
Abstract
Objective:
The objective of this study was to determine the magnitude of electrolyte disorders and influencing factors among cancer patients in Southwest Ethiopia.
Methods:
Facility-based cross-sectional study was conducted in Jimma Medical Center (JMC). Eighty-four cancer patients admitted to JMC were recruited for this study. A structured questionnaire and serum electrolyte measurements were used for data collection. Bivariate and multiple logistic regression was employed to determine the association between electrolyte disorders and associated factors among admitted cancer patients. P value ⩽ 0.05 was used as a cut point to declare statistical significance.
Result:
The overall prevalence of electrolyte disorders was 60.7%. The presence or absence of comorbid diseases, age, body mass index (BMI), nutritional status, and current prescribed medication use were associated with electrolyte disorders. Younger patients had lower odds for electrolyte disorders (odds ratio (OR) = 0.128 (P value = 0.05) and OR = 0.08 (P value = 0.033)) for the first and the second quartile, respectively. Underweight patients had a threefold likelihood to develop electrolyte disorders (OR = 3.13 (P value = 0.043)) than having normal BMI. Compared with those in need of nutritional intervention, patients not in need of nutritional intervention had lower odds for the disorders (OR = 0.109 (P value = 0.006)). Medication had increased the likelihood of electrolyte disorders by 5.5 times than with no medication (P value = 0.023). Those who had comorbid disease had 10 times likely to develop electrolyte disorders than those who did not have comorbid diseases (P value = 0.004).
Conclusion:
Electrolyte disorders were prevalent in cancer patients. Age, BMI, nutritional condition, comorbid disease, and prescribed drugs were the predictors of electrolyte disorders in cancer patients. Authors recommend routine screening of electrolyte disorders in cancer patients and special emphasis on controlling and managing risk factors.
Introduction
In 2018, there were 18.1 million new cases of cancer and 9.6 million deaths attributable to cancer; on average, there is a 20% risk of getting cancer before the age of 75 and a 10% chance of dying from it. 1 The burden of cancer in Africa is rising; there were 847,000 new cancer cases (6% of world total) and 591,000 deaths (7.2% of world total) in 2012, with three-fourth of it was in 47 sub-Saharan Africa countries. 2
In 2017, cancer incidence in Ethiopia was 108/100,000 population, and mortality was 84.5/100,000; the incidence to mortality ratio was 0.78. 3 Despite the relatively low incidence of cancer in Africa, the mortality rate is disproportionately high. Poor survival of cancer patients can be attributed to many factors including late diagnosis, unavailability of timely and standard treatment for the disease, as well as comorbidities and socioeconomic factors.
Besides the burden of cancer itself, comorbidities are an important independent prognostic factor for patients with cancer. 4 The coexistence of different chronic diseases is more common in cancer patients than the general population without cancer, hence present in 68.7% of cancer patients, and 32.6% of these individuals had ⩾2 comorbid conditions. 5 The prevalence of comorbidities has important clinical, health service, and research implications from early to the late stage of cancer. 6
Electrolyte disorders in cancer patients have important prognostic implications; 7 they appear to be the strongest predictors of mortality along with coagulopathy, and renal failure, increasing mortality in hospitalized patients with some types of cancer. 8 These disorders are said to increase morbidity and mortality by cancer and decrease the quality of life. 9 Critically ill cancer patients, patients having renal diseases, patients taking medications or in chemotherapy, and endocrine disorders associated with Syndrome of in appropriate Anti-Diuretic Hormone secretion (SIADH) were prone to electrolyte disorders.10,11
The occurrence of electrolyte disorders at the admission or during the hospitalization in cancer patients represent a significant factor influencing the outcome and length of hospitalization. Effective and timely normalization of electrolyte levels had a positive effect on prognosis, as well as on the length of stay in the hospital, thus potentially resulting in life savings. 12 For example, a higher rate of hyponatremia has a significant and independent association with longer hospital stay and higher mortality. Patients who had correction of hyponatremia in the hospital had a decreased risk of mortality. 13 Recent literature also supported correction of hyponatremia had more positive effects, including blood sodium level, length of hospital stay, hospital complications, and hyponatremia symptoms. 14 Hyponatremia has a higher economic cost and higher possibility of readmission, and it was associated with up to around $3000 higher hospital costs/patient when compared with the cost of normonatremic subjects in the United States. 15
While it is a universal notion that diagnosis and treatment of comorbidities are necessary, due emphasis is not given to electrolyte disorders in cancer patients. In some diseases, electrolytes are being used for diagnosis and follow-up, while the electrolyte disorder itself is not given enough attention so far in the study area. In this study, we assessed the magnitude of electrolyte disorders in cancer patients and determine influencing factors.
