ratio = 1.52, 95% confidence interval: 1.11, 2.10), and having a history of sexual intercourse (adjusted odds ratio = 2.19; 95% confidence interval: 1.53, 3.13) were found significantly associated with sexual and reproductive health service needs of youths.
Conclusion:
the overall need for sexual and reproductive health services among youths was found high. Therefore, managers and health workers need to prioritize an intervention that can improve youth-friendly service, information dissemination, and counseling, promoting discussion among family members on the sexual and reproductive health needs of the youths.
Introduction
Reproductive health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity, in all matters relating to the reproductive system. It is critical during youth age and affects the health of the next generation. 1 Every year, an estimated 1.7 million youths lose their lives prematurely related to reproductive health problems. 2 Globally, more than 25% of the world’s population is between the age of 10 and 24 years; of those 86% of them are living in developing countries including Ethiopia. 3
Youth is characterized by significant physiological, psychological, and social changes. Ethiopia has a rapidly growing population, especially the adolescent and youth age group population that makes up 33.8% of the Ethiopians. 4 Young people experience many significant sexual reproductive health challenges as inadequate access to youth-friendly services (YFSs) as well as information on growth, sexuality, and family planning. 5 This has led youth into risky sexual behaviors resulting in high sexually transmitted infection (STI) and HIV prevalence, early pregnancy, and vulnerability to delivery complications resulting in high rates of death and disability.5 –7
Parents, teachers, and other adults widely fail to prepare young people with the information, skills, and resources needed to plan a steady, healthy course through the transition to adulthood. 8 As a result, youths are experiencing different health outcomes related to sexual and reproductive health (SRH). 9
YFS should be accessible, acceptable, and appropriate to the needs of young people. The World Health Organization (WHO) definition of YFS requires that such services should be in the right place, at the right time, at the right price, and delivered in the right style to be acceptable to young people. In addition, the services should be effective, safe, and able to meet the individual needs of young people—who will then return when they need to and recommend these services to friends. 10
Nationally, in Ethiopia, different promising practices are implemented, and direction and activities are done to implement SRH services to youths like accessing YFS, developing national adolescent and youth SRH strategies, developing a health sector transformation plan (HSTP), and universal health coverage through sustainable development goals (SDG) and formulate family law. 7
Generally, there is little evidence on these services and the local information required on the SRH needs of school youth. Therefore, this study was aimed to assess the reproductive health service needs of youths in Debre Tabor town preparatory school students, and it identified important factors that need to be addressed and make a difference in the youths’ health service needs satisfaction.
Methods and materials
Study area and period
The study was conducted in Debre Tabor town from 15 to 30 February 2020 G.C. It is the seat of the South Gondor administrative zone. This town is 676 km away from the capital city of Ethiopia (Addis Ababa), and 103 km away from the regional capital city of Amhara (Bahir Dar). According to the 2007 central statics agency report and current projection in 2019, Debre Tabor town has a total population of 60,563 where 33,651 are males. The town had one general hospital, three health centers (HC; only one HC provides YFS), and a family guidance association of Ethiopia that delivers YFS. The town had three preparatory schools and there were around 3438 students, of which 2021 students were males (South Gondor education bureau report, 2020).
Source and study population
All the three Debre Tabor preparatory school students (age 15–29 years) were considered as the source population, while the randomly selected Tewodros, the 2nd preparatory school, was used as the study population of this study.
Eligibility criteria
All Debre Tabor preparatory school students aged ⩾15 were included in the data collection process of this study, while those who were severely ill during the data collection period were excluded from the study.
Sample size determination and sampling procedure
The sample size required for this study was calculated using a single population proportions formula considering the following assumptions. Prevalence of SRH needs was 76.3%, 11 95% confidence level, 10% non-response rate, and 3% margin of error

Adding a 10% non-response rate, the final sample size used for this study was 850 samples.
Debre Tabor town has three preparatory schools; among these, Tewodros, the 2nd preparatory school students, was selected by lottery method (considering feasibility) as a study population. Here in this school, there were 1178 students; of these, 632 were males, and 639 were grade 11 students. Then, the sample size was proportionally allocated to each grade (11 and 12) based on the number of students available in each grade level. Then, 461 and 389 students were sampled from grades 11 and 12, respectively. The lottery method was applied to access the study participants in each grade taking the roster as a sampling frame. Finally, 454 and 384 students were involved in the study from grades 11 and 12, respectively.