Methods
Study area, design, subjects, and tools
The study was conducted at Jimma Medical Center (JMC) found in Jimma town, southwest Ethiopia. An institution-based cross-sectional study was conducted from 1 April to 30 May 2019 on admitted cancer patients. The study was conducted on 84 consecutive admitted cancer patients in this institution. Cancer patients with an age greater than or equal to 18 years were included in this facility-based cross-sectional study. The sample size was calculated using a single population proportion formula by assuming the prevalence of hyponatremia in cancer 47%, (maximum sample size from all available literature) research conducted in the United States in hospitalized cancer patients 13 with a confidence interval of 95%, a margin of error 5%. The final sample size after applying the single population correction formula gave 84 patients.
A set of closed and open-ended questions were prepared for the sake of collecting socioeconomic and demographic data; the questionnaire was pretested before the actual data collection. Nutritional status was assessed by a questionnaire adopted from Patient-Generated Subjective Global Assessment (PG-SGA), 16 developed specifically for patients with cancer. Body mass index (BMI) was calculated after the measurement of height and weight. Moreover, Cancer patient’s substance use was assessed by Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST), 17 an eight-item screening tool developed by the World Health Organization (WHO) to detect and manage substance use and related problems. The type of cancer, the stage of cancer, the presence and absence of comorbid conditions, and the presence or absence of current medication were recorded from patent charts.
For measuring the level of serum electrolytes, HumaLyte Plus5 Ion-Selective Electrolyte Analyzer (GmBH, Germany) was used. The measurement is performed by an ion-selective electrode that has five different electrodes in the analyzer: Na+, K+, Ca2+, Cl−, and a reference electrode was used under a standard operating system.
Definitions of terms
Electrolyte disorder was defined by test results indicating an altered level of at least one of the electrolytes (potassium, chloride, sodium, or calcium level), that is, either increasing or decreasing from the normal range. The following ranges were used to determine the imbalance for each electrolyte: Na+= 135–145 mmol/L, K+= 3.5–5.5 mmol/L, Ca2+= 2.1–2.55 mmol/L, and Cl− = 98–108 mmol/L. 18
The nutritional status of subjects was classified based on the PG-SGA score. A score of greater than or equal to two was considered as in “need of nutritional intervention” and a score of less than two as “needless to nutritional intervention. 19
Substance use was classified in the following manner
No/Low risk for substance use-related problems—score for smoking and chewing is between 0 and 3 but up to10 for alcohol. 17
Moderate risk for substance use-related problems—score for smoking and chewing is between 4 and 26, but between 11 and 26 for alcohol. 17
High risk for substance use-related problems—if the score is above 27. 17
Data analysis
Data were checked, cleared, and fed into Epi-data (version 4.1) and then exported to SPSS (version 22.0) software for statistical analysis. The association of independent variables with electrolyte disorders was investigated by using bivariate logistic regression. All independent variables with a P value of ⩽ 0.25 in the bivariate logistic analysis were fitted into multiple logistic regression to identify associated factors in the final model. The degree of association was interpreted by using odds ratios (ORs) with 95% confidence interval (CI) and P ⩽ 0.05 was considered as statistically significant.
Ethical clearance was obtained from Jimma University, Institutional Review Board (IRB); written consent was obtained from each study participant.
Results
Prevalence of electrolyte disorders
The overall prevalence of electrolyte disorders was 60.7% (51 patients). In those 51 cancer patients, the disturbance occurred in at least one of the four electrolytes (Na+, K+, Ca2+, Cl−), or in two or more of those measured electrolytes. Alteration of major serum electrolytes showed in Figure 1.