Operational definitions
Youth is the age between 15 and 29 years. 4
SRH needs: Youths who have a perceived need for at least one of the following SRH service components: abortion, STI diagnosis and treatment, condom use, voluntary testing and counseling (VTC) with HIV counseling and testing, RH information, counseling, contraception, and maternity care (pregnancy test, antenatal care (ANC), postnatal care (PNC)) were considered having SRH need (yes/no). 4
Attitude: Seven questions which have five ordered responses were used to measure the attitude of respondents toward SRH service needs and use. Respondents who have scored above or equal to the median value were considered as having a favorable attitude, while those who scored below the median value were considered as having an unfavorable attitude toward SRH service need and use. 10
Knowledge: Eight questions were used to measure the knowledge of the respondents on SRH needs. When respondents get the right answer, it was coded as yes “1”; if not it was coded as no “0” for the eight questions. Respondents who scored above the mean value were regarded as knowledgeable, whereas those who scored below the mean value were considered as not knowledgeable about SRH health service needs. 12
Data collection tools and procedures
The data were collected by using pre-tested, structured, and self-administered questionnaires prepared from reviewing previous similar literature.12 –14 The questionnaires were composed of socio-demographic factors, health system services accessibility, behavioral factors, sexual history, and family-related factors. Four diploma nurses were recruited as data collectors and two health officers were also recruited as supervisors. The questionnaires were developed in English and then translated into Amharic language and again translated back into English to ensure consistency. The 1-day training was given to data collectors and supervisors on the techniques of respondent approach, research ethics, and data collection procedures including how to ensure confidentiality and privacy. The data were pre-tested among 43 (5%) students in ferrite preparatory school and then necessary modification was made. The collected data were checked daily for completeness by the principal investigators and supervisors.
Statistical analysis
Data were cleaned and entered into EpiData v. 4.6 and exported to Statistical Package for Social Sciences (SPSS) v. 25 for statistical analysis. Descriptive statistics, such as frequency, proportion, and summary measures, were used. The association between independent variables and reproductive health service needs was made using a logistic regression model. All independent variables having a p value ⩽0.25 in binary regression were included in the multivariable logistic regression. Multicollinearity was checked using standard error, while Hosmer and Lemeshow tests 15 were used to check model fitness. Statistical significance was determined using an odds ratio with a 95% confidence interval (CI) and a p value of <0.05, and adjusted odds ratio (AOR) with a 95% CI was used to declare factors of statistical significance with SRH service needs of students.
Ethical considerations
Ethical clearance was taken from the Ethical Review Committee of Wollo University College of Medicine and Health Sciences with the APPROVAL NUMBER/ID: CMHS 465/02/12. A letter of permission to conduct the study was obtained from the Zonal Educational Administrative Office. After explaining the purpose of the study, written consent was obtained from participants before data collection. They were informed that participating in the study was voluntary and the right to withdraw from the study at any time was explained. Privacy of the respondents and confidentiality of information was secured at all levels. The interviews were conducted in a private room and personal identifiers were not used during the data collection process.
Results of the study
Socio-demographic characteristics of the respondents
A total of 838 respondents were included in this study making a response rate of 98.6%. Among the study participants, 495 (59.1%) were females and the mean (±SD) age of the respondents was 19.4 (±1.79) years. Regarding their religion, 762 (90.9%) were Orthodox Christian, and 548 (65.4%) reside in the urban area, most of the study participants were single in marital status (735 (87.7%)) (Table 1).
Socio-demographic characteristics of students in Debre Tabor preparatory schools, Northwest Ethiopia, 2020 (n = 838).

Sexual and family-related characteristics of the respondents
Among the study participants, 310 (37%) had a history of sexual intercourse in their life, and the mean (±SD) of first sexual initiation was 18.19 (±3.33) years. Regarding the discussion about SRH, 439 (52.4%) did not have a discussion about SRH with their families (Table 2).
Sexual and family-related characteristics among students of Debre Tabor preparatory school, South Gondor Zone, Northwest Ethiopia, 2020 (n = 838).