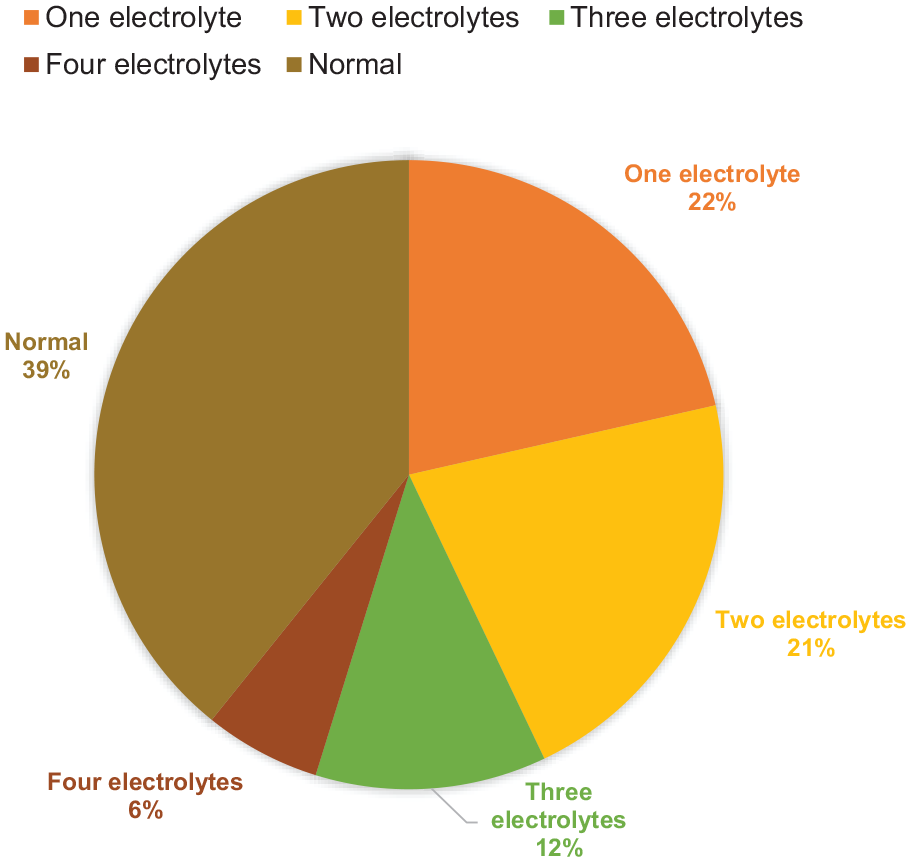
Category of electrolyte status based on the number of electrolytes altered in cancer patients admitted to JMC, 2019.
Disturbance of the serum level of each electrolyte also occurred in cancer patients. The most pronounced alteration occurred in serum level of Sodium (Na+) 40 (47.6%) followed by potassium (K+) 26 (31%), then chloride (Cl−) and calcium (Ca2+) 19 (22.6%) each, as shown in Figure 2. The frequency of serum electrolyte alteration was also analyzed in terms of increment or decrement of each electrolyte and classified as hypo and hyper according to the type of electrolyte.

Electrolyte derangements based on the type of electrolyte, in cancer patients admitted to JMC, 2019.
Influencing factors for occurrence of electrolyte disorders
To assess the association of each independent variable with the occurrence of electrolyte disorders, checking assumptions and binary logistic regression were performed. The presence or absence of comorbidity diagnosis, age, BMI, nutritional assessment, and current prescribed medication use were the candidate variables for multiple logistic regression analysis. Patient age was classified based on the quartile classification system. 20
Age was one of the candidates for multiple logistic regression. Taking the fourth quartile (>55 years) as a reference, there was a significant difference in the odds of electrolyte disorders. Generally, younger patients had significantly lower odds for electrolyte disorders (adjusted odds ratio (AOR) = 0.128 (95% CI: 0.016–0.99), P value = 0.05) and the second quartile patients had also significantly lower odds of electrolyte disorders (AOR = 0.08 (95% CI: 0.01–0.81), P value = 0.033). There was no significant difference in the odds of electrolyte disorders in the third quartile and fourth quartile (AOR = 1.50 (95% CI: 0.25–9.05), P value = 0.655).
BMI was among the factors associated with electrolyte disorders. In the final model, underweight patients had higher odds for electrolyte disorders. Compared with the normal, underweight patients had closer to threefold likelihood to develop electrolyte disorders (AOR = 3.13 (95% CI: 1.07–4.99, P value = 0.043). There was no significant difference in the odds of electrolyte disorders among those having normal BMI and overweight patients (AOR = 1.86 (95% CI: 0.37–9.33), P value = 0.451). The PG-SGA was used to assess the patient’s nutritional status, and there was a significant difference in the odds of electrolyte disorders among those who were not in need of nutrition intervention and need nutrition intervention. Compared with those in need of nutritional intervention, patients not in need of nutritional intervention had lower odds for the disorders (AOR = 0.109 (95% CI: 0.023–0.521), P value = 0.006).
Prescribed medications and comorbid diagnoses were among the factors associated with electrolyte disorders. Patients taking prescribed medications (for comorbid diagnosis treatment and for pain alleviation) had higher odds for electrolyte disorders. Medications had increased the likelihood of electrolyte disorders by 5.5 times than with no medications (AOR = 5.58 (95% CI: 1.273–24.496, P value = 0.023). The presence of comorbid diseases was an important factor associated with electrolyte disorders. Those who had comorbid diseases had 10 times the risk to develop electrolyte disorders than those who didn’t have comorbid diseases (AOR = 9.92 (95% CI: 2.051–48.00, P value = 0.004). Associated factors with electrolyte disorders are given in Table 1.
Bivariate and multiple logistic regression analysis of variables associated with electrolyte disorders among cancer patients admitted in JMC, 2019.

JMC: Jimma Medical Center; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; BMI: body mass index; PG-SGA: Patient-Generated Subjective Global Assessment.
P value ⩽ 0.25 and **P value ⩽ 0.05.
Discussion
In this study, the prevalence of electrolyte disorders was 60.7%. The value observed in the present study was higher as compared with the one observed in Turkey; comorbidity was observed in 39% of the patients. The most frequent oncological diagnoses in these patients were lung and hematological malignancies. 21 The discrepancy between the two studies might be explained by population characteristics. For example, the previous study assessed patients from the emergency department, while the current study encompassed all admitted patients in an oncology unit. The other population difference is that there was a relatively lower percentage of comorbid illness (39%) in the previous study compared with the current (46.4%). It should also be noted that the types of cancer are an important factor in the occurrence of electrolyte disorders. Despite our definition of electrolyte disorders, this figure remains high and indicates the need for intervention in this area. Other comorbidities are also present in 46.4% of the current study population.
The presence or absence of comorbid diseases, age, BMI, nutritional status, and current prescribed medication use were associated variables after multiple logistic regression analyses in this study. While there is no significant association between electrolyte disorders, and sex, income, and educational status in the current study, mortality was higher in women with shorter rather than longer education, among those with lower rather than higher income. 22 Socioeconomic differences in survival could be explained partly by cancer stage and comorbidity.
There was a significant association between age and electrolyte disorders in this study. Older age patients were found to have higher odds of electrolyte disorders. It was also previously reported that the age of 75 years or more proved to be a significant and independent predictor of a worse overall and disease-specific survival as compared with age between 65 and 74 years. 23
In this study, younger patients had significantly lower odds for sodium alteration which was in agreement with the previous report in Singapore; increasing age was a strong independent risk factor for both hypo- and hypernatremia. 24 Aging is associated with a decreased capacity to cope with environmental, disease-related, and drug-related stresses in sodium and water balance, due to reductions in total body water, thirst sensation, renal responsiveness to anti-diuretic hormone (ADH), and glomerular filtration rate. 25
There was a significant association between BMI and electrolyte disorders in this study. Underweight patients had higher odds of electrolyte disorders. Similarly, in a study conducted in the Netherlands, a lower BMI was associated with an increased risk of hypokalemia which could be explained by low dietary intake of electrolytes that may contribute to electrolyte disorders. 26
In this study, 46.4% of cancer patients had comorbid diseases. In previous studies, high comorbidity (68.7%) was present in cancer patients, and 32.6% of these individuals had ⩾2 comorbid conditions. The frequency was increased in the elderly, smokers, and those with lower socioeconomic status. Rates also appeared to vary by specific tumor sites. 5