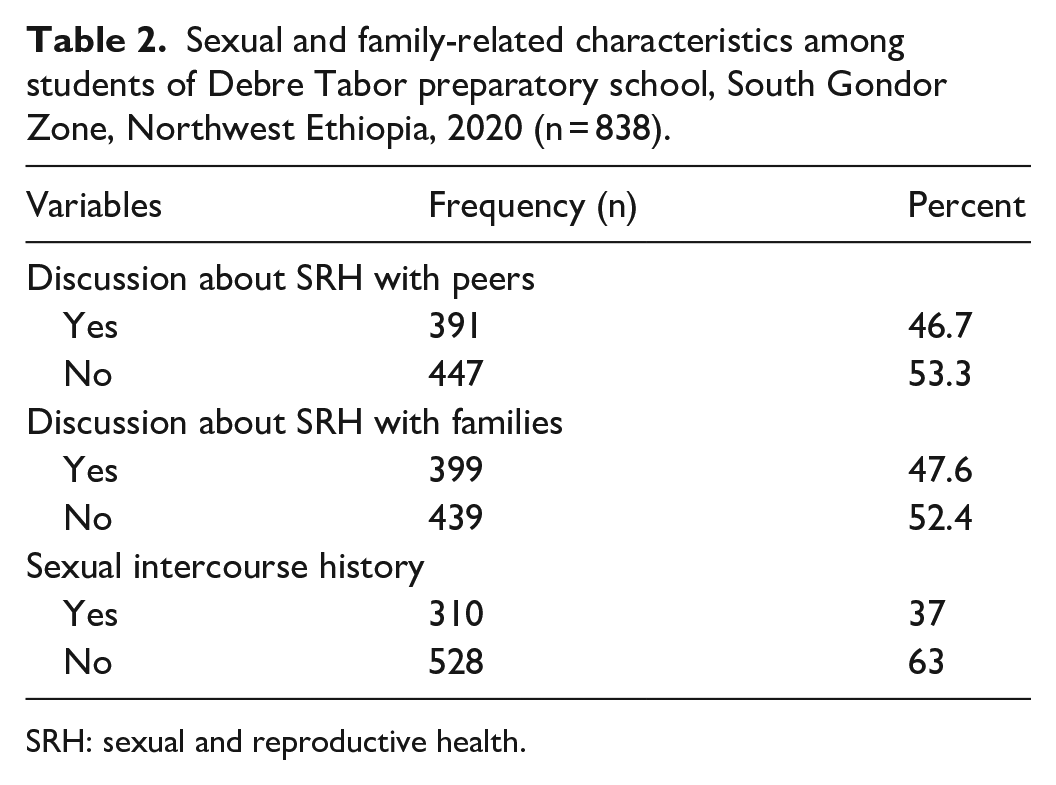
SRH: sexual and reproductive health.
Health service accessibility and behavioral characteristics of respondents
Among the respondents, 564 (67.3%) have access to SRH services (like information), and 554 (66.1%) say long waiting time was one of the reasons that reduce their need for reproductive health services. Along with the knowledge status, 589 (70.3%) were knowledgeable about SRH services, and 647 (77.2%) have a favorable attitude toward the need for reproductive health services (Table 3). About 265 (31.5%) of respondents had no information about SRHs, whereas about 203 (24.2%) and 124 (14.8%) of respondents got information from health professionals and mass media, respectively, about SRHs.
Health service accessibility and behavioral related characteristics among students of Debre Tabor preparatory school, South Gondor Zone, Northwest Ethiopia, 2020 (n = 838).

SRH: sexual and reproductive health.
SRH services need
The overall magnitude of at least one component of SRH service needs in life was 61.5 % with 95% CI: 58.2%−64.8%.
Components of SRH service needs
In all, 211 (25.2%), 195 (23.3%), and 181 (21.6%) respondents had reported that STI diagnosis and treatment, VTC, and SRH information seeking were the most reported components of SRH service needs, respectively.
Factors associated with SRH service needs
In the final multivariable regression model, having information about SRH, sexual history, discussion about SRH with families, being married, and educational status of respondents’ fathers were significantly associated with SRH service needs.
The odds of needing SRH services for those fathers’ education level was college and above were 73% less likely as compared to those whose fathers who cannot read and write (AOR = 0.27; 95% CI: 0.15–0.46). Regarding marital status, those who were married were 2.24 times more likely to need SRH services as compared to those who were single (AOR = 2.24; 95% CI: 1.10–4.55). The odds of SRH needs were 2.56 times higher among those who had information about SRH as compared to those who have no information about SRH services (AOR = 2.56; 95% CI: 1.85–3.55). Those who had a discussion about SRH with their families were 52% more likely to need SRH services compared to those who had no discussion with their families about SRH services (AOR = 1.52; 95% CI: 1.11–2.10). Likewise, those who had a history of sexual intercourse were 2.19 times more likely to need SRH services as compared to those who had no history of sexual intercourse (AOR = 2.19; 95% CI: 1.53–3.13) (Table 4).
Factors associated with sexual and reproductive health service need among Debre Tabor preparatory school students, South Gondor Zone, Northwest Ethiopia, 2020 (n = 838).

SRH: sexual and reproductive health; COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
p < 0.05; **p < 0.01; ***p < 0.001; Hosmer and Lemeshow test (x 2 = 8.272, df = 8, and p = 0.407), 1 = reference category.
Discussion
The overall magnitude of SRH service need was 61.5% at 95% CI: 58.2–64.8. This figure is lower than a study conducted in the Hadiya zone of 76.3%. 11 This discrepancy may be due to sampling size variation and time variation due to the change in accessible health services.
However, the result is higher than studies conducted in Zimbabwe (20%) and Ghana (42%),15,16 respectively. The possible reason might be the study population difference; in the study conducted in Ghana, youth who live in urban settings were included, but this study included those living in both urban and rural settings. Evidence revealed that youth who live in rural settings are more likely to need SRH services when compared to those who live in an urban setting. 17 There is low awareness among youths about their SRH service in this study. Evidence showed that youth having low awareness about SRH services, especially those who lack poor educational awareness, protection, and counseling, were more exposed to sexually risky behavior; they need more services to get the solution, specifically abortion and contraceptive methods.6,8,18
Marital status was found statistically significant with the SRH need of youth students. Those who are married were more than two times more likely to need SRH services compared to those who were single. This is in line with studies conducted in Zimbabwe. 17 The possible justification may be married women need different services especially related to maternity care, family planning to build families, and holding activities as per their plan and they can freely discuss with their partner, families, and friends that create a good opportunity to adequate awareness and positive attitude toward SRH service needs. Evidence revealed that youth who are in a union or married have more to access and need SRH services, especially family planning and maternity care.2,13
The educational status of families was a significant predictor of the SRH needs of the youths. The odds of students’ father educational level of college and above were 73% less likely to need SRH service as compared to those whose fathers were unable to read and write. On the contrary, in a study conducted in Ethiopia 19 and Uganda, 20 youths within more educated families were more likely to need SRH services. The possible justification might be that more educated families counsel their children and discuss at home about SRH sufficiently where they might not need SRH services from the outside; as a result that creates an opportunity for awareness and full source of information about SRH services, then they could abstain from risky sexual behavior.
Youths who have a history of sexual intercourse were 2.19 times more likely to need SRH service as compared to those who have no history of sexual intercourse. This finding is consistent with studies conducted in Ethiopia, Uganda, and Ghana,11,21,22 respectively. The possible reason might be exposed to sexual intercourse may lead to the need for SRH services like contraceptives, condoms, abortion, maternity care, HIV and STI treatment and counseling to prevent unwanted pregnancy, complications, and bad health consequences. Evidence shows that youth who had a history of previous sexual intercourse had frequently visited health facilities to get different SRH services particularly STI and HIV counseling and testing, and contraceptive services.2,14,23,24 Moreover, evidence revealed that youth who had risky sexual behavior had more need for abortion and condom use. 14
Having information about SRH was significantly associated with SRH service needs. This is in line with studies conducted in Ethiopia. 11 The possible explanation might be sufficient information about SRH that may increase the awareness and attitude of youth toward the need for SRH service. Evidence revealed that youth having good information about SRH is not only important in addition to get and need SRH service timely, but also important for youth’s general health and well-being. It is central to their ability to make informed choices and decisions about their lives, including when and whether to consider having children. Moreover, it is a good chance to create healthy and respectful relationships; health services that are inclusive, safe, and appropriate; access to accurate information; effective and affordable methods of contraception; and access to timely support and services concerning unplanned pregnancy. Having access to information about SRH that provides quality information about maintaining a healthy lifestyle and physical and mental health services can all help youth achieve optimal health, well-being, and more need SRH services.14,25
Discussion about SRH with families was significantly associated with SRH service needs. This is similar to studies conducted in Ethiopia. 12 The possible explanation might be family’s engagement in youth SRH needs helps them to develop the confidence to get additional information and service including the service delivery point. Evidence showed that parent–young people discussion and communication about SRH issues is crucial in not only increasing the need for SRH services but also creating good awareness and positive approaches to reduce risky sexual behaviors.25 –28
Limitation of the study
The study was not supported by the qualitative part for augmenting the findings.
It might be affected by social desirability bias which could affect the validity of the result.
Conclusion
The overall need for SRH services among youths was found high. Therefore, managers and health workers need to prioritize an intervention that can improve YFS service, information dissemination, and counseling, promoting discussion among family members on the SRH needs of the youths.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221113667 – Supplemental material for Sexual and reproductive health service needs among youths attending preparatory school in Debre Tabor Town, Northwest Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221113667 for Sexual and reproductive health service needs among youths attending preparatory school in Debre Tabor Town, Northwest Ethiopia by Metages Adane, Niguss Cherie, Yitayish Damtie, Mulusew Malde and Muluken Genetu Chanie in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Wollo University, College of Medicine and Health Sciences, and School of Public Health for giving me the chance of doing this research. We would like to express our deepest gratitude to Amhara Health Bureau for creating this opportunity and sponsorship. Our gratitude also again to data collectors and study participants.
Author contributions
All authors met the following criteria:
1. Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas.
2. Drafted or wrote, or substantially revised or critically reviewed, the article.
3. Agreed on the journal to which the article will be submitted.
4. Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
5. Agreed to take responsibility and be accountable for the contents of the article.
Availability of data and materials
The data sets used and/or analyzed during this study are available within the manuscript.
Consent for publication
All authors gave their consent for the publication of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the Ethical Review Committee of Wollo University College of Medicine and Health Sciences (APPROVAL NUMBER/ID: CMHS 465/02/12).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from each study participant.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.