In the present study, the presence of comorbid disease in cancer patients increases the odds (9.921 times) for electrolyte disorders. Previous studies had also found comorbidities like diabetes mellitus increase the odds (1.23 times) and hypertension (1.63 times) for the presence of at least 1 electrolyte disorder. 26 Life expectancy was strongly related to both age and the burden of chronic illness; coexisting chronic illness is associated with a substantial reduction in life expectancy after a diagnosis of cancer. 27 Moreover, an increased level of comorbidity was associated with higher all-cause mortality compared with patients without comorbid conditions. 28
The current study showed 54.8% of patients were taking medications and these medications increase the likelihood of electrolyte disorders, as found in another study. 26 The use of antipain is beneficial for cancer patients to alleviate pain but is associated with the occurrence of electrolyte disorders. Pharmacological agents that increase the synaptic concentration of serotonin, like tramadol, may induce inappropriate ADH secretion in patients who are not water-depleted. Tramadol alone may produce dilutional hyponatremia secondary to SIADH in certain individuals. 29 Non-steroidal anti-inflammatory drugs inhibit renal prostaglandin synthesis and cause various electrolyte and acid-base disturbances, including hyponatremia and hyperkalemia. 30 Besides the analgesics, several drugs that might be used for comorbid diseases might induce electrolyte disorders. 31
This study showed cancer patients taking medications had two times the risk to develop hypocalcemia compared with those patients without prescribed medications. This is in agreement with the previous study which stated that drugs like Aminoglycosides, Gentamicin, Phosphate enemas, Anticonvulsant therapy (for example, phenobarbitone, Phenytoin, and Magnesium sulfate) can cause hypocalcemia. 31 The study determines the magnitude and influencing factors in cancer patients; this study is the first of its kind in the area. With its strength, this study has limitations as well, readers should be aware of the following limitations. First, due to the cross-sectional nature of the study, it failed to infer causality. Second, despite the finding of a high prevalence of electrolyte disorders, other supposed influencing factors including the stage of cancer, patients were symptomatic or not were not elucidated in this study. Third, although hospital length of stay appeared to be well influenced by electrolyte disorders, the study failed to assess hospital length of stay. Fourth, cancer patients were taking variable types of medications which poses difficulty to compile and run analysis; the study failed to imply medication type to specific electrolyte disorder associations.
Conclusion and recommendations
Electrolyte disorders were prevalent in cancer patients. Older age group patients were prone to electrolyte disorders; patients in need of nutritional intervention were significantly associated with electrolyte disorders. Underweight, current use of medications, and having comorbid diagnosis had increased the odds for electrolyte disorders. Attention should be given to cancer patients especially for electrolyte disorders. Admitted cancer patients should be routinely screened for electrolyte disorders. Besides, cancer patients should be screened routinely for malnutrition and comorbid diseases. Special emphasis on the status of serum electrolytes should be given for cancer patients in old age, underweight, needing nutritional intervention, comorbid diseases, and taking medications.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211052861 – Supplemental material for Factors influencing the occurrence of electrolyte disorders in cancer patients
Supplemental material, sj-docx-1-smo-10.1177_20503121211052861 for Factors influencing the occurrence of electrolyte disorders in cancer patients by Addis Alem, Chala Kenenisa Edae, Endriyas Kelta Wabalo, Amare Abera Tareke, Almaz Ayalew Bedanie, Wondu Reta, Moyeta Bariso, Gadisa Bekele and Belay Zawdie in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledge Jimma University for funding this study.
Author contributions
Chala Edae made substantial contributions to conception and drafting the manuscript. Addis Alem performed collecting, analyzing, and interpreting the data. Belay Zawdie and Endriyas Kelta were major contributors in writing the manuscript. Amare Abera, Almaz Ayalew Bedanie, Wondu Reta, Moyeta Bariso and Gadisa Bekele revised the manuscript critically. All authors read and approved the final manuscript.
Availability of data and materials
The data set supporting the conclusion of this article can be found from the corresponding author with reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from Institutional Review Board (IRB) of Jimma University, with approval number IHRPG/556/2019.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Jimma University (grant No. 551/2011).
Informed consent
Written informed consent was obtained from all participants before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